The @ukmedschools clinical academic survey shows the UK has lost 1/4 of early-career doctors working as medical academics in just one year.
Medical academic staff committee co-chairs @DocStrain and @gibb_jonathan say this sharp fall will have a knock-on effect on public health and economic growth:
https://t.co/ACqyYuWOBG
MTX: SC vs Oral? Metanalysis of 9 RCTs, 974 RA pts. Compared w/ oral, SC MTX signif. incr odds of ACR20 (RR=1.15), ACR50 (RR=1.14) & reduced GI adverse events (RR=0.58), diarrhea (RR=0.42): BUT no difference in ACR70, DAS28-ESR, bioavailability AUC, or other AE https://t.co/jE9xwSl6Y2
𝗔𝗹𝗹𝗼𝗽𝘂𝗿𝗶𝗻𝗼𝗹
◦ According to 2016 updated EULAR evidence-based
recommendations for the management of #gout, in patients with normal kidney function, #allopurinol is recommended for first-line #urate-lowering therapy, starting at a low dose (100 mg/day) and increasing by 100 mg increments every 2–4 weeks if required up to the maximum allowed dosage (600-800 mg/d), to reach the uricemic target (serum uric acid levels <6 mg/dL, in case of tophaceous gout <5 mg/dL).
◦ If the serum uric acid target cannot be reached by an appropriate dose of allopurinol, it should be switched to #febuxostat 80 mg/d (can be increased up to 120 mg/d) or a #uricosuric, or combined with a uricosuric.
◦ Febuxostat or a uricosuric are also indicated if allopurinol cannot be tolerated.
◦ Alternative treatments in refractory cases:
- Probenecid 250 mg (one-half of a 500-mg tablet) two times a day for about one week, then 500 mg (one tablet) two times a day for a few weeks
- Lesinurad 200 mg once a day in the morning (maximum dose)
- Pegloticase 8 mg via IV infusion every 2 weeks
*Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. 2017;76(1):29-42.
🔗https://t.co/wXB73ZeFyY
A post-hoc analysis of the RITAZAREM trial evaluated the risk factors for relapse in patients with #ANCA-associated #vasculitis (AAV) who achieved remission after reinduction with #rituximab and #glucocorticoids. The study analyzed two distinct phases: the maintenance phase (months 4–24, on rituximab or #azathioprine) and the off-treatment phase (months 24–48, after stopping maintenance therapy).
𝗠𝗮𝗶𝗻 𝗥𝗲𝘀𝘂𝗹𝘁𝘀
◦ Overall: 170 patients were included. There were 99 relapses total, of which 46 occurred during maintenance therapy.
𝗥𝗶𝘀𝗸 𝗙𝗮𝗰𝘁𝗼𝗿𝘀 𝗯𝘆 𝗧𝗿𝗲𝗮𝘁𝗺𝗲𝗻𝘁 𝗣𝗵𝗮𝘀𝗲
𝘿𝙪𝙧𝙞𝙣𝙜 𝙈𝙖𝙞𝙣𝙩𝙚𝙣𝙖𝙣𝙘𝙚 𝙏𝙝𝙚𝙧𝙖𝙥𝙮 (𝙤𝙣 𝙞𝙢𝙢𝙪𝙣𝙤𝙨𝙪𝙥𝙥𝙧𝙚𝙨𝙨𝙞𝙤𝙣):
◦ Musculoskeletal involvement at baseline → significantly increased relapse risk (OR 2.8, 95% CI 1.1–7.2).
◦ Higher patient global assessment (patient-reported disease activity) → associated with increased relapse risk (OR 1.1 per unit increase).
◦ Multivariable analysis also linked markers of inflammation (changes in platelets, white blood cells, and IgA levels) with higher relapse risk.
𝘿𝙪𝙧𝙞𝙣𝙜 𝙊𝙛𝙛-𝙏𝙧𝙚𝙖𝙩𝙢𝙚𝙣𝙩 𝙋𝙝𝙖𝙨𝙚 (𝙖𝙛𝙩𝙚𝙧 𝙨𝙩𝙤𝙥𝙥𝙞𝙣𝙜 𝙢𝙖𝙞𝙣𝙩𝙚𝙣𝙖𝙣𝙘𝙚):
◦ Presence of CD19+ B cells → associated with higher relapse risk (OR 2.5, 95% CI 1.2–5.1).
