Don’t Miss It! ASPC’s Imaging MasterClass is almost here, and the agenda is 🔥 Sat, April 5 | 10 AM EDT, FREE Half-Day Virtual Event, Focus: Multimodality Cardiovascular Imaging for Prevention – Must-know insights for clinicians! @a_l_bailey@CardioMDPhD
https://t.co/cfUPIQrDVC
Becoming a leader in cardiovascular medicine
Empower others, mentor, and foster a clear vision putting the team first. Connect with people and communicate wisely with careful choice of words and actions. Prioritize things that give you joy, respond gracefully to challenges, and always stay true to yourself.
#Leadership #ACC25 @ACCinTouch@JACCJournals
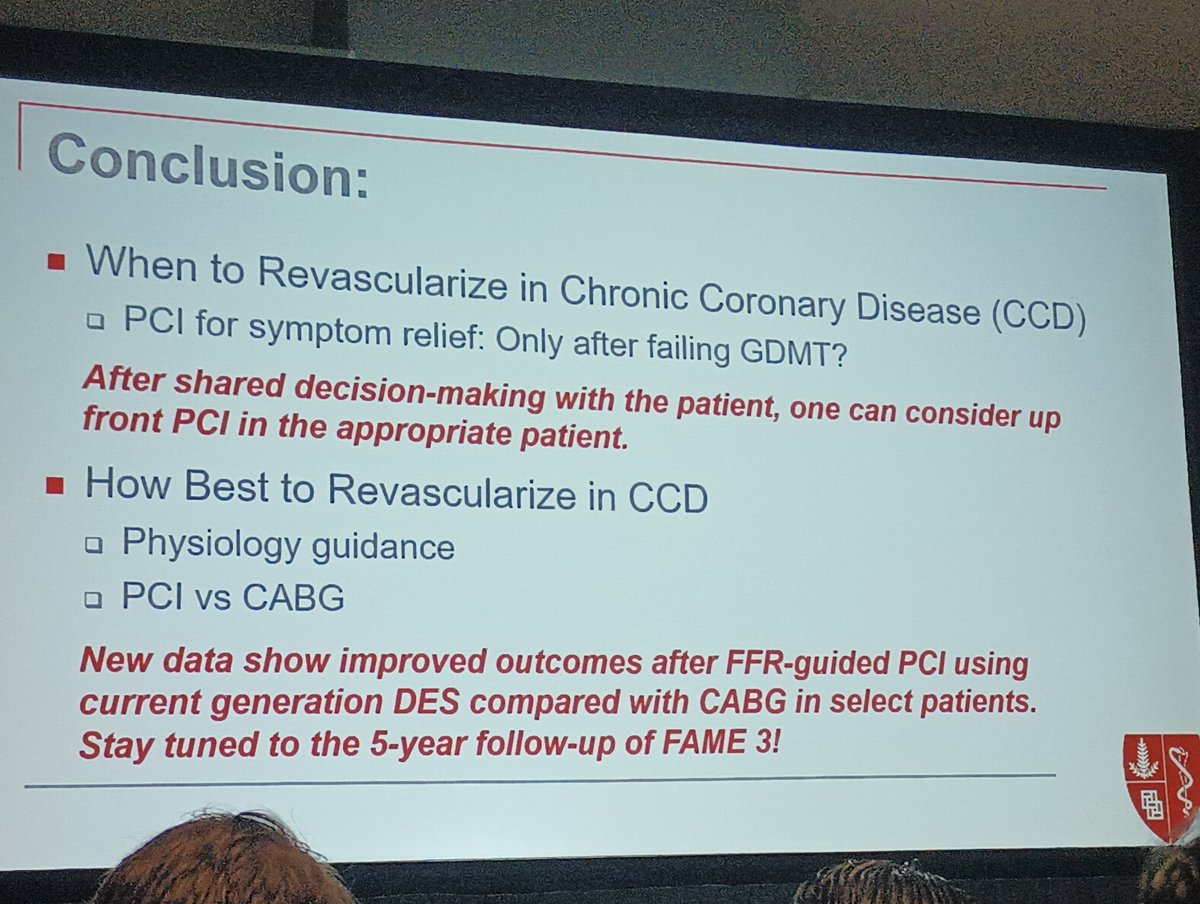
What's new in the chronic CAD guidelines?
