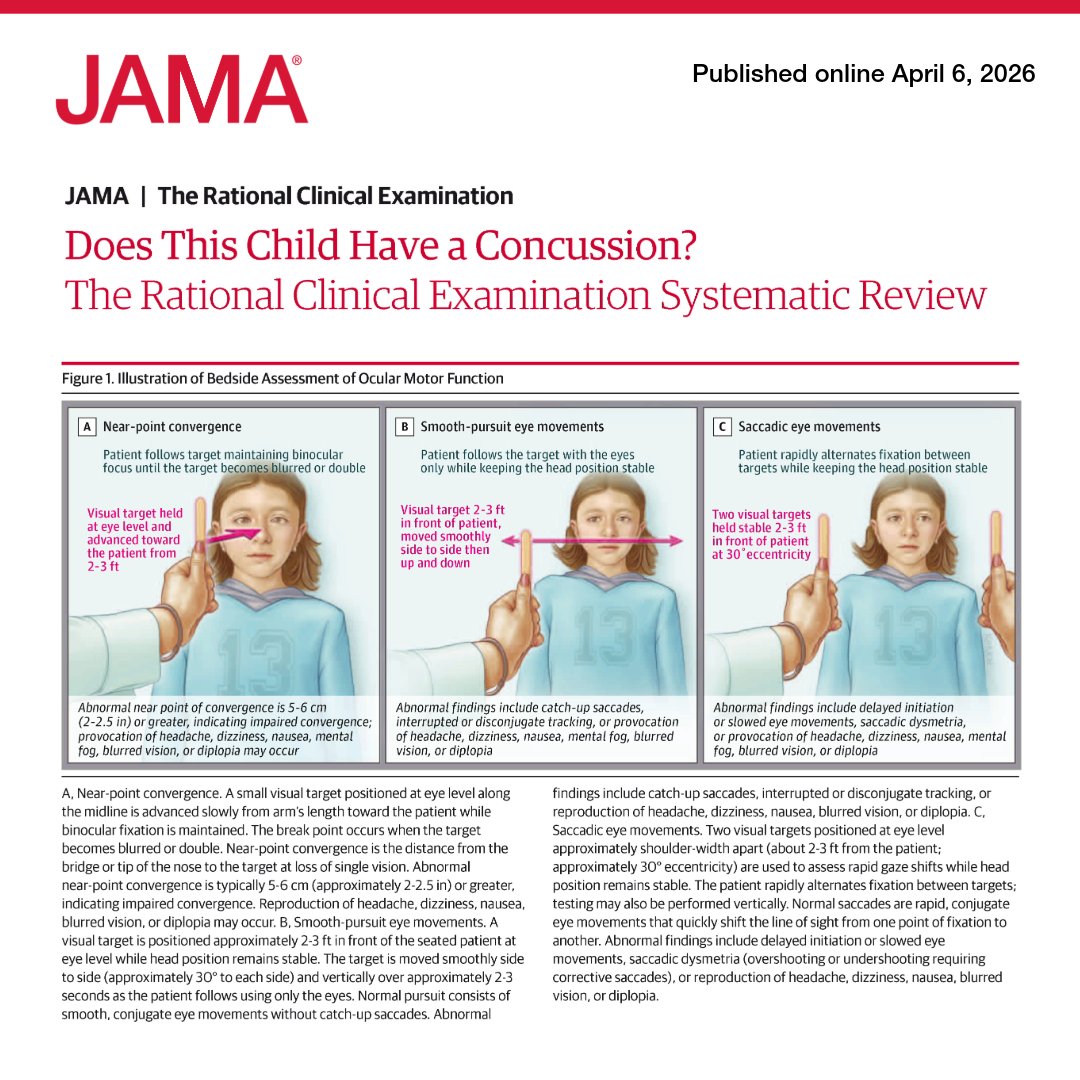
An estimated 1.1 million to 1.9 million #pediatric concussions occur annually in the US.