◦ Reappearance of ANCA (anti-proteinase-3 or anti-myeloperoxidase) → strongly associated with relapse (OR 3.2, 95% CI 1.3–7.7).
𝗖𝗼𝗻𝗰𝗹𝘂𝘀𝗶𝗼𝗻 𝗼𝗳 𝘁𝗵𝗲 𝗦𝘁𝘂𝗱𝘆
Risk factors for relapse in AAV are phase-dependent. During active maintenance therapy, clinical factors (musculoskeletal disease and patient-reported activity) and non-specific inflammatory markers predominate. After treatment withdrawal, immune reconstitution (return of B cells) and ANCA reappearance become key predictors.
𝗖𝗹𝗶𝗻𝗶𝗰𝗮𝗹 𝗜𝗺𝗽𝗹𝗶𝗰𝗮𝘁𝗶𝗼𝗻
Monitoring B-cell recovery, ANCA status, and inflammatory markers (especially after stopping therapy) can help identify patients at higher risk of relapse and guide personalized decisions on treatment duration or closer surveillance.
*Romich E, Baker JF, Riley TR 4th, et al. Risk Factors for Relapse in Antineutrophil Cytoplasmic Antibody-Associated Vasculitis Among Patients With Relapse After Induction of Remission With Rituximab. Arthritis Rheumatol. 2026;78(5):1134-1144.
🔗https://t.co/WIxeimIHma
#Myositis mimics are a regular challenge encountered in clinics, and critically important for our patients.
A real pleasure working with #neurology colleagues on this—highlighting practical #guidance that is especially useful for new consultants : https://t.co/9tz8KTwPXa
Subclinical interstitial lung disease (ILD) is common in #rheumatoid#arthritis (RA), affecting approximately 18–60% of patients (roughly 25% in prospective screening studies), compared to only about 10% with clinically significant RA-ILD. Some patients with subclinical RA-ILD progress to symptomatic disease, which carries increased morbidity and mortality.
Risk factors for subclinical RA-ILD include:
◦Demographic: older age, male sex, and smoking.
◦RA-specific: higher disease activity (elevated CRP/ESR, higher DAS28), and seropositivity (RF and anti-CCP antibodies). No clear link with methotrexate use or RA duration has been established.
Associated biomarkers: MUC5B promoter variant, MMP-7, PARC (pulmonary and activation-regulated chemokine), and surfactant protein D.
The optimal management of subclinical RA-ILD remains unknown, with no prospective trials or specific guidelines available. ACR/CHEST guidelines for clinical RA-ILD conditionally recommend mycophenolate, azathioprine, rituximab, tocilizumab, or cyclophosphamide as first-line options and advise against methotrexate, leflunomide, TNF inhibitors, and abatacept; however, they do not address subclinical disease.
Early identification and intervention in subclinical RA-ILD represent an important area for future research to potentially prevent progression to clinically significant ILD.
*From: Ormsby AL, Matson SM, Griffith MR, Demoruelle MK, Lee JS. Subclinical Interstitial Lung Disease in Rheumatoid Arthritis: Implications for Early Detection and Management. Chest. 2026 Apr;169(4):1018-1025.
🔗https://t.co/bkCmL7MABJ
There is probably no established treatment regimen specifically for #rheumatoid#arthritis (RA) patients who predominantly present with #tenosynovitis, and general guidelines are generally followed. Tenosynovitis is not even considered a physical examination finding that should be noted individually, as is done with the count of tender and swollen joints, despite being highly prevalent in RA, even from early stages of the disease, and having prognostic implications.
Ultrasound-assessed tenosynovitis has been shown to predict the development of erosive joint damage in early RA patients, representing a potential imaging biomarker. The tendons most frequently involved in RA are the extensor carpi ulnaris (ECU), tibialis posterior tendon, and the finger flexor tendons of two to four fingers. Patients with ECU tenosynovitis develop more erosive changes in the nearby ulna and triquetrum, suggesting that tenosynovitis may be directly involved in the pathophysiology leading to erosive disease.
