1/I always say you can tell a bad read on a spine MR if it doesn’t talk about lateral recesses.
What will I think when I see your read? Do you rate lateral recess stenosis?
Here’s a thread on lateral recess anatomy & a grading system for lateral recess stenosis
Most anticoagulation mistakes in stroke happen because we ask:
Which anticoagulant should I use?
before asking:
Does this stroke even deserve anticoagulation?”
Stroke anticoagulation is not a prescription.
It is AIR TRAFFIC CONTROL.
Every stroke subtype is a different aircraft.
And every aircraft does NOT get runway clearance.
🟢 GREEN RUNWAY
These are thrombin-rich strokes.
✔ AF-related stroke
→ DOAC usually preferred
✔ Mechanical valve
→ Warfarin only runway
✔ Rheumatic MS + AF
→ Warfarin tower
✔ LV thrombus
→ Usually 3–6 months
✔ Cerebral venous thrombosis
→ Heparin first, even if venous hemorrhagic infarct exists
✔ APS-related stroke
→ Warfarin dominates
✔ Cancer/NBTE stroke
→ LMWH often preferred
These are not aspirin diseases.
🟡 YELLOW HOLDING PATTERN
Not every AF stroke should receive immediate anticoagulation.
Before takeoff:
• How big is the infarct?
• Any hemorrhagic transformation?
• BP controlled?
• Platelets safe?
• Mass effect?
• ICU instability?
• Post-thrombectomy status?
ELAN and OPTIMAS changed the conversation:
Small stable infarct?
Earlier DOAC may be safe.
Large infarct?
Delay may save the brain.
Timing is neuroimaging plus judgment.
Not calendar mathematics.
🔴 RED NO-FLY ZONE
Do NOT empirically anticoagulate:
Lacunar stroke
Atherosclerotic stroke
Most ESUS
Routine AIS <48h
Infective endocarditis embolic stroke
NAVIGATE-ESUS and RE-SPECT ESUS reminded us:
“Cryptogenic” is not a license for DOAC.
🚨 WHEN BLEEDING HAPPENS
The first drug is not PCC.
The first drug is:
STOP.
Then:
→ CT brain
→ INR / renal function / platelets
→ Identify last dose
→ Reverse selectively
→ Reassess mechanism
Because the hardest question in stroke anticoagulation is not:
What should I start?
It is:
When should I restart?
AHA/ASA.
ELAN.
OPTIMAS.
Modern CVT guidance.
The era of one anticoagulation rule for all strokes is over.
Treat the mechanism.
Not just the MRI.
#Neurotwitter #Medtwitter #Stroke #Anticogulation
Antiplatelet therapy after stroke is not:
Aspirin for everyone.
DAPT for everyone.
Or clopidogrel because the patient had a stroke on aspirin.
It is a 3-question decision.
What is the mechanism?
What is the clock?
What is the bleeding risk?
That is the whole game.
Minor non-cardioembolic stroke or high-risk TIA, early presentation, low bleeding risk?
Think short DAPT.
Aspirin plus clopidogrel.
Usually 21 days.
Then single antiplatelet.
Not 3 months by habit.
Not lifelong because the first prescription was never reviewed.
Mild to moderate stroke or high-risk TIA with selected high-risk features?
Ticagrelor plus aspirin may enter the discussion.
But it is not simply stronger clopidogrel.
It is a selected-patient decision, with bleeding and dyspnoea on the other side of the scale.
Severe symptomatic intracranial stenosis?
This is the 90-day exception.
Aspirin plus clopidogrel may be justified, but only as part of aggressive medical therapy:
statin, BP, diabetes, smoking, lifestyle.
DAPT alone is not a treatment plan.
Lacunar stroke?
Respect SPS3.
Long-term aspirin plus clopidogrel is not wisdom.
It is bleeding dressed as prevention.
ESUS?
Do not guess with anticoagulation.