📊 This JAMA Rational Clinical Examination reviews the diagnostic accuracy of symptoms and signs observed in the initial evaluation of a child or adolescent who may have had a #concussion.
https://t.co/pCEhjaAoI2
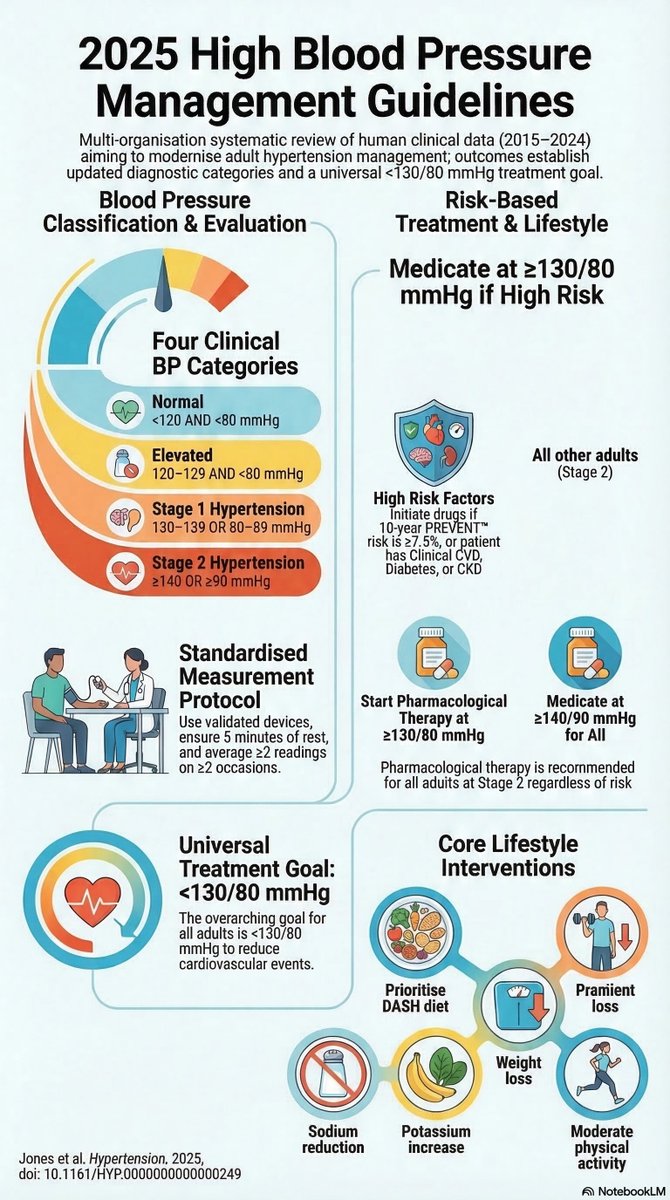
📊 JAMA Clinical Guidelines Synopsis: The 2025 ACC/AHA guideline recommends home and office #BloodPressure monitoring to confirm diagnosis and titrate medications, with a target blood pressure of <130/80 mm Hg for most adults.
https://t.co/PSVJGLesbs
#Rhinoplasty remains one of the most debated—and difficult to teach—procedures in plastic surgery. In @PRSJournal, 4 senior surgeons share a practical framework for balancing preservation and structural techniques.
Read more: https://t.co/9DulraR7ju
@Dr_SamuelLin
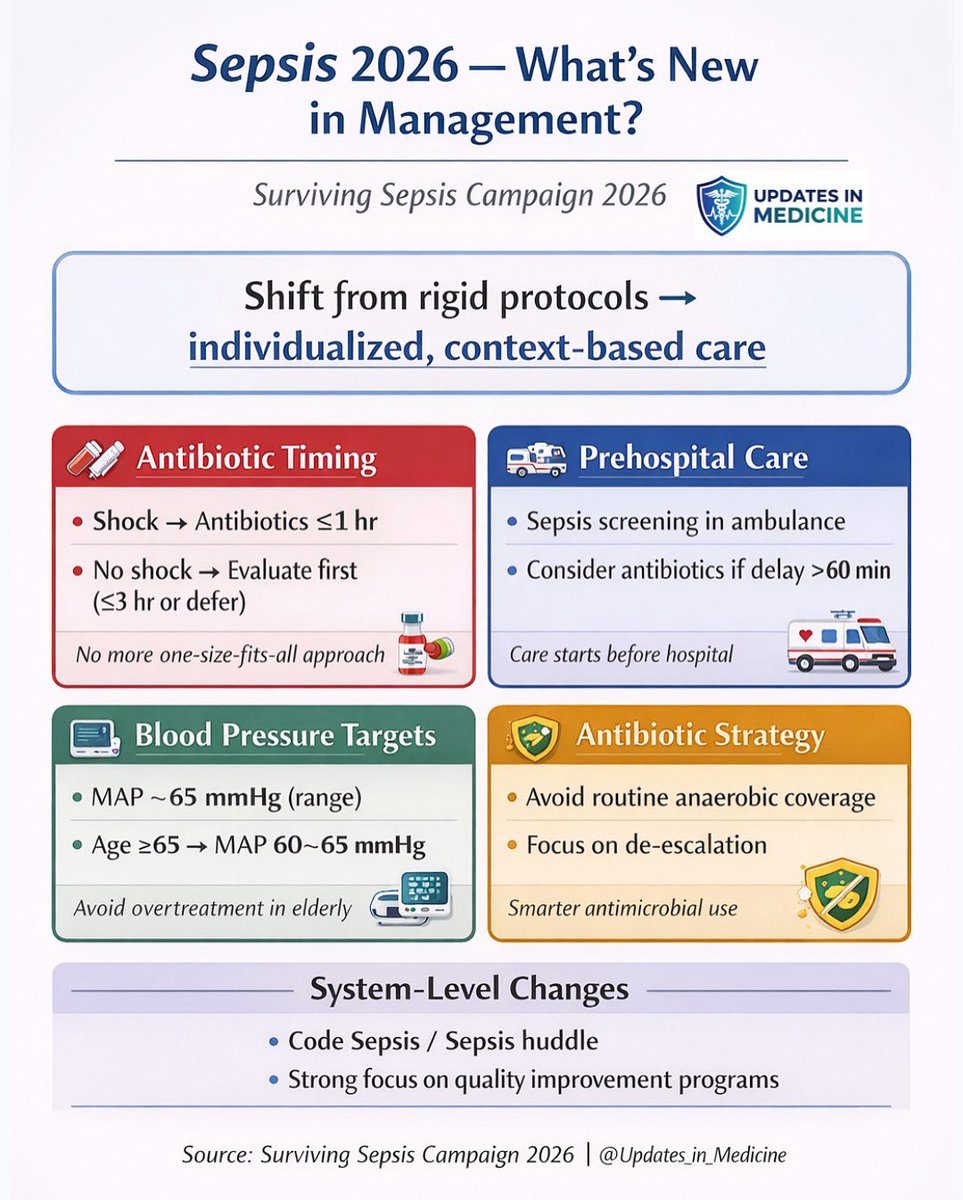
📊 JAMA Clinical Guidelines Synopsis: The newly released Surviving #Sepsis Campaign guidelines from ESICM and SCCM endorse early broad-spectrum antibiotics, rapid fluid resuscitation, and deescalation strategies for adults with sepsis or septic shock.
https://t.co/AVBfkuij0j
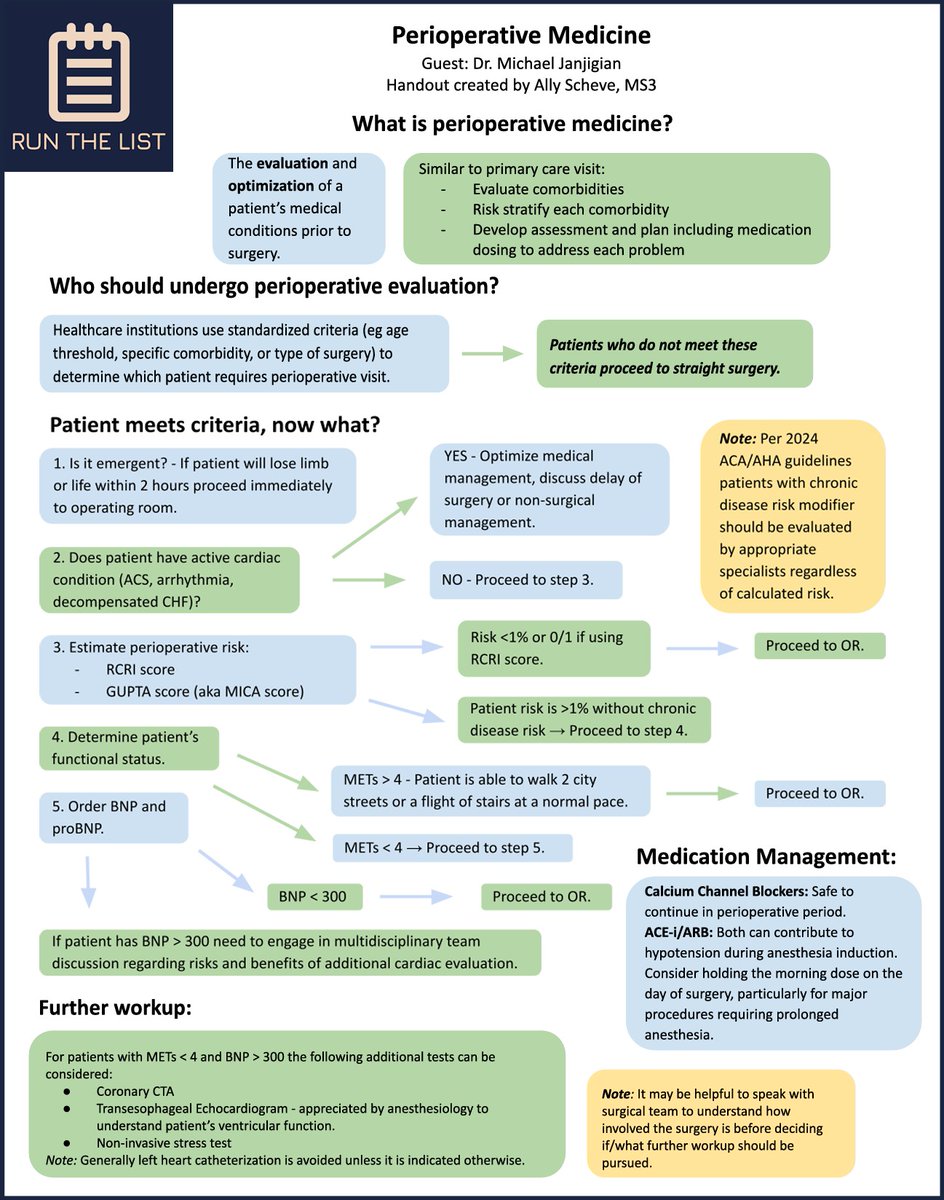
We are so lucky to have another RTL handout by Ally Scheve for "Perioperative Medicine" with links to the episode below!