Although there are no specific recommendations for patients with established RA who predominantly present with tenosynovitis, there is evidence that clinically suspected arthralgia patients with multiple sites of tenosynovitis, with or without osteitis, respond better to methotrexate during the first year (TREAT EARLIER trial).
All of the above suggests that tenosynovitis should be given greater consideration as an important prognostic factor in therapeutic decision-making for RA, and that patients who predominantly present with tenosynovitis should perhaps be considered a specific subtype with a higher risk of erosive disease and a need for earlier, more aggressive treatment.
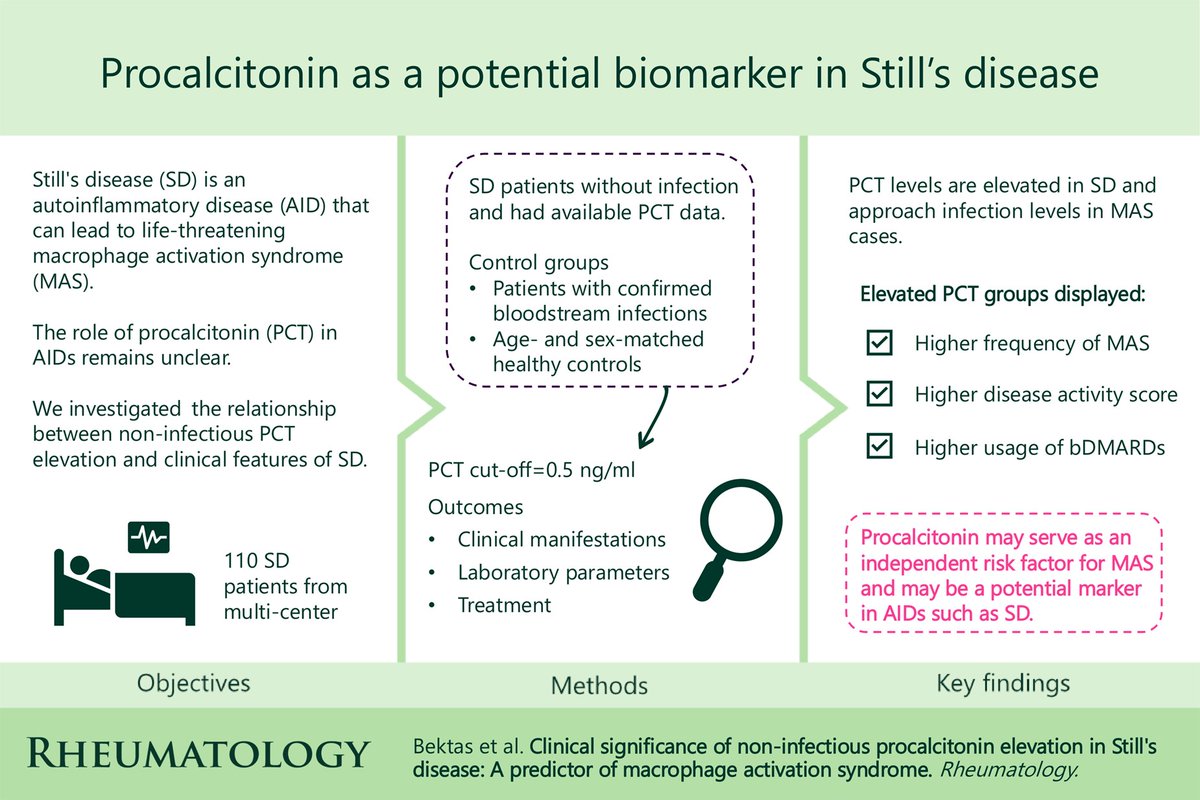
#Procalcitonin (PCT) may be a potential inflammatory marker in the course of Still’s disease (SD), as demonstrated by a retrospective study that included 110 patients with SD and absence of infection:
◦ PCT levels were significantly higher than in healthy controls and nearly as high in macrophage activation syndrome (MAS) cases as in confirmed infections.
◦ 32% had baseline PCT ≥0.5 ng/ml; 43% had peak PCT ≥0.5 ng/ml.
