@mandeep_mayo Wire, aspiration with penumbra, 2b3a and if still no flow then IC TPA, once flow is established then will anti-coagulate for 24-48 hours before relooking. Interesting case and thank you for sharing, would love to know your thoughts!
2 new 🔥 off the press papers
1️⃣ How to perform coronary endo and micro fx assessment in cath lab @MuhammadAjmalMD@DrArgyle 👇
https://t.co/Mg2sViGdrI
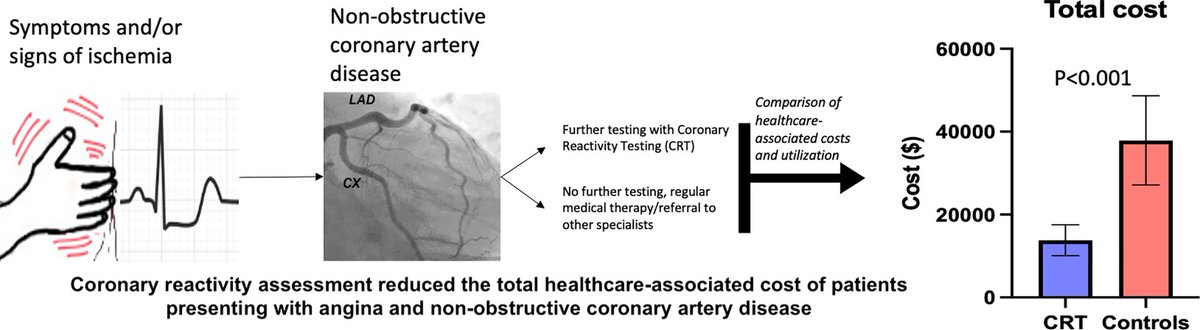
2️⃣ Assessment of coronary micro & endo function ⬇️ downstream healthcare cost by ~25k/pt in 2 yrs!
https://t.co/hjujOxxH0a
@mandeep_mayo Upfront hemodynamic support, aspiration, no reflow meds, ivus, if disease then stent and if no disease then continue with DAPT, IV anticoagulation for atleast couple days with hemodynamics support and monitoring in the ICU, unfortunately no best option.
Join us Monday 3/6 @ 8:30 AM for Highlighted Original Research: Interventional and Structural - Top #ACC23 Abstracts
Coronary reactivity testing for endothelial and microvascular dysfynction reduces healthcare-associated cost in #ANOCA
Almost 4 decades ago, Andreas Gruentzig described "the ideal catheter" to me. He foresaw the development of FFR, hi-pressure balloons, aspiration catheters, stents, & more. His thoughts on physiologic measurement both during & post-procedure are thought-provoking. #AngioHistory
Excellent point from the REVIVED editorial: pts with the most severe CAD were likely referred to CABG as a GDMT arm wouldn't have been ethical. A PCI vs CABG strategy would have overcome this limitation but would have required more pts and longer FU.