Newly published: Low RV Ees/Ea predicts subsequent development of late right heart failure post LVAD better than basic RHC. Congrats to first author @OslerResidency SAR @lexiem515! And many thanks to our co-authors @Js08Paul & @RyanTedfordMD.
https://t.co/iE06HbLWYE
#PVLoops to dive deep into hemodynamic biventricular interactions in #LVAD patients
Thankful for opportunities to partake in this exciting work @MayoCVFellows
🫀Invasive monitoring is not dead. It was misunderstood
For years
Pulmonary artery catheters were abandoned
“Too invasive”
“No outcome benefit”
But maybe the problem was not the tool...It was how we used it 🧐
*Hemodynamics is not a number. It is a trajectory
This review reframes the concept
Not a snapshot
But a dynamic evolution
After initial therapy
The hemodynamic trajectory predicts outcomes
🫀 Clinical implication
If you are not reassessing You are treating blindly
*Phenotyping shock. The real power of invasive monitoring
Cardiogenic shock is not one entity
Cold and wet
Cold and dry
Warm and wet (SIRS-driven)
Mixed shock
🫀 Clinical implication
Same blood pressure
Different physiology
Different treatment
*Normotensive shock. The silent killer
One of the most important concepts
Patients can have:
Normal BP
Normal lactate
But low cardiac output
🫀 Clinical implication
SvO₂ ↓ is often more sensitive than lactate
Perfusion can be impaired before hypotension appears
*PAC is not for everyone. But essential for some
Routine use? No
Targeted use? Absolutely
Indications:
• Overt cardiogenic shock
• Unclear hemodynamics
• Failure of initial therapy
• Mechanical circulatory support
🫀 Clinical implication
Use PAC when decisions matter most
*Cardiac power output. The strongest prognostic marker
CPO = MAP × CO / 451
It integrates pressure + flow
🫀 Clinical implication
Low CPO = high mortality
Better than CO alone
*Right ventricle. The forgotten determinant
RV failure changes everything
Key markers:
• CVP/PAWP ratio
• PAPi
• Pulmonary compliance
🫀 Clinical implication
If you treat LV and ignore RV
You will fail
*Monitoring during mechanical support
tMCS is not “set and forget”
You need continuous adjustment
Flow
Preload
Afterload
RV-LV interaction
🫀 Clinical implication
PAC transforms tMCS from support
Into precision therapy
*AI is coming. But physiology remains the foundation
Hypotension prediction
Shock phenotyping
Outcome prediction
But Garbage data → garbage AI
🫀 Clinical implication
Good monitoring is the prerequisite for good AI
🤓Final reflection
We moved from:
Clinical exam → Non-invasive tools
Now we must integrate Invasive + non-invasive + physiology
Because monitoring does not save patients, Understanding does 🤓
📚 Baldetti L et al. Rev. Cardiovasc. Med. 2025; 26(6): 27034 https://t.co/tcTmhBNKC1
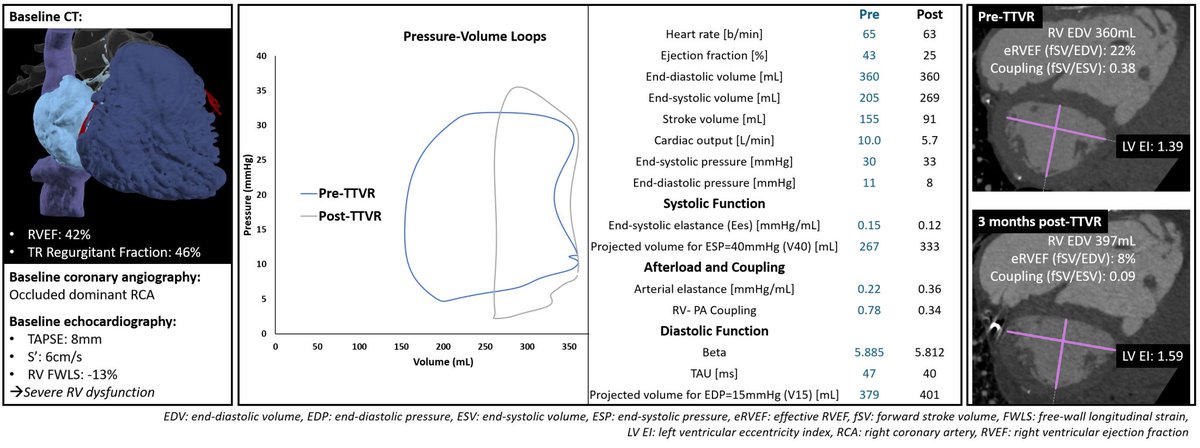
Post-#TTVR findings via #PVLoops:
📌 Worsening of RV/PA coupling
📌RV diastolic properties were preserved with unchanged capacitance
A multi-modality approach to better understanding RV function post-#TTVR!
