Clinical Research Fellow in Electrophysiology and Imaging, King’s College London. Cardiology Reg and Aspiring EP, board game enthusiast, vegan, cancer survivor
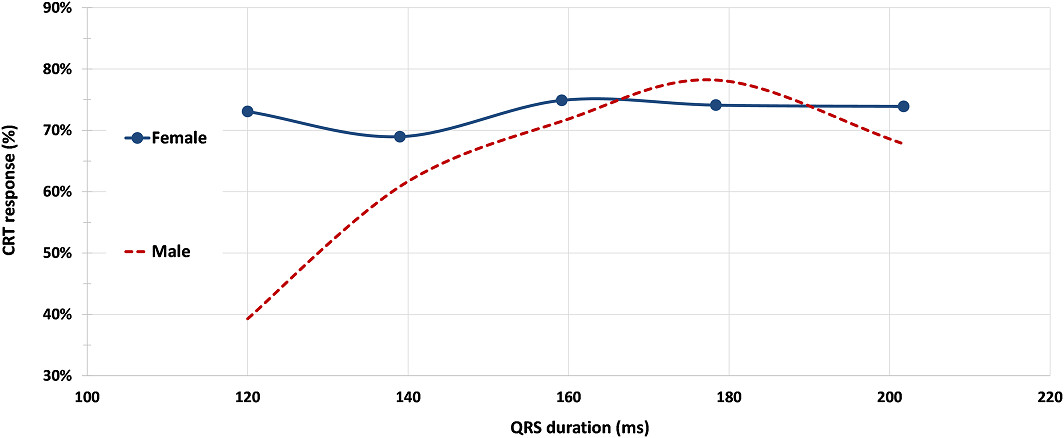
Really pleased to put this out there - should we be using sex-specific CRT eligibility criteria? #epeeps
Heart Size Difference Drives Sex‐Specific Response to Cardiac Resynchronization Therapy: A Post Hoc Analysis of the MORE‐MPP CRT Trial | JAHA https://t.co/NStzyix1GB
… what’s a physician again??
is this not just straight up misleading and lying what’s happening 😭😭😭
literally ask any general member of the public and they won’t have a clue who these ppl are - this is shady and how ppl still don’t think this is a bad idea is tapped ‼️
@PurumittalDr What was the mode of arrest? VF/monomorphic VT? Was the first presentation with chest pain and ischaemic changes? If not an STE-ACS is there a place for CMR, then ICD, GDMT, and revasc following optimisation if there are symptoms? No critical LMS disease
@jdrwilcox PGY-12 for me, about 4.5 years left! Tbh I think there’s something to having “life experience” unrelated to the job, I’ve found personally that certain things in my personal life have made me a better dr, eg having health issues myself, dealing with tragedy, having kids
@narrowQRS Such a great video! I’ve been in research for a couple of years and nowhere near the lab but this brought it all back so succinctly with great example traces
@ecgandrhythmRoe I think focal AT from the left. Would give adenosine in the first instance to confirm that it’s not typical flutter, but given the history it’s likely related to the myxoma
@Hragy He had angina at one point now requiring BB. Would be reasonable to offer PCI or OMT and inform that PCI is mainly for symptom relief/coming off BB. He has aggressive CAD so would save the LIMA for when he is in his 60s and possibly has multivessel disease at that stage
@EhdaieMd Paced morphology of S2 different to S1. Retrograde activation seems identical throughout. My theory - the S1 beats are fusion with intrinsic rather than pure RV. So fast pathway is refractory for those beats hence retrograde slow. S2 - fast pathway is not refractory
@jdrwilcox@LKoliastasis@panosxap@PCRonline Once he’s on the table in the first place, I think most would treat any low hanging fruit. Trouble is, can’t see any in this case, not a clear STEMI, his LVEF was almost certainly impaired to begin with rather than as a result of ACS given angio findings