SSRIs can cause lasting alterations in hormonal secretion by desensitising serotonin receptors in the brain.
Most people will think of serotonin acting locally within the brain, but this isn't the case. By acting on the hypothalamus, which is essentially the hormonal 'master switch' of the body - SSRIs can impact the regulation of key hormones throughout the body.
These hormones include cortisol, growth hormone - and particularly Oxytocin. The so-called 'love hormone', oxytocin, plays a central role in mediating love, bonding and sexual desire.
There's evidence to show that treatment with SSRIs like Fluoxetine can cause these hypothalamix receptors to desensitise, resulting a lasting suppression of Oxytocin release. This effect is so pronounced that it can persist long after Fluoxetine has fully metabolised from the body.
Given that Oxytocin is crucial for sexual desire, this impact of SSRIs on the Hypothalamus could be vital in understanding Post-SSRI Sexual Dysfunction (PSSD).
I've written extensively precisely on their distinct mechanism of actions.
Psychedelic compounds exert their rapid and sustained effects on cortical structure and function primarily by activating 5-HT2A receptors.
Furthermore, lipophilic psychedelics (such as 5-MeO-DMT) can diffuse into neurons, engage these intracellular 5-HT2ARs, and trigger downstream pathways that drive dendritic spine growth.
However, the primary target of SSRI treatment can instead be considered the 5-HT1A receptor - with the goal being to desensitise its autoreceptor through sustained activation by inhibiting SERT.
Can SSRIs Cause Certain Genes To Be "Switched Off" In The Brain?
Epigenetics is the field of genetics that explains how gene expression can be altered without changing the underlying genetic code directly.
One example of a particularly enduring form of epigenetic modification is DNA methylation - which can essentially 'deactivate' a particular gene.
Chromatin Immunoprecipitation sequencing has found that Fluoxetine treatment can result in some puzzling epigenetic modifications.
Chronic exposure to Fluoxetine reduced the expression of an enzyme called CaMKII (calmodulin-dependent protein kinase II) in the Nucleus Accumbens.
The Nucleus Accumbens is a small structure in the centre of the brain that key for mediating feelings of reward and motivation.
CaMKII is an enzyme that regulates the level of Calcium in a cell and is conducive to glutamate and dopamine signalling as well as memory formation.
These are neurotransmitters that are involved in feelings of excitement and reward.
SSRIs in fact have their own set of effects on the endocrine system, by altering the behaviour of the hypothalamus. The hypothalamus is central to regulating hormone responses to hunger, sleep, arousal etc.
In one animal study, rats were treated with the SSRI fluoxetine for 14 days. Just 2 days after the end of treatment, the SSRI group showed 74% lower levels of Oxytocin and 68% lower levels of ACTH compared to control.
Can SSRIs Cause Certain Genes To Be "Switched Off" In The Brain?
Epigenetics is the field of genetics that explains how gene expression can be altered without changing the underlying genetic code directly.
One example of a particularly enduring form of epigenetic modification is DNA methylation - which can essentially 'deactivate' a particular gene.
Chromatin Immunoprecipitation sequencing has found that Fluoxetine treatment can result in some puzzling epigenetic modifications.
Chronic exposure to Fluoxetine reduced the expression of an enzyme called CaMKII (calmodulin-dependent protein kinase II) in the Nucleus Accumbens.
The Nucleus Accumbens is a small structure in the centre of the brain that key for mediating feelings of reward and motivation.
CaMKII is an enzyme that regulates the level of Calcium in a cell and is conducive to glutamate and dopamine signalling as well as memory formation.
These are neurotransmitters that are involved in feelings of excitement and reward.
One study of 55 Canadian women examined the impact of SSRI exposure in late gestation. The women were taking the SSRI Paroxetine at doses between 10-60mg during the third trimester, primarily to treat anxiety or depression.
Of the 55 infants exposed to Paroxetine, 12 (about 1 in 4) suffered severe complications necessitating prolonged hospitalisations.
9 of the babies suffered from respiratory distress, 2 experienced hypoglycemia and 1 from jaundice. Furthermore, 20% of the babies in the Paroxetine group were born prematurely versus only 3.7% in the control.
@cbaileyreno No, simply that there appears to be a genetic risk factor in developing PFS. I present the evidence that PFS is driven by epigenetic changes, which are reversible, here: https://t.co/H30jrPfom7
The key to understanding your hormones isn't necessarily just their serum levels, but the genetics determining your hormone receptors...
For example the androgen receptor, which is bound by the typically male hormones such as testosterone and DHT can have dramatically different sensitivities based on your individual genetics.
