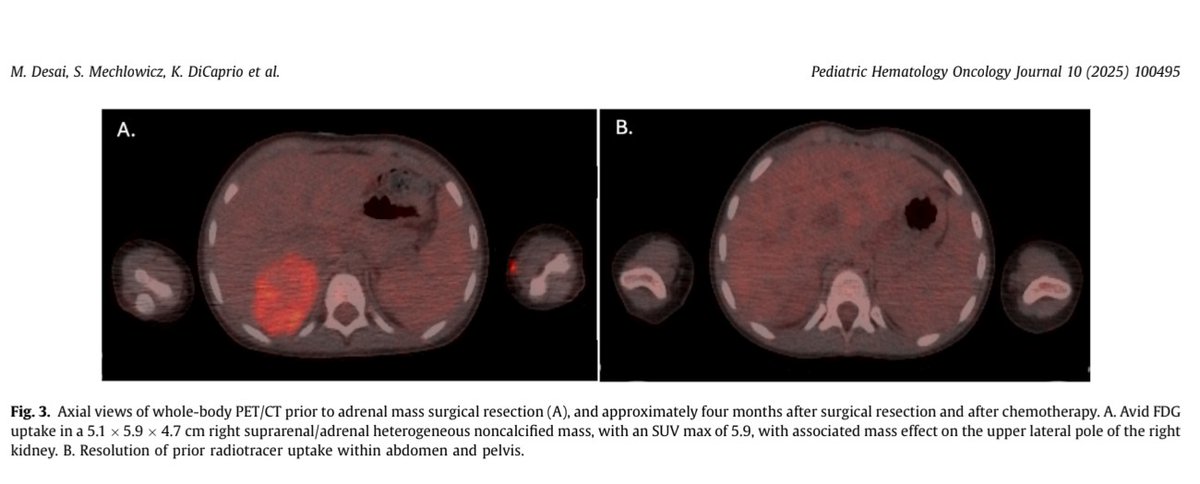
When one rare tumor wasn’t rare enough, this toddler said 'Let’s make it a case report'
Synchronous ERMS + ACC + germline CBL mutation = genetics keeping pediatric oncology on its toes.
Moral: If a kid brings two tumors to clinic, always invite genetics to the party #GeneticsWins
BRAF V600E mutations. Nanoparticle-based delivery of targeted
agents, like anti-BCL2 or cytokine inhibitors, represents an emerging therapeutic strategy. Have you noticed this phenomenon in your practice? Give your inputs in comments #pediatriclch#langerhanscellhistiocytosis
This systematic review by Dana Ashkenazi Lustig and colleagues from Israel speaks about the spontaneous resolution of LCH lesions. Proposed mechanisms include biopsy-induced inflammatory
system modulation, apoptosis via the Fas/Fas-L pathway, & disruption of the MAPK signalling
These findings highlight the importance of
regular monitoring of height & weight during & after therapy.
Future prospective studies incorporating body composition assessments may provide further insight into sarcopenic obesity & long-term metabolic risks in this population
Krisha Savla and colleagues from Tata Memorial Hospital, Mumbai have described their findings about the nutritional status of children with acute leukemias receiving chemotherapy at their centre. Details of the findings in comments.
In this cohort, 37.5 % of children classified as malnourished.