Come learn more in room S404!
Discussion on pharmacological and non-pharmacological management, indications for revascularization, and investigating chronic CAD
#ACC25@JACCJournals@ACCinTouch#accfit
#CardioNugget 53/365
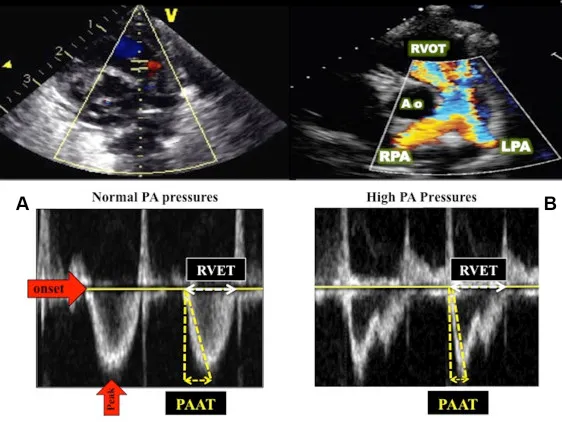
Echo Pearl: Acceleration Time (AT) in TTE!
AT = Time from onset of flow to peak velocity on Doppler.
1️⃣ Pulmonary Valve & Pulmonary HTN (PH) 🫁
👉 RVOT AT (PW Doppler @ RVOT)
📏 AT < 100 ms → ⬆️ Pulmonary Vascular Resistance (PVR), suggests PH
📏 AT < 60 ms → Highly suggestive of severe PH
✅ Normal AT >120 ms
2️⃣ Aortic Valve & Aortic Stenosis (AS) 💔
👉 Aortic Valve AT (CW Doppler @ AV)
📏 AT > 100 ms → Severe AS
📏 AT > 120 ms + AT/ET > 0.35 → 🚨 Highly suggestive of severe AS
🧐 Useful in low-flow, low-gradient AS!
3️⃣ Mitral Valve & Mitral Stenosis (MS) 🫀
👉 Mitral Inflow AT (CW Doppler @ MV)
📏 Prolonged AT → Think Mitral Stenosis!
4️⃣ Prosthetic Valves 🏗️
AT helps differentiate normal function vs prosthetic stenosis or patient-prosthesis mismatch in bioprosthetic & mechanical valves.
📝 Take-Home Points:
✅ Short RVOT AT = PH
✅ Prolonged Aortic AT = AS
✅ Prolonged Mitral AT = MS
✅ AT is valuable in prosthetic valve assessment!
#CardioNuggets #echofirst #MedEd
Insightful sessions at the BCM Hospital Medicine Conference today—huge thanks to @sargsyanz & @StephVSherman for organizing!
Here are my top 5 takeaways (more in the image below):
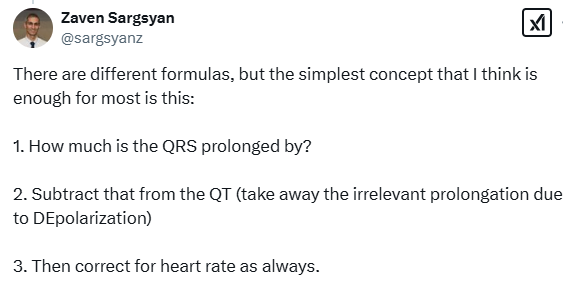
1️⃣QTc-↑ meds may be safe if prolonged due to ↑ QRS: Calculate the modified QT (QTm) to account for this—details in the image!
2️⃣ Hypokalemia ↑ risk of hepatic encephalopathy in cirrhosis. When repleting K: PO > IV—it's safer, cost-effective & patient-friendly. To promote safe diuresis, use a 5:2 spironolactone: furosemide ratio, titrating up to 400mg :160mg with close monitoring!
3️⃣ Naltrexone is safe for alcohol dependence in most liver disease patients, including cirrhosis, except in advanced cirrhosis (Child-Pugh C).
4️⃣ Sarcopenia worsens cirrhosis outcomes. Mitigate it with a bedtime snack & avoid long fasting periods!