◦ Elevated PCT (≥0.5) was strongly linked to:
- Higher frequency of MAS
- Higher mPouchot scores
- Greater use of biologics (especially anakinra)
- Laboratory signs of severe inflammation (thrombocytopenia, ↑ AST/LDH/CRP/ferritin, ↓ albumin)
◦ MAS risk was independently increased:
- ~4.3-fold (baseline PCT ≥0.5)
- ~5.4-fold (peak PCT ≥0.5), after multivariate adjustment
◦ PCT normalized with immunosuppressive treatment.
Although PCT cannot be used to distinguish active SD from infection, these findings suggests that increased PCT levels in patients with SD are associated with a severe inflammatory response. PCT may also serve as a potential independent predictor of MAS and could be considered a convincing marker in the assessment of non-infectious inflammation.
*Bektas E, Uludogan BC, Firlatan Yazgan B, et al. Clinical significance of non-infectious procalcitonin elevation in Still's disease: a predictor of macrophage activation syndrome. Rheumatology (Oxford). 2026;65(2):keaf575.
🔗https://t.co/ENd2yobI4B
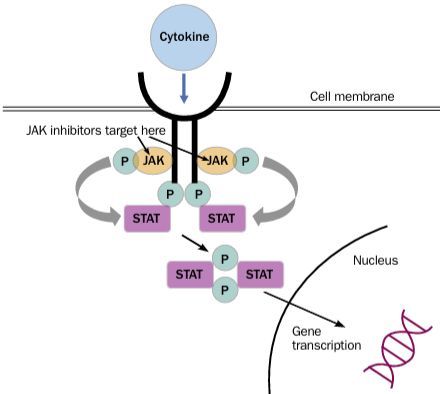
Full read review of JAK inhibitors. JAK inhibitors have a reasonably rapid onset of action and a short half-life, which facilitates management of any adverse effects. The half-life of Tofacitinib, Baricitinib & Upadacitinib is 3 hrs, 13 hrs. & 9-14hrs. https://t.co/QfQHXAPX7N