iTunes: https://t.co/lSN2sjH0kA
Spotify:
https://t.co/JrIIx8f1bP
#meded#medtwitter
Surviving Sepsis Campaign 2026 Guidelines - Summarised
Some key thoughts got my attention
- Pre hospital antibiotics
- Code Sepsis/ Sepsis Huddle
- No empirical anaerobic or antifungal coverage in sepsis/septic shock unless at high risk for such infections
- Initiating Vasopressors through peripheral line
- Emphasis on De-resuscitation
- Arterial lines if required
- Insufficient evidence for Methylene Blue and Midodrine (gonna change for sure in the following guidelines)
- HFNC over NIV in hypoxemic respiratory failure
Do like and share if you find them useful!
#Sepsis #Septicshock #Survivingsepsiscampaign
JUST RELEASED!
The 2026 Update of the Surviving #Sepsis Campaign Guidlines is now online!
Permanent Free Access
Adult: https://t.co/Noup1PiXmZ
Children: https://t.co/zN6pifl8FT
🧬🫀 Lipoprotein(a) meets Calcium Score: are we finally refining risk?
This large multicohort study tackles a clinically frustrating question:
👉 What do we do with elevated Lp(a) when risk is still uncertain?
🔍 Core idea
Lp(a) is a genetically driven, causal risk factor for ASCVD.
