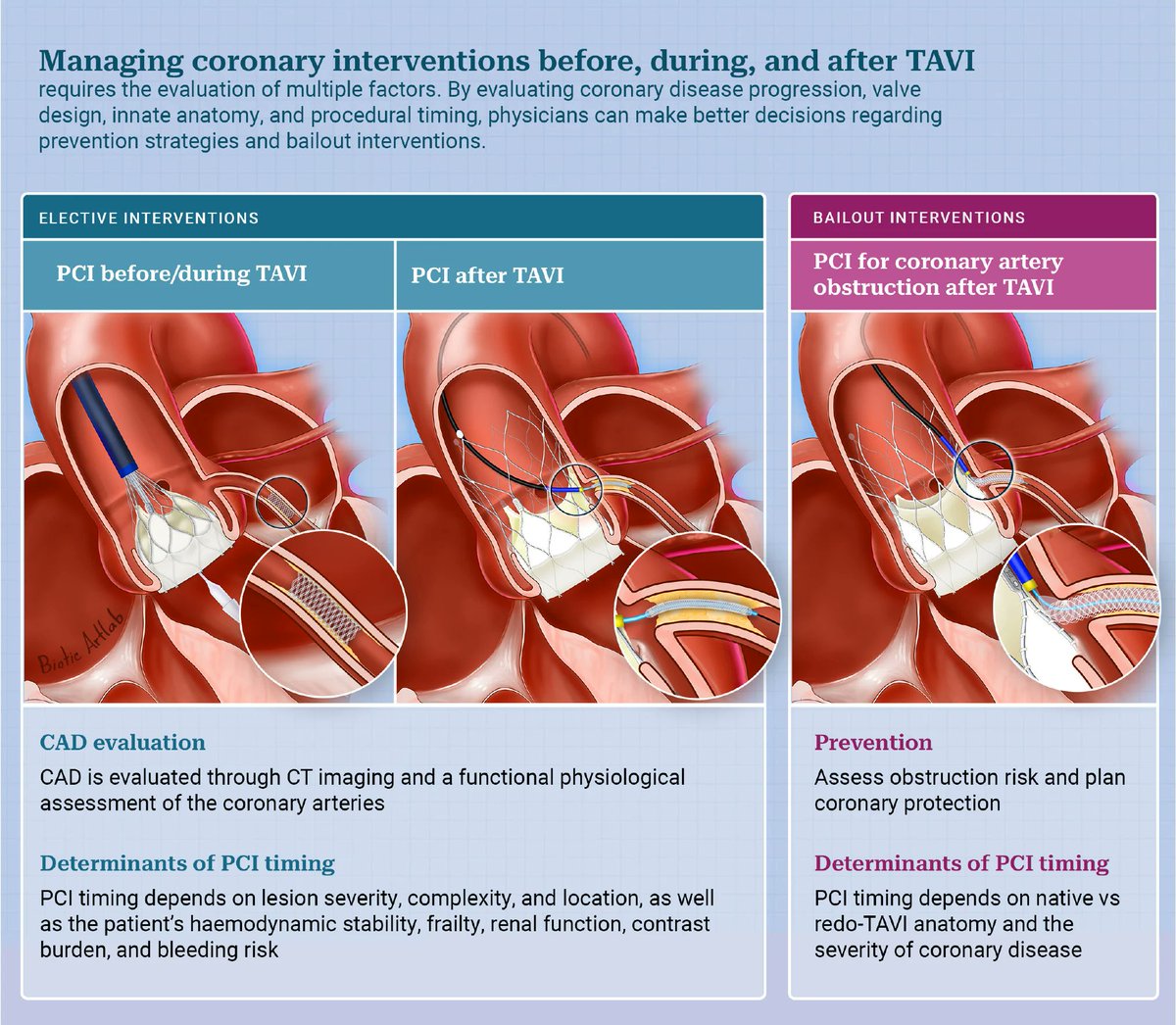
This State-of-the-Art review provides a comprehensive and practical overview of coronary interventions related to TAVI, encompassing coronary evaluation and physiological assessment, the indications and timing of percutaneous coronary intervention before and after valve implantation, and strategies for managing coronary obstruction. https://t.co/yojhLj5N5p
LV Torsion: A Powerful Marker of Systolic Function
Definition
Left ventricular (LV) torsion (or twist) is the heart’s wringing motion during systole: the apex rotates counterclockwise while the base rotates clockwise (viewed from the apex). This reflects the helical architecture of subendocardial and subepicardial myocardial fibers.