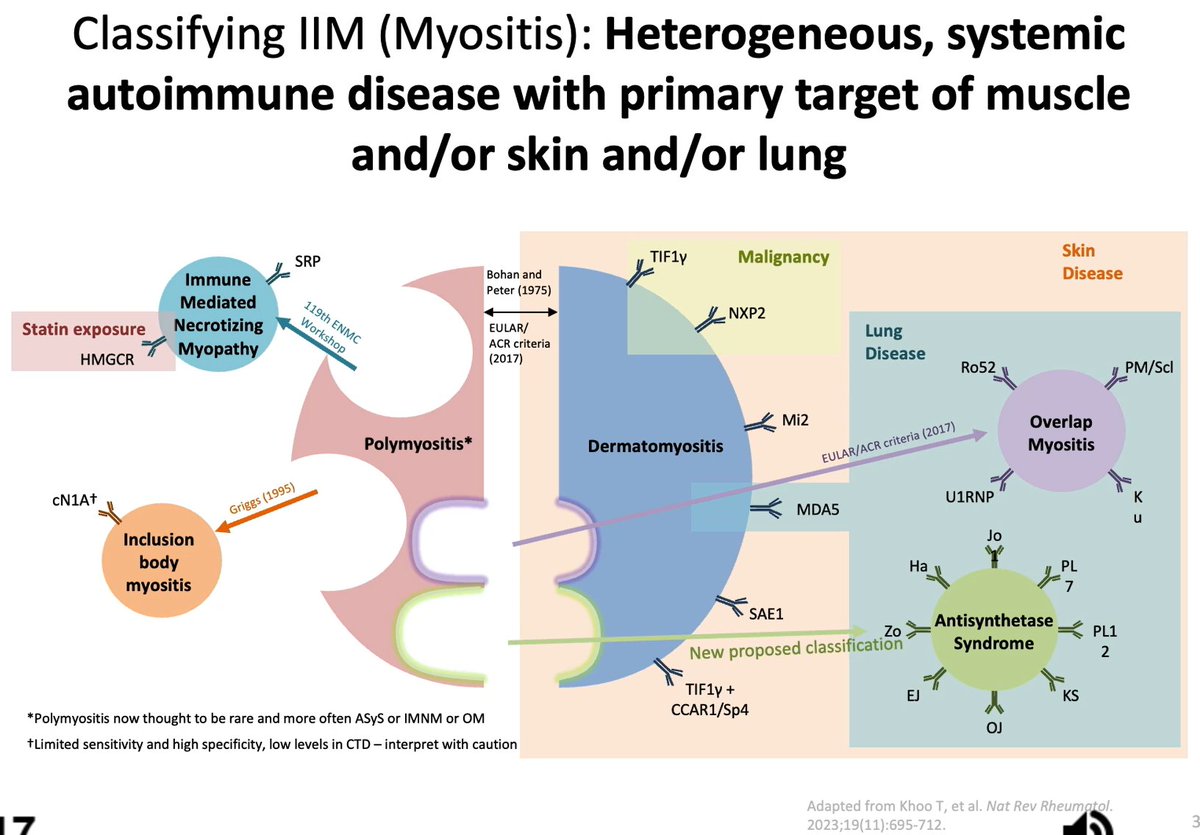
My new favorite myositis specific antibodies slide, c/o Dr. Rohit Aggarwal
Highlights the re-classification of prior cases of "polymyositis"
Covers nuance with CCAR1 & TIF1y pts (ie low risk of +CCAR1)
HJighlights lung cases (ie MDA5, overlaps, antisynthetase) #RNL26
New this week in Arthritis & Rheumatology:
Single-cell RNA-seq study of epithelial & immune cell populations in RA-ILD lungs
https://t.co/rpLO34Fqcd
Single-cell RNA-seq study of blood & synovial fluid in early oligoarthritis & enthesitis-related arthritis
https://t.co/mKsjMMw99B
Notes From the Field: Ethical principles & standards for phase III/IV ULT clinical trials
https://t.co/7DaPfxUjS3
Notes From the Field: Best practice approaches & common methodologic pitfalls when using large databases
https://t.co/bulCZ4Ef9o
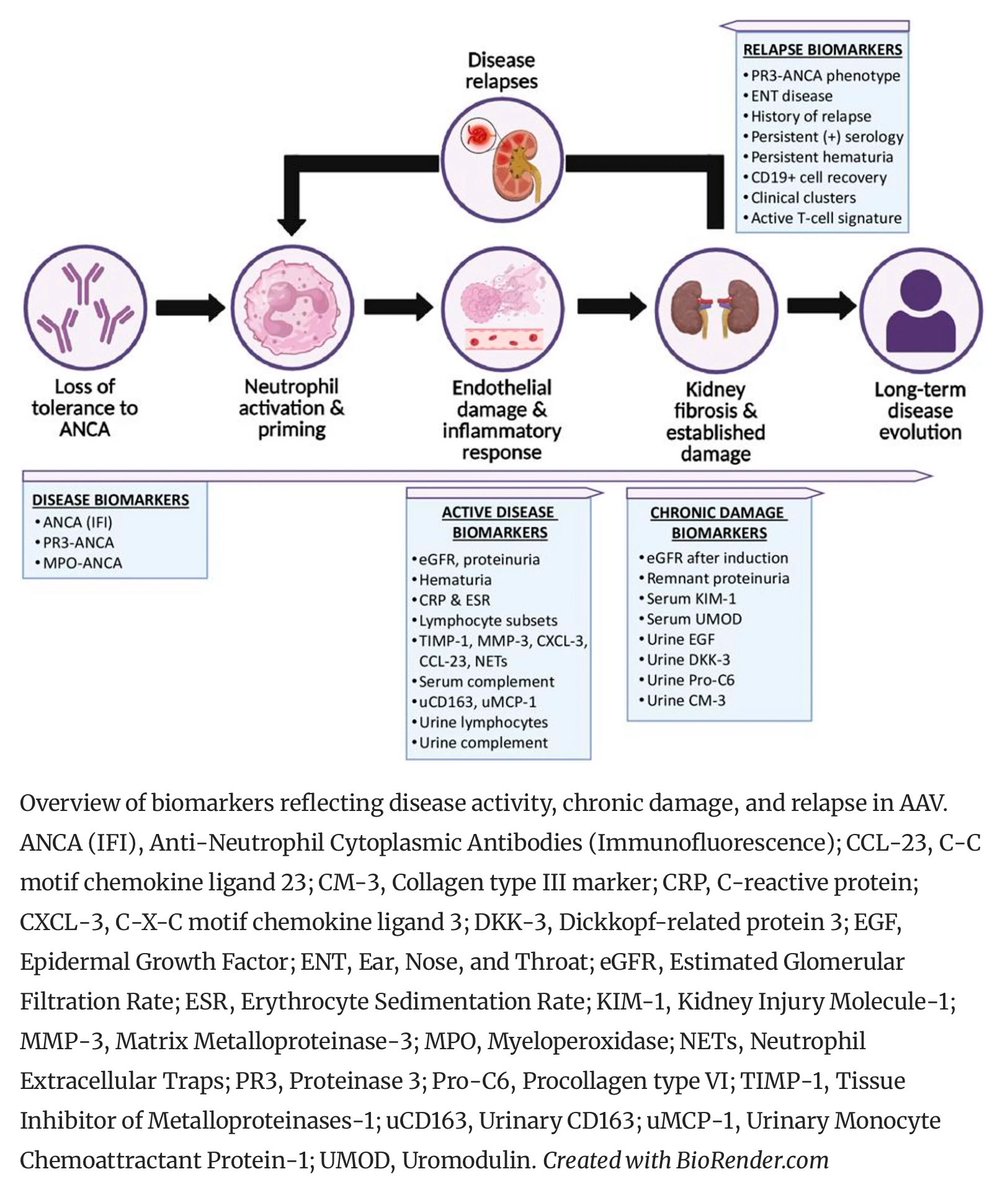
#Renal involvement is a key driver of morbidity and mortality in #ANCA-asssociated #vasculitis (AAV). Pathogenesis involves endothelial injury, complement activation, NETosis, and dysregulated immunity, leading to glomerular and tubulointerstitial damage. Distinguishing active inflammation from chronic damage remains challenging, underscoring the need for reliable tools to assess disease activity and predict long-term renal outcomes.
Current evaluation relies on clinical parameters, serum creatinine, proteinuria, and ANCA titers—imperfect surrogates for renal inflammation. Renal biopsy remains the gold standard for assessing activity and chronicity, with histopathological classifications providing prognostic value, though it is invasive and may not capture dynamic injury or repair.
Urinary #biomarkers (from tubular cells, podocytes, and immune pathways) offer promise as non-invasive markers of renal involvement, but studies are limited by small cohorts, heterogeneous definitions, and lack of standardized assays.
Future advances require integrating urinary biomarkers with histopathological and clinical data for precise activity assessment. Large, longitudinal, multicenter studies are needed to validate biomarker panels that differentiate activity from chronic damage, guide treatment, and monitor response. Combining validated urinary biomarkers with biopsy findings could enable precision medicine in AAV, improving prognostication, minimizing toxicity, and enhancing outcomes.
📸 Overview of biomarkers reflecting disease activity, chronic damage, and relapse in AAV.
*From: Mejía-Vilet, J.M., Alba, M.A. & Hinojosa-Azaola, A. The Assessment of Disease Activity and Renal Prognosis in AAV – The Contribution of Urinary Biomarkers and Renal Biopsy. Curr Rheumatol Rep 28, 1 (2026).