Start antiplatelet, investigate properly, and reclassify the mechanism when evidence appears.
AF-related stroke?
Antiplatelet therapy is not enough.
The patient needs an anticoagulation strategy when safe.
Stroke on aspirin?
First ask:
Was it really aspirin failure?
Or was it:
missed AF,
intracranial stenosis,
carotid plaque,
non-adherence,
wrong dose,
cancer-associated stroke,
or uncontrolled risk factors?
Never escalate before you re-diagnose.
The clean bedside rule:
DAPT is a bridge.
SAPT is the destination.
Anticoagulation is a different road.
Mechanism decides the map.
In stroke prevention, the most dangerous antiplatelet error is not choosing the wrong tablet.
It is forgetting to write the stop date.
#Neurotwitter #MedX #Stroke #Aspirin
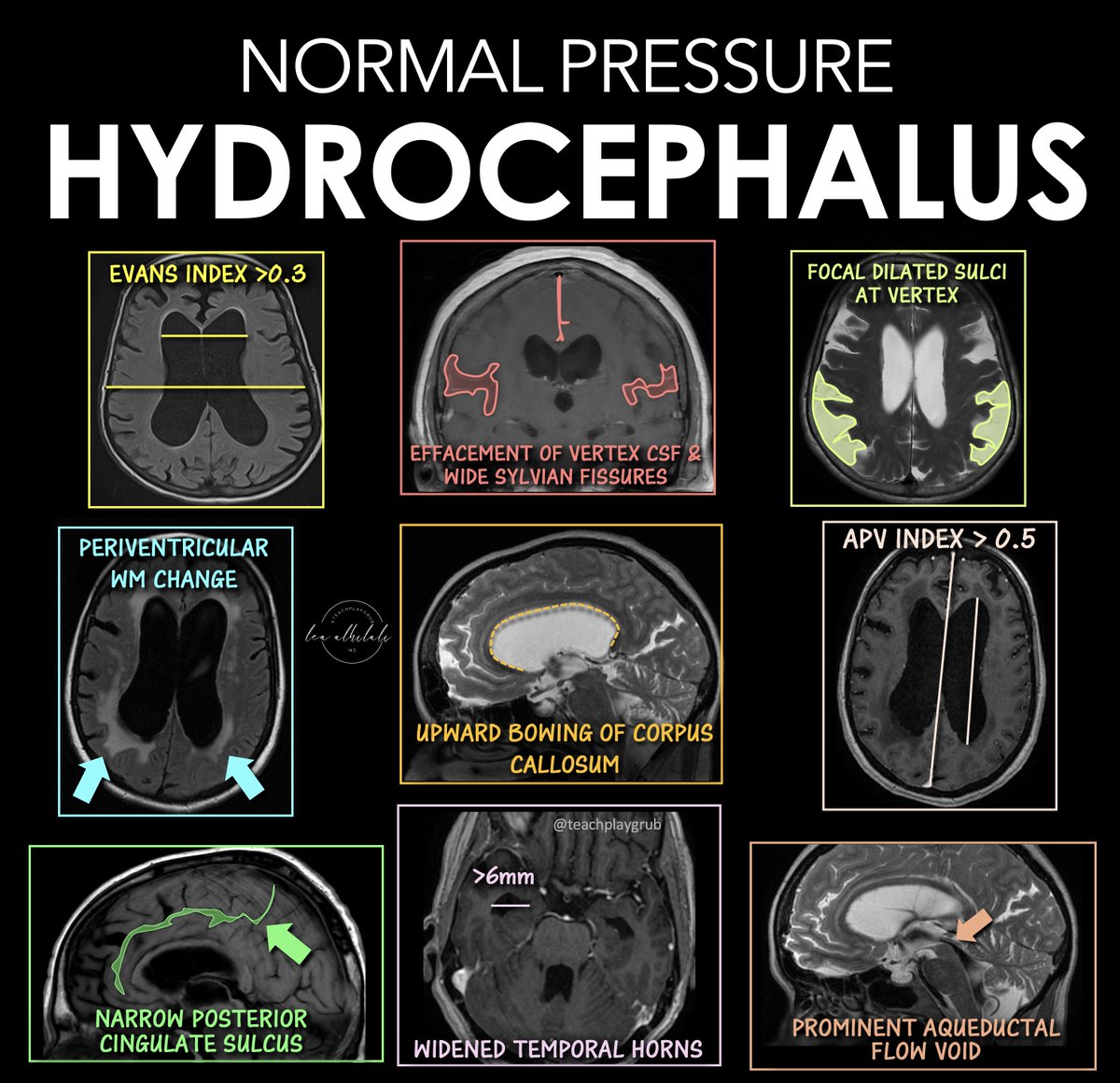
To call it or not to call it? That is the question!