5️⃣ Serum bicarb ↑ during diuresis? Don’t panic! It’s not always contraction alkalosis—other causes include ↑ bicarbonate reabsorption & ↓ chloride from diuretics.
@BCM_InternalMed@BCMDeptMedicine
#MedTwitter #MedEd
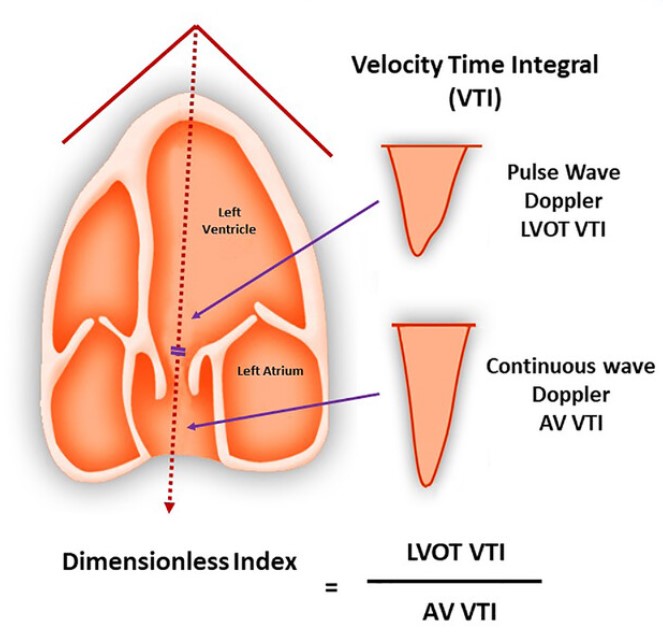
Cardiology Pearls - Aortic stenosis
What is the dimensionless index (DI)?
DI is used to assess severity of aortic stenosis. This metric doesn't require calculation of the LVOT cross-sectional area involved in obtaining the aortic valve area (a measurement which can be prone to error).
Calculated by dividing LVOT-VTI by AV-VTI:
>0.50: mild AS
0.25-0.50: moderate AS
<0.25: severe AS
Other parameters for defining severe AS
Vmax ≥ 4m/s, MG ≥ 40 mmHg, AVA ≤ 1cm²
@CardioNerds
#CardioEd #cardiotwitter
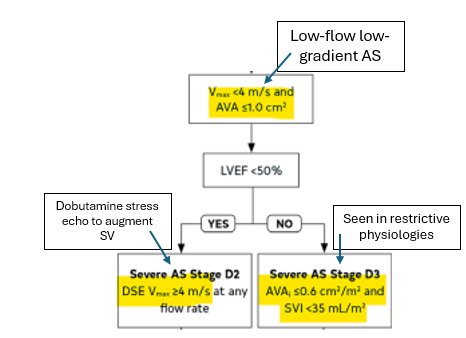
Cardiology Pearls - Aortic Stenosis
What is Low-flow Low-gradient severe Aortic stenosis?
When AVA ≤ 1cm² but Vmax < 4m/s and MG < 40 mmHg
There are 2 variants:
1. Low EF (<50%): augmentation of stroke volume with Dobutamine stress echo results in Vmax ≥ 4m/s = true severe AS
2. Preserved EF (>50%): seen in restrictive physiologies, calculation of AVAi ≤ 0.6cm²/m² and SVI <35ml/m² = true severe AS
What is pseudo-AS?
Low EF (<50%): augmentation of stroke volume with Dobutamine stress echo results in AVA > 1cm²
@CardioNerds
#CardioEd #cardiotwitter
🌟 Don’t miss this 🅓🅔🅔🅟 🅓🅘🅥🅔 led by the brightest minds in the field!
🗓️ February 4, 6, and 11 | 6:30–8:00 PM ET
🔗 Register now: [https://t.co/QsHQy3OY8I](https://t.co/4RTrT1fN5f) 👍
5.What are some risks with SGLTi?
- ⬆️ risk of fungal or yeast infections - ⬇️ by good perineal hygiene and ✅ glycemic control
- DKA (<0.5% of patients) - ⬆️ risk during prolonged fasting e.g. peri-surgery or GI illness when patients should be counselled to stop their SGLTi