LV systolic mechanics occur in 3 planes:
- Radial (SAX) contraction: contributes to pressure generation
- Longitudinal (LAX) shortening: contributes to stroke volume
- Torsional deformation: enhances systolic efficiency and pressure development
How is torsion measured?
Using speckle-tracking echocardiography, torsion is calculated as the rotational difference between apex and base (degrees). Rotational velocity (deg/sec) can also be measured.
Why does it matter?
Torsion is a sensitive marker of myocardial performance and may detect dysfunction before EF falls.
Seen in:
🔵 Early ischemia
🔵 MI
🔵 HCM / DCM
🔵 HFpEF / HFrEF
https://t.co/itEeUHKifn
📉Understanding myocardial infarction (MI) localization.
This chart correlates specific EKG lead ST-elevations with their corresponding occluded coronary arteries- the LAD, LCx, or RCA and the affected myocardial territories.
#Cardiology#STEMI#EKG
🫀In cardiogenic shock, we still focus heavily on MACROcirculation:
📉 blood pressure
📉 cardiac output
📉 LVEF
📉 vasopressor dose
But what if the real battle is happening deeper?
🩸 At the microcirculatory level.
This excellent ATS viewpoint highlights one of the most important evolving concepts in shock physiology:
⚠️ normalization of macrocirculation does not necessarily mean restoration of tissue perfusion.
Despite advances in cardiogenic shock management, mortality remains >40%.
Even more striking, up to 45% of deaths occur in patients with normalized cardiac index.
That disconnect may be explained by persistent:
🩸 microvascular dysfunction
🩸 impaired capillary perfusion
🩸 endothelial dysfunction
🩸 tissue hypoxia despite “acceptable” hemodynamics
The review reinforces that: Microcirculation is not a passive bystander.
It may be a central driver of:
• organ dysfunction
• lactate persistence
• shock progression
• mortality
Particularly interesting is the emphasis on simple bedside tools.
We often think microcirculation requires advanced devices, yet:
📌 capillary refill time (CRT)
📌 mottling
📌 ΔPCO₂
📌 lactate trends
still carry strong prognostic value.
A CRT >3 seconds at ICU admission was associated with worse outcomes, and combining CRT with the CardShock score achieved an impressive AUC of 0.93 for outcome prediction.
The article also reviews modern technologies:
🔬 handheld vital microscopy
🔬 sublingual microcirculation imaging
🔬 NIRS
🔬 laser Doppler assessment
bringing “real time” bedside microcirculatory monitoring closer to clinical practice.
One of the strongest physiological messages:
⚠️ Shock is not only about flow. It is about effective tissue level oxygen delivery.
The review beautifully summarizes the four major mechanisms of microvascular dysfunction:
• heterogeneity
• hemodilution
• congestion
• edema
Particularly relevant for intensivists:
📌 venous congestion itself may worsen microvascular flow
📌 elevated filling pressures impair driving pressure
📌 edema increases oxygen diffusion distance
This is highly relevant in:
• advanced heart failure
• VA ECMO
• mixed shock states
• fluid overloaded patients
Another important takeaway: Persistent microcirculatory dysfunction after VA ECMO initiation was associated with increased mortality, even when macrocirculation improved.
Perhaps the key message of this paper is:
🩸 Microcirculation should no longer be considered a secondary endpoint in cardiogenic shock.
It may become one of the most important physiological targets of the next decade.
📖 Merdji H, American Journal of Respiratory and Critical Care Medicine. 2026, 212(3), 410–413 https://t.co/81Zp3aj274.
Recognizing lead-to-artery patterns can rapidly localize myocardial infarction and guide urgent intervention when every minute matters.
Bookmark this one.