Do you feel a bit wacky & wobbly when it comes to calling normal pressure hydrocephalus on imaging?
You don’t want to overcall it, but you don’t want to miss it either!
Here are the signs of NPH
🔹 Evans Index > 0.3
--Enlarged frontal horns relative to skull width → ventriculomegaly.
Remember it: “One out of three is too big for me!”
🔹 Periventricular White Matter Change
--T2/FLAIR hyperintensity from transependymal CSF flow.
Remember it: “Leaking pressure leaves a glow.”
🔹 Narrowing of the Posterior Cingulate Sulcus
--Tight high-convexity sulci from crowding at the vertex.
Remember it: “The top gets squeezed shut.”
🔹 Effaced Vertex CSF + Wide Sylvian Fissures
--Tight sulci up top but enlarged fissures laterally (DESH pattern).
Remember it: “Dry on top, wet on the sides.”
🔹 Upward Bowing of the Corpus Callosum
--Ventricular expansion pushes the corpus callosum upward.
Remember it: “If the corpus callosum is arched, the patient can’t march (wobbly)”
🔹 Temporal Horns > 6 mm
--Early temporal horn dilation from hydrocephalus.
Remember it: “Big horns before big vents.”
🔹 Focally Dilated Sulci at the Vertex
--Patchy enlarged sulci despite surrounding crowding.
Remember it: “Holes in a leaky roof = too much water on the brain!”
🔹 APV Index > 0.5
--Increased ventricular-to-parenchymal proportion suggesting hydrocephalus.
Remember it: “Glass half full is too much!”
🔹 Prominent Aqueductal Flow Void
--Increased CSF flow through the aqueduct on MRI.
Remember it: “If the aqueductal flow is super black, the ventricles are out of whack.”
Classic NPH imaging theme: enlarged ventricles + tight high convexities + disproportionate CSF redistribution.
Hopefully now you won't wobble on the diagnosis of NPH!!
Mononeuritis multiplex is not just neuropathy.
It is a red flag.
⚠️ Painful
⚠️ Asymmetric
⚠️ Stepwise nerve involvement
Think vasculitis until proven otherwise.
This is a neurological emergency—delay can mean irreversible nerve damage.
Common culprits:
• ANCA-associated vasculitis
• Polyarteritis nodosa
• SLE
• Cryoglobulinemia
• Rheumatoid vasculitis
Key clinical clue:
➡️ Sudden wrist drop / foot drop in different limbs, at different times
What to do:
✔️ Act early
✔️ Confirm with NCS + biopsy (when needed)
✔️ Start immunosuppression promptly
Miss it → disability
Catch it → salvageable
#Rheumatology #Neurology #Vasculitis #MononeuritisMultiplex @docakx@IhabFathiSulima #MedicalEducation #ClinicalPearls #AutoimmuneDisease #EarlyDiagnosis
Leptin is often reduced to a satiety hormone.
But that misses the bigger picture.
Leptin is trying to defend fat balance
And in doing so, it can drive hypertension
What is leptin?