🔗https://t.co/MyMimEl07Z
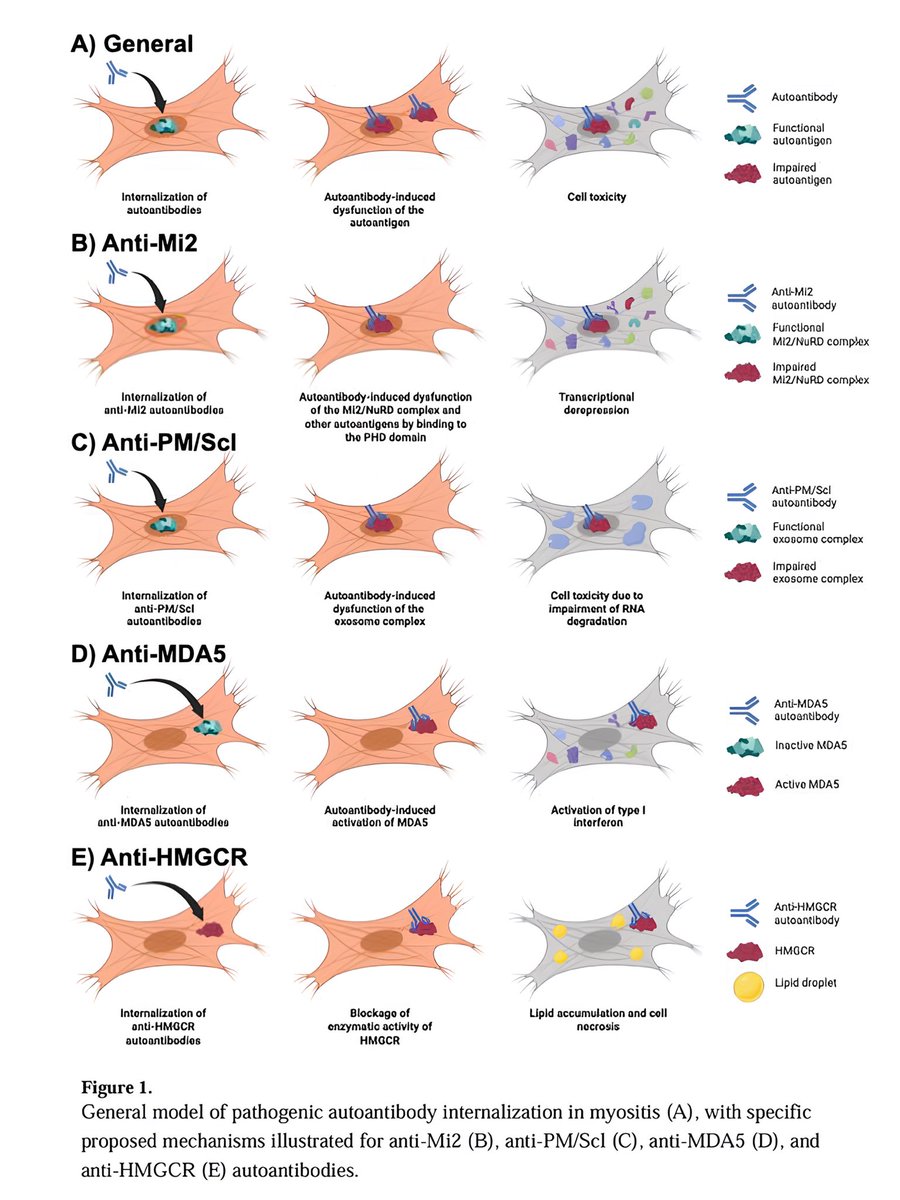
Emerging evidence supports a novel model in #myositis where #autoantibodies (particularly anti-Mi2, anti-MDA5, anti-HMGCR, and anti-PM/Scl) enter live skeletal #muscle cells, disrupt target antigen function, and cause damage—distinct from traditional type II/III hypersensitivity. Patient-derived autoantibodies induce transcriptomic and histopathological changes in cultured myoblasts that mimic patient biopsies, though evidence is lacking for anti-NXP2 and anti-TIF1γ groups, and in vivo internalization mechanisms remain unknown.
Future research should examine effects on other muscle-resident cells (e.g., endothelial, fibroblasts, immune cells), test in vivo models, and investigate entry mechanisms (e.g., Fc receptor dependence).
Implications for idiopathic inflammatory #myopathies:
• Supports quantitative and potential functional autoantibody assays for diagnosis, prognosis, and therapy monitoring.
• Suggests B cell/immunoglobulin depletion as effective for muscle involvement.
• Indicates therapies restoring target antigen function may be beneficial.
This internalization model may extend to other #autoimmune diseases with autoantibodies targeting intracellular antigens (e.g., certain neurologic disorders, systemic sclerosis, SLE, ANCA-associated vasculitis), warranting further cell-based and in vivo studies.
*From: Kirou RA, Pinal-Fernandez I, Mammen AL. Autoantibody internalization in myositis skeletal muscle: Emerging evidence, mechanistic insights, and therapeutic relevance. Autoimmun Rev. 2025 Nov 25:103962.
🔗https://t.co/lX8HsFfIi5