At end of Rx, 5.3 % were severely & 22.6 %
were moderately malnourished, 8.2 % were overweight & 6.7 %
were obese
Improvement in the status could be attributed to effective nutritional interventions, supportive care
https://t.co/8gLHkpFr8G
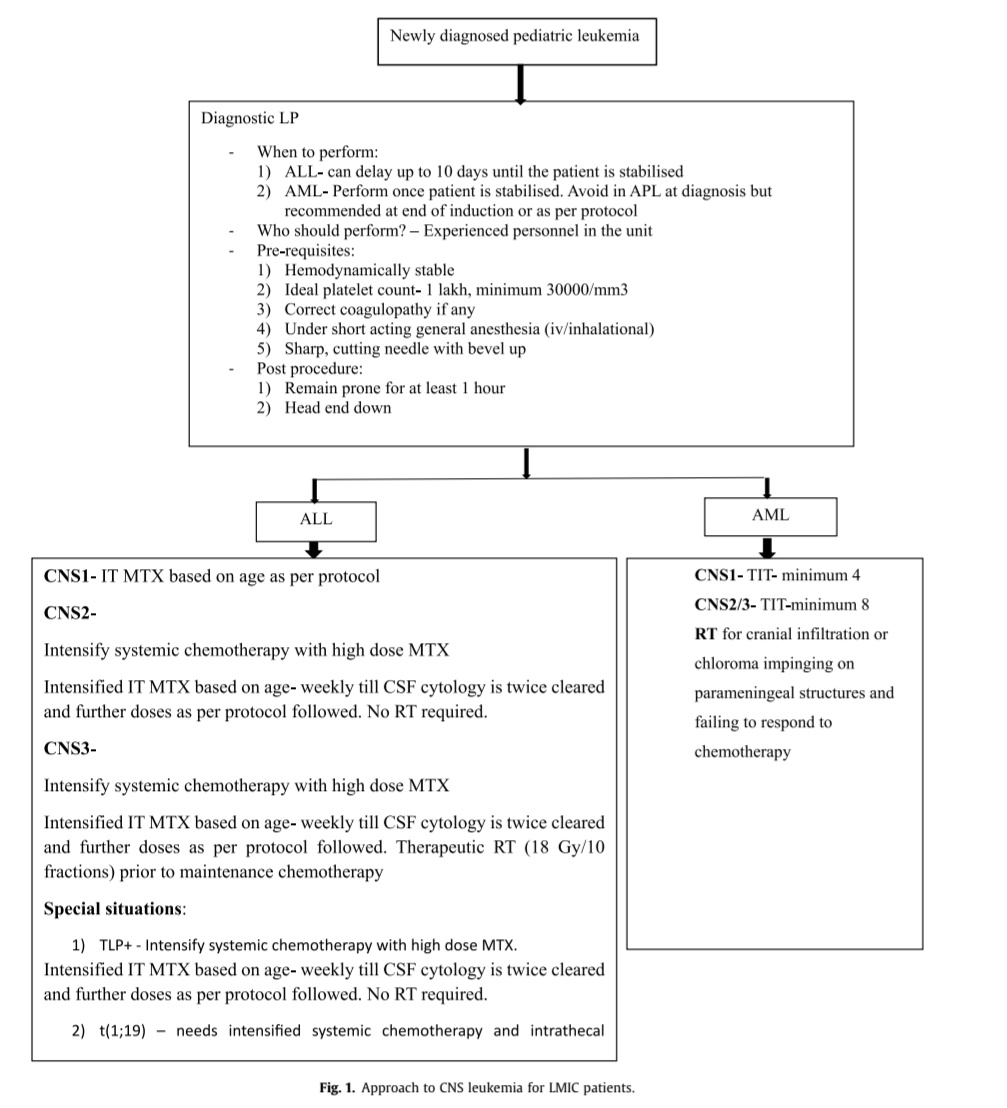
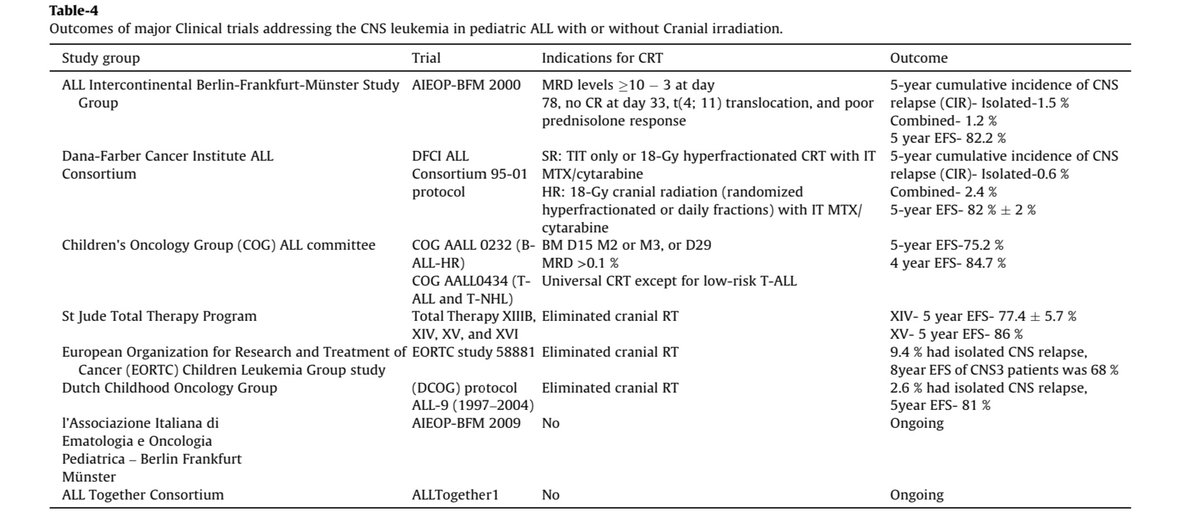
This interesting article written by Maya Et al describes the diagnostic algorithm in CNS leukemias, CNS directed therapy in ALL, management of CNS disease at relapse, role of newer agents and immunotherapies, CNS directed treatment in ALL and AML.