🔗: https://t.co/BIdO72avny
#PVloop#hemodynamics#heartfailure
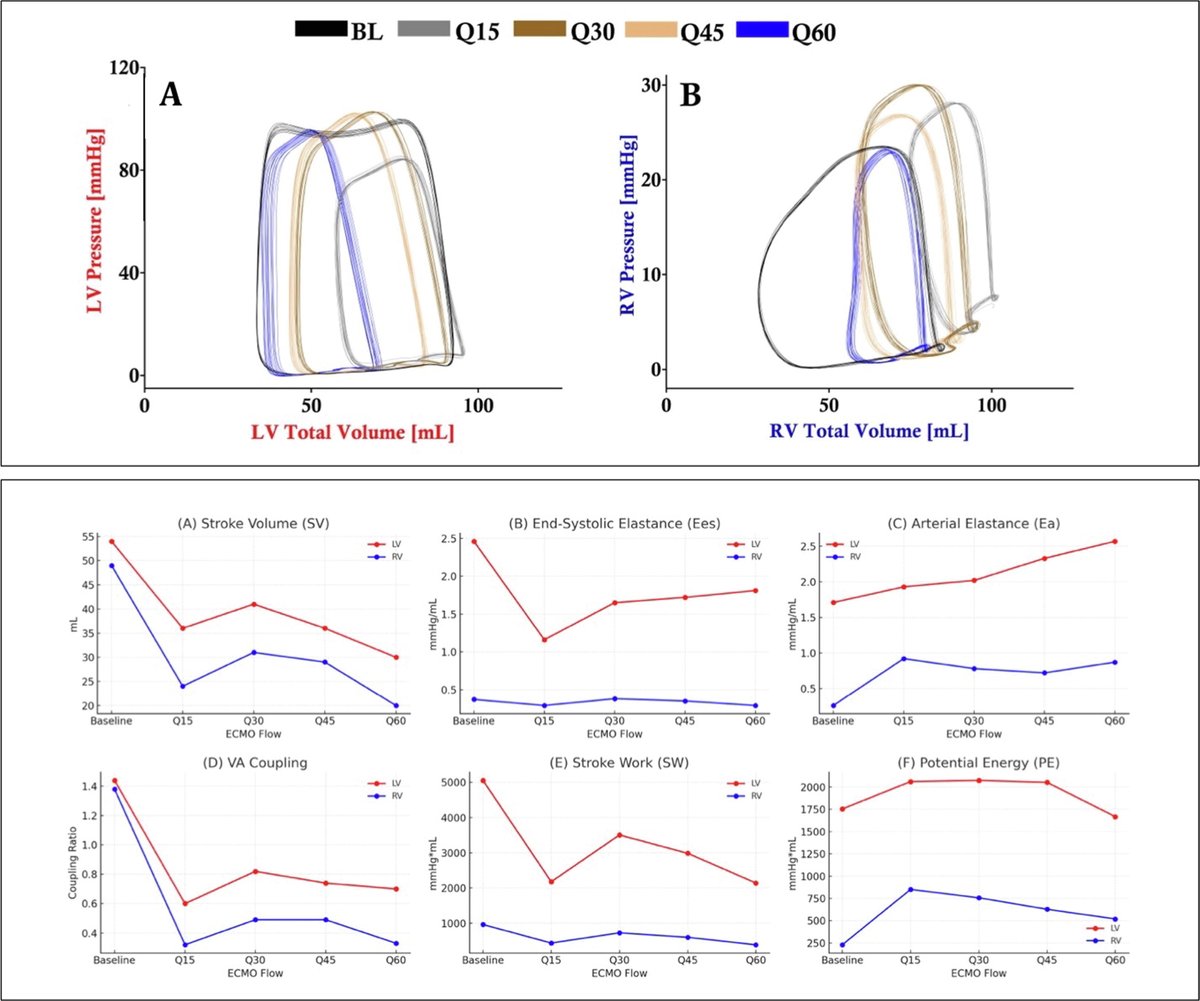
🚨"Bi-Ventricular #PVloop Response to VA-ECMO Flow Ramping"
🔗https://t.co/CPN2iGzbxF
Because the LV and RV respond differently to #ECMO changes, BiV #PVloop monitoring is essential to guide truly optimized, ventricle-specific ECMO management. 💡
#heartfailure#PVLoops#Cardio
🚀 Introducing CD Leycom's brand-new instructional #PVLoop#hemodynamics video series!
For both experienced #Cardiology researchers or those new to #PVloops, our latest series walks you through each step.
👉 Visit our Support page to watch: https://t.co/iSq36oeYXf
🔟 Take-home
Static diagrams make this look complex – two lines crossing, shifting, labelled with variables.
But the real system isn’t two lines at all – it’s one dynamic loop constantly finding balance.
Pms drives flow, Ivr resists it, and the heart only limits output when it can’t accept more return.