A key feature is the number of CAG repeats on an area of the receptor called the "Ligand Binding Domain". The more CAG repeats, the less sensitive you are to these male hormones:
More CAG Repeats -> Reduced Sensitivity
Fewer CAG Repeats -> Higher Sensitivity
Patients suffering from side effects from medications that disrupt these male hormones (such as Finasteride) are often found to have an abnormal number of CAG repeats.
Cecchin et al. (2014) examined the genomes of 69 patients purporting to have "Post-Finasteride Syndrome", as well as 91 control patients.
They found PFS patients were 6 times more likely to have an extremely high number of CAG repeats. This is likely a contributing factor to their enduring side effects, even when Finasteride treatment had long since ended.
Given the strong Androgenicity of DHT, it’s hardly a surprise that its depletion is linked to a host of undesirable side effects in both the body and the brain.
One of the functions of DHT is maintain the delicate balance between estrogenic (typically female hormone) activity in the body and androgenic activity.
One of the consequences of disrupting this balance is the risk of developing female bodily characteristics, such as gynecomastia.
The science underlying the lasting adverse effects of Finasteride is better understood that you might think. A small pilot study of patients complaining of Post Finasteride Syndrome found increased DNA methylation of the 5-alpha-reductase Type II gene in sample of cerebrospinal fluid.
DNA methylation is a form of epigenetic modification by which the gene becomes less accessible to transcriptional machinery, which in essence means the gene is ‘switched off’.
Intriguingly there’s evidence that DHT can stimulate its own synthesising enzyme in a positive feedback loop. It’s therefore possible that the supposedly temporary inhibition of 5-alpha-reductase by Finasteride can have a more lasting impact on gene expression.
You can read more here: https://t.co/119yCoF0ep
Did you know your individual genetics can dramatically alter your risk of side effects from medications?
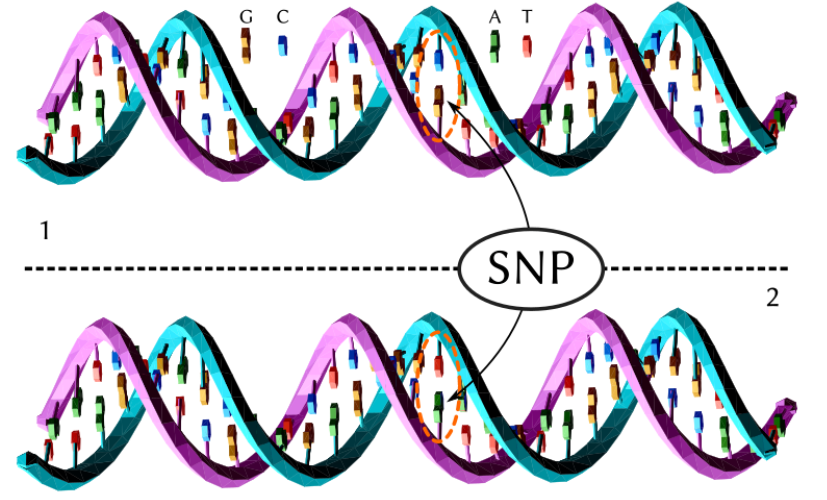
Single-nucleotide polymorphisms (SNPs) are simple ‘letter’ swaps in the DNA code that can result in dramatically different health outcomes.
In one study of 200 men treated with SSRIs, simply one of these single ‘letter swaps’ was found to be responsible in a 3-fold increase in the risk of developing sexual side effects.
The science around vitamin A and synthetic retinoids is complex and often appears contradictory. The key to understanding these disparities is the enormous difference between synthetic retinoic acid precursors, and the dietary retinols.
For example, studies on the hormonal effects of Isotretinoin treatment have consistently identified dramatic reductions in testosterone.
A 2019 study by Nasrallah et al measured an average 40% reduction in total testosterone across 113 male patients following six months of 0.5 mg/kg per day.
https://t.co/zVxBvraVP8
The study involved 201 Japanese patients - 36 of whom developed clinically significant sexual dysfunction from paroxetine, fluvoxamine, or milnacipran.
A genome wide association screening of 186,320 SNPs was performed to pinpoint genetic hotspots linked to SSRI/SNRI‐induced sexual side effects.
Eleven SNPs identified a strong association with the MDGA2 (a gene implicated in neural development and synaptic adhesion).
The strongest signal came from rs1160351, where each risk allele nearly tripled the odds of SSRI/SNRI‐induced sexual dysfunction (risk ratio 2.92).