But in practice:
⚠️ Risk remains heterogeneous
⚠️ Treatment pathways are still evolving
⚠️ Not all patients with high Lp(a) behave the same
📊 What this study shows
Adding Coronary Artery Calcium (CAC) dramatically improves risk stratification:
✅ High Lp(a) + high CAC → clearly elevated risk
✅ High Lp(a) + CAC = 0 → surprisingly lower short-term risk
👉 In other words:
Lp(a) = potential risk
CAC = realized disease
🧠 Why this matters
We often treat Lp(a) as a binary “on/off” risk signal.
This paper reinforces a more nuanced model:
💡 Risk is not just biology (Lp(a))
💡 It’s the interaction between biology + plaque burden
⚖️ But here’s the catch
Population-level conclusions can mislead:
CAC = 0 does NOT mean “no risk”
It may simply reflect earlier disease stage
Especially relevant in younger patients with high Lp(a)
👉 Time horizon matters.
🔮 Clinical takeaway
This is where imaging becomes decisive:
✔️ Use CAC to contextualize Lp(a)
✔️ Avoid over- or under-treatment
✔️ Move toward precision prevention
🚨 Bottom line
Lp(a) tells you who might be at risk
CAC tells you who already is
The future is not choosing between them—
👉 it’s integrating both intelligently