TNT (Triple-Negative Thrombocytosis) Treatment Algorithm —
Proposed by BJHaem, Godfrey et al. — shown at the 3rd Kuwait Hematology Conference
🧬 First question: Clonal or non-clonal?
🔍 Second question: Megakaryocyte atypia or not?
➡️ These 2 answers place every patient into 1 of 4 treatment pathways.
⸻
🟥 1) Clonal marker + Megakaryocyte atypia
Triple-Negative ET with clonal marker (cTNT-ET / ITAM-C)
• Age ≥60 or refractory symptoms or cardiovascular RFs → Aspirin if no bleeding risk
• Age ≥60, prior vascular event, persistent Plt ≥1500×10⁹/L, or refractory symptoms → Consider cytoreduction
• Monitor for evolution toward PMF/MDS/other MPN
⸻
🟧 2) Non-clonal + Megakaryocyte atypia
ITAM (Idiopathic thrombocytosis with atypical megakaryocytes / TN-ET without clonal markers)
• Age ≥60, symptoms, or CV risk → Consider aspirin
• Age ≥60, prior vascular event, Plt ≥1500×10⁹/L, or multiple CV RFs → Consider cytoreduction
• Monitor carefully for transformation; marrow should be repeated if phenotype changes
⸻
🟦 3) Clonal marker + No megakaryocyte atypia
CTUS (Clonal thrombocytosis of undetermined significance)
• Age ≥60 or symptoms or CV RFs → Could consider cytoreduction (case-by-case)
• Aspirin can be considered depending on risk profile and Plt count
• Monitor for evolution to ET/MPN
⸻
🟩 4) Non-clonal + No megakaryocyte atypia
ITUS (Idiopathic thrombocytosis of undetermined significance)
• Usually benign course
• Annual FBC monitoring
• Aspirin only if another indication (e.g., CV risk)
• Cytoreduction not recommended
⸻
Key Factors That Determine Treatment
1️⃣ Clonal or non-clonal?
2️⃣ Megakaryocyte atypia present or absent?
3️⃣ Age ≥60?
4️⃣ Symptoms?
5️⃣ Thrombosis history?
6️⃣ Cardiovascular risk factors?
7️⃣ Platelet count?
⸻
#MPN #TNT #TripleNegativeET #ET #CTUS #ITUS #Thrombocytosis #Hematology #NGS #KuwaitHematologyConference #SOHO25 #EmiratesHematologySociety
Bedside clinical skills have been diminished by an overreliance on technology. A new Review Article presents educational strategies for reinvigorating the bedside encounter and shows how much can be learned from it.
Read the review “Strategies to Reinvigorate the Bedside Clinical Encounter,” the latest in the Medical Education series, by Brian T. Garibaldi, MD, MEHP, and Stephen W. Russell, MD, from @NUFeinbergMed and the University of Alabama at Birmingham (@UABNews): https://t.co/7IF47hAwzR
#ScienceSaturday
❓ What controls whether T cells keep fighting or get tired?
➡️ A recent study in Nature Immunology reveals that a protein called SATB1 acts like a “brake” on CD8 T cells, the immune system’s cancer-fighting soldiers.
➡️ During chronic infections or #cancer, T cells can become exhausted over time. This research shows that SATB1 controls how fast T cells multiply and how strongly they attack tumors. When SATB1 levels are high, T cells stay balanced but may hold back their attack. When SATB1 is removed, T cells expand faster and fight harder, especially when combined with immunotherapy, though they may tire sooner.
➡️ Importantly, blocking #SATB1 improved tumor control and boosted the power of checkpoint inhibitors in preclinical models, suggesting a promising new strategy to enhance cancer immunotherapy.
🌟 Congratulations to the study authors at the University of Melbourne, Peter Doherty Institute, University Hospital Bonn, Peter MacCallum Cancer Center, and collaborators for deepening our understanding of T cell biology and uncovering a potential way to make immunotherapies even more effective. @UniMelb@TheDohertyInst@UniklinikBonn@PeterMacCC@NaturePortfolio
🔗 Read more: https://t.co/VIv9VjgAqg