@MattersoftheH14#MedTwitter#Cardiology#ECG#STEMI
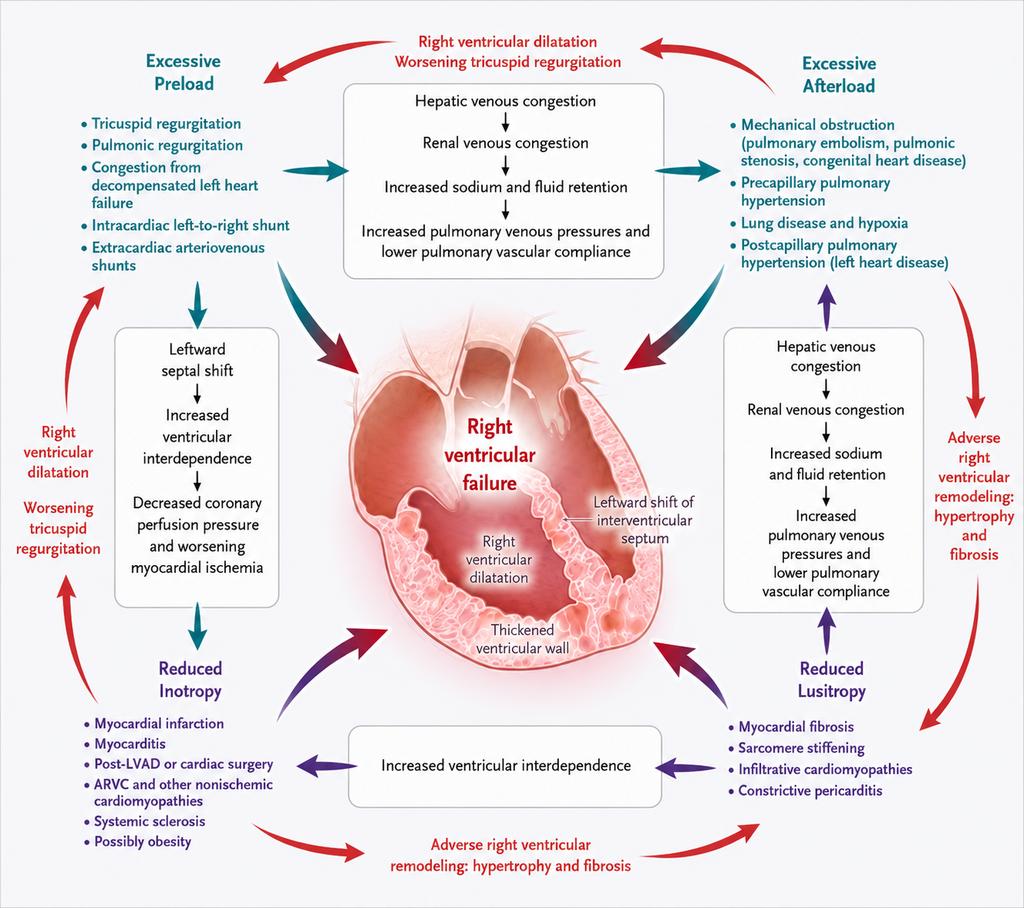
Right ventricular failure can rapidly progress from congestion to multisystem dysfunction.
Early recognition of RV strain, rising venous pressures, and worsening hemodynamics is critical in advanced cardiac care.
@MattersoftheH14#Cardiology#HeartFailure#MedTwitter #CriticalCare
🫀 CardioNugget
Disproportionate vs Proportionate Secondary MR
➡️ LVEDV (size) vs EROA (severity)
🔴 Disproportionate MR (COAPT)
Smaller LV, high EROA
MR out of proportion to LV dilation
👉 MR is a driver of HF
✅ TEER → benefit
⚪ Proportionate MR (MITRA-FR)
Larger LV, moderate EROA
MR matches LV dilation
👉 MR is a bystander
❌ TEER → limited benefit (focus GDMT)
🟢 Key Takeaway
👉 Same EROA ≠ same disease
👉 Always interpret MR relative to LV size
💡 Memory line:
“Out of proportion → fix the valve
In proportion → fix the ventricle”
#CardioNuggets #MedED #TEER #CardioMed
Efficacy of dual antiplatelet therapy for three months versus 12 months after coronary artery bypass grafting: multicentre, double blinded, randomised controlled trial: @bmj_latest
🥸 Top CABG-collaborative group.