That’s the whole story.
The rest is just how the system re-equilibrates around that simple truth.
(Next time – more on why RAP doesn’t determine cardiac output.)
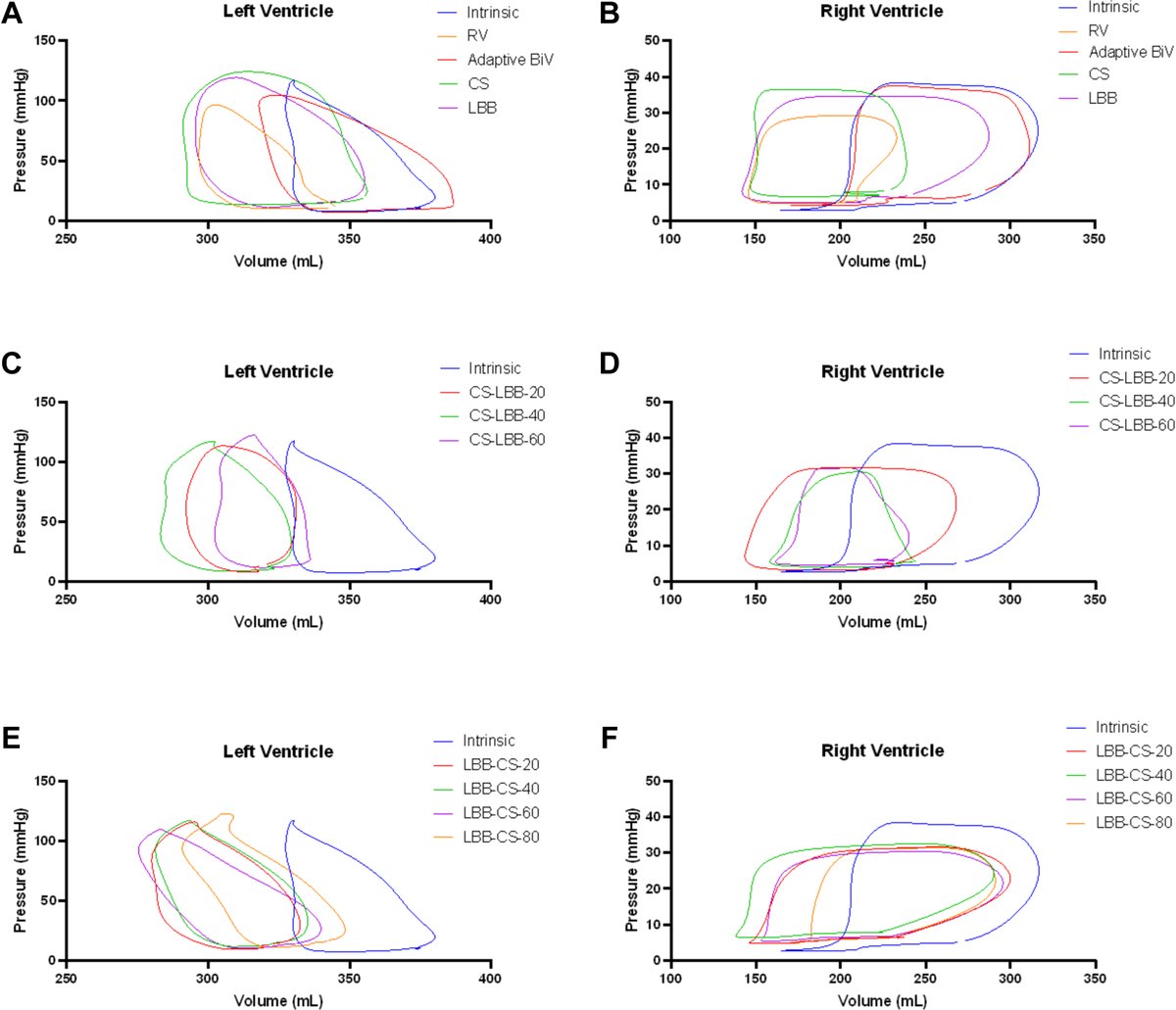
🚨 New Case Study: BiV #PVLoop Optimization of #CRT in an #LVAD Patient
Read here: https://t.co/1ucEVK5qF0
"Current guidelines...gap in consensus and the need for individualized management. #PVloops may serve as a powerful tool for guiding individualized device optimization."
Excited to participate at the #2025PICS Conference! 🎉
With the growing adoption of real-time, clinical #PVloops in congenital heart disease, we look forward to sharing the latest advancements in the field—along with our newly released #PVloop software.
#hemodynamics#cardiology
Always a pleasure catching up with Dr. @stevenhsu_md — a key contributor to advancing the use of RV #PVloops for better phenotyping in #PAH, optimizing #LVAD support, and other cutting-edge applications using real-time #PVloop#hemodynamics!
Link: https://t.co/F4uhWTCFan