Leptin is an adipokine released by fat cells
More fat → more leptin
Less fat → less leptin
Its job:
• tell the brain you’ve had enough
• tell the body to burn stored fat
How does it burn fat?
Leptin activates the sympathetic nervous system
→ norepinephrine release
→ β-adrenergic stimulation on fat cells
→ activation of hormone-sensitive lipase
→ breakdown of triglycerides into free fatty acids
Leptin is not just saying “stop eating”
It’s saying:
→ “use what you’ve stored”
But biology doesn’t work in isolation
There is signal crosstalk
Think about insulin.
Its goal is to lower glucose
But when chronically elevated, it spills over:
• fat storage
• sodium retention
• increased uric acid
• growth signaling → acanthosis nigricans, skin tags
All in an attempt to control glucose
Leptin behaves the same way
Its goal is to reduce fat mass
But in metabolic disease:
• leptin levels are high
• the hypothalamus becomes resistant to satiety signaling
Yet—
The pathways driving the sympathetic nervous system remain active
So now you have:
Leptin trying harder to:
• suppress appetite
• burn fat
But instead creating:
• chronic sympathetic activation
• increased heart rate
• vasoconstriction
• renal sodium retention
→ elevated blood pressure
This is centrally driven hypertension
The leptin-resistant hypothalamus ignores satiety
but keeps the sympathetic nervous system turned on
Bottom line
Leptin is not malfunctioning
It is overcompensating
Trying to fix fat balance in a resistant system
But that signal spills over
→ into sympathetic overdrive
→ into hypertension
Control leptin
Control insulin
Restore signaling
And you don’t just affect weight
You affect blood pressure
Drop your thoughts below 👇👇
See my previous blood pressure post below 👇👇
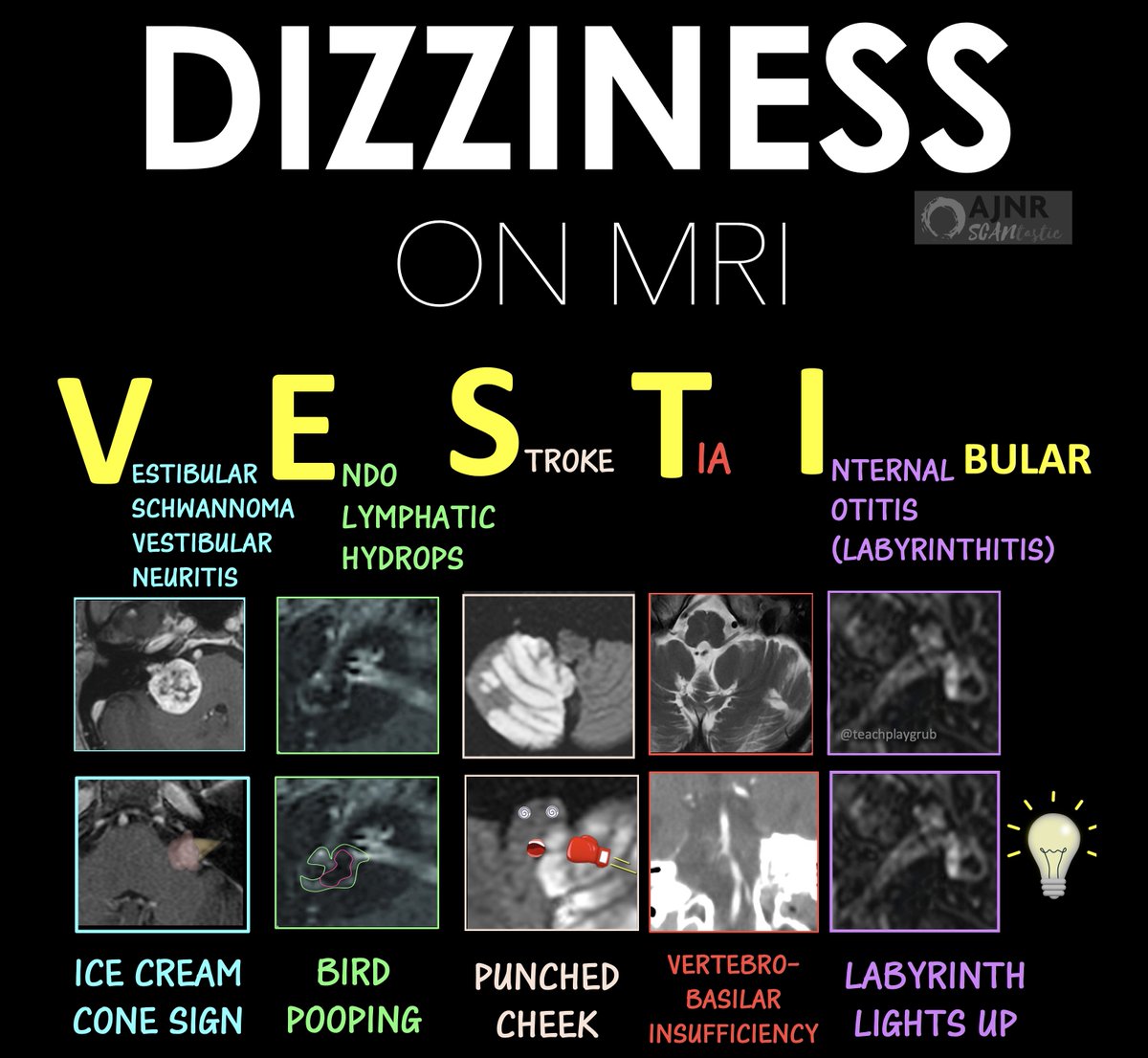
1/Do scans for dizziness make your head spin?
Need to know what to look for?
Just hear me out!
This month’s @theAJNR SCANtastic will show what to look for:
https://t.co/oLdQvuIDR6
Does the work up for dizziness make your head spin?
Wondering what you should look when a patient presents w/dizziness?
This month’s @theAJNR SCANtastic has what you need to hear!
https://t.co/glUq8OwQdB
For every patient w/dizziness, remember the mnemonic VESTIBULAR to remind you what to look for:
V is for vestibular schwannoma, vestibular neuritis
E for endolymphatic hydrops (Meniere’s)
S for stroke
T for TIA
I for internal otitis (labyrinthitis)
B for BBPV
U for under hydration
L for loops of vessels (vascular loops)
A for arrhythmia
R for recurrent migraine (vestibular migraine)
In this month’s @the AJNR, de Pont et al. looked at delayed post contrast imaging for Meniere’s. They found that when the filling defect for the endolymph herniates into the semicircular canal, Meniere’s disease is usually more severe & chronic
I think it looks like a bird pooping!
So now you know this finding for Meniere’s disease on delayed post contrast MRI! Hopefully now an MRI for dizziness won’t put you off balance!
Follow @theAJNR & check it out for yourself!
https://t.co/glUq8OwQdB
🤵♀️A 41-year-old woman develops progressive dysphagia, diplopia, and limb weakness. Days later she deteriorates with seizures and decreased consciousness. Brain MRI is performed during ICU admission.
🥼What is the most likely diagnosis?
🙆♀️A 42-year-old woman with septic shock and coma undergoes brain MRI after status epilepticus.
🧠Supratentorial cortical abnormalities are present, but the cerebellum shows contralateral involvement despite no primary lesion.
Which phenomenon explains this crossed pattern?
😓66-year-old man with sudden left arm weakness and dysarthria. MRI: acute infarct in the left capsule-thalamic region. CTA: left PCA (P2) occlusion.
🙀But the deficit is ipsilateral.
😎Left–right confusion? Exam error? A glitch in the Matrix… or is there another explanation?