👇👇👇👇
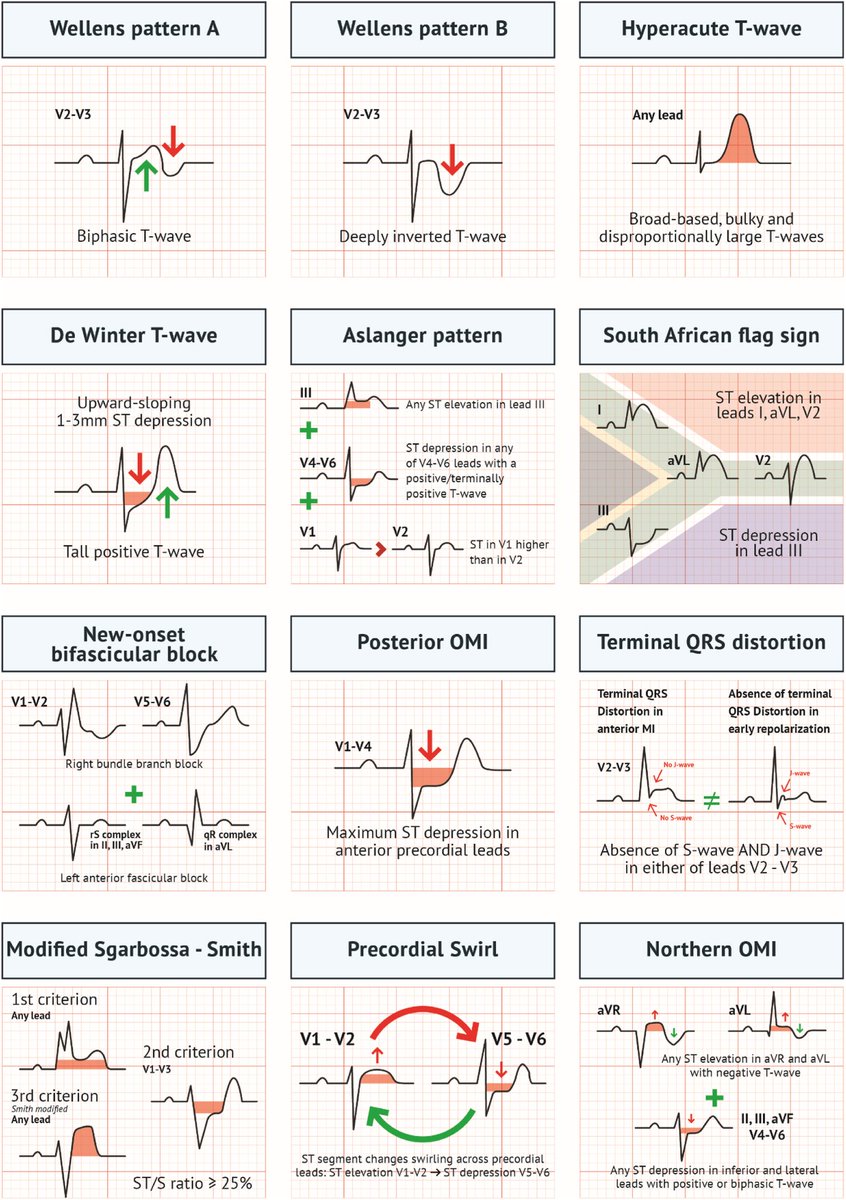
Acute MI is not always STEMI.
A major 2025 review highlights why relying only on classic STEMI criteria can miss dangerous coronary occlusions.
A thread on OMI (Occlusion Myocardial Infarction): 🧵
Recurrent TR after T-TEER can limit TTVR when central clips obstruct valve delivery. The ELASTA-T technique enables controlled leaflet detachment to facilitate TTVR. Read our step-by-step expert review on this novel strategy. #Cardiology#tricuspidvalve
🔗https://t.co/HwbLBYhn19
@fiorenzofio@TRheude@StarneckerF@XhepaErion@MichaelJoner3
1/14
Why can't you use direct oral anticoagulants (DOACs) in patients with mechanical valves (MVs)?
DOACs have been one of the most important advances in my career. And yet, the presence of a MV is one of the few contraindications.
The reason highlights the unique nature of thrombus formation in those with a MV and provides insights into the evolution of human hemostasis.