• Wakes up feeling perfectly fine
• Eyelids start to droop by the afternoon
• Double vision kicks in while reading
• Chewing dinner becomes completely exhausting
• Symptoms magically improve after resting
What is the diagnosis?
عقدتُ اجتماعاً مثمراً للغاية مع أخي صاحب السمو الشيخ محمد بن زايد آل نهيان، حيث ناقشنا العلاقات الهندية الإماراتية في مختلف القطاعات، وسبل تعزيز شراكتنا الاستراتيجية الشاملة. وقد جددتُ شكري وتقديري له ولحكومة دولة الإمارات العربية المتحدة على اهتمامهم ورعايتهم للجالية الهندية المقيمة في الدولة.
@MohamedBinZayed@G7
Consent from multiple parties ✅✅✅
‘Sandbag leads to tendon sag’
50s, female
Cross Fit
Longstanding bilateral anterior knee pain, but manageable
Doing hill work with sandbags – rapid deterioration of left sided infrapatellar pain on one descent over a few seconds & struggling to weight bear on way home and following few days
OE –
Tender through proximal patella tendon, but mostly focally over superficial aspect of distal patella
Unable to single leg squat, but double squat almost pain-free
Video reel -
Photo -
‘Sag’ of infra-patella soft tissues on left side (arrow) vs right (note - the PCL is radiologically & clinically intact, so not a confounding factor)
MRI (T2FS sagittals) –
Both knees show marked patellofemoral chondral changes and proximal patella tendinopathy
However, left side reported as showing separation of ‘patella sleeve’ – an unusual tendon tear configuration (arrow)
POCUS video with dynamic assessment (isometric resisted knee extension) highlights the defect further
After this, a different patient with a similar pathology, but in a different clinical context – chronic proximal patella tendinopathy, with no traumatic onset / acute injury history
Whilst undertaking a PRP injection targeting a deep surface tendon tear, we can see injectate flow proximally via the tendon defect into superficial patella aponeurotic ‘sleeve’ over distal pole (an unusual tear pattern – most ‘occult’ tears spread inferiorly into mid tendon body)
End of reel shows intra-operative arthroscopic debridement of a proximal tear and calcific tendinopathy (very cool 😎)
First, patella tendon arthroscopic debridement – we can see the surgeon cautiously debride the area of tendinopathy, tearing & fat pad back to healthy shiny tissue
Caution must be taken to not to take too much tissue bulk as this can ‘de-stabilise’ the tendon and lead to further tendinopathy or tearing
In the second half of the video, we see how POCUS (LS) in real-time readily identifies the calcific deposit in the tendon and helps the surgeon navigate the shaver safely to break it down
Finally, a mini-incision is made anteriorly to open the paratenon under direct vision and debride the neo-vessels
The patient can then load healthy remaining tendon rather than hammering away at damaged tissue that’s past the point of no return (‘deaf’ to tensile load)
In these presentations, Hoffa’s fat pad involvement is typical, often adhered to the area of deep surface tendinopathy with pathological neovascular in-growth (analogous to the Achilles and Kager’s fat pad pathophysiology)
‘Patella alta’ is a big risk factor for tendon pathology and is present almost universally in non-traumatic cases
Initial pre and post-surgical data with UTC scanning and patient score outcomes is promising
Musing –
How many recalcitrant patella tendinopathies – or tendinopathies 'full stop' - are due to these hidden defects?
Something to ponder…🧐
Consent ✅
‘Insane in the membrane’
Teenage professional dancer
Bilateral 'claudicant' crescendo / decrescendo crampy pain anterolateral shins (see patient map below)
Typically brought on by sustained effort - repetitive jumping based dance movements, but also fast walking and remaining ‘en point’
No latent symptoms at all
MRI lumbar spine, & pre and post exercise MRI of lower legs unremarkable
Nerve conduction and EMG studies normal
Dynamic CECS compartment pressure tests normal
US guided block of superficial peroneal nerve proximally had no effect
OE –
Normal except subjective reduction in ankle pulses with sustained ankle dorsiflexion and plantarflexion
POCUS video (doppler blood flow mode) –
Flow limitation in anterior tibial artery as it passes through the interossesous membrane with tibialis anterior contraction and passive ankle plantar flexion
Essentially a 'downstream variant' of PAES
Research link –
‘Anterior tibial artery entrapment syndrome: case report’
Miyamotto M et al. 'Anterior tibial artery entrapment syndrome'. J Vasc Bras. 2018
A quick post inspired by my favourite fellow Nervy Nerd, @simensletten on the Single Leg Heel Raise Test (SLHR) for the assessment of painful S1 radiculopathy.....
As you might expect, the plantarflexors are collectively mighty strong muscles, rendering manual muscle testing somewhat redundant in some situations and a quandary in others.
Manual testing may underestimate a meaningful deficit, categorising it as ≥4/5 MRC, and it does not examine fatigue, which is common in neuropathic presentations.
https://t.co/SuSd48e8W5
https://t.co/SPiC6z4kCm
To my knowledge, there is currently no validated schema for assessing plantarflexion strength in lumbar radiculopathy, but it is often recommended to approach it more functionally... enter the SLHR, or some kinda of tippy toe action.
I would usually screen initially with a simple one-rep side-to-side comparison and then selectively assess for “fatigue” when indicated.
In the paper by Hébert-Losier et al. (2017), normative SLHR values in healthy individuals ranged from roughly 20–35 repetitions, influenced by age, sex and activity levels. Similarly in recent cross sectional study cited later.
https://t.co/h4G16DjFJ8
This probably makes it more useful clinically as a “do as many as you can” test when comparing to the contralateral side, though small side-to-side differences (perhaps 2–3 reps) are likely normal.
Anecdotally, I’d probably regard a >30% side to side deficit in repetitions performed as something of an eyebrow raiser in the appropriate clinical context, though to my knowledge this is not based on any validated radiculopathy specific data.
As always, interpret alongside the wider clinical picture including diminished or absent achilles reflex, muscle atrophy and a qualitative account of how they perform it.
Importantly, performing a SLHR is probably not only about plantarflexion strength. Balance, intrinsic foot strength, coordination and confidence likely contribute too. I have had seemingly healthy people unable to get the heel off the ground on either side.
In terms of operationalising the test, there is also a more recent paper looking at SLHR performance in those with Achilles tendinopathy, including an accompanying app and demographic-adjusted website calculator. The term Heel Rise Endurance Test (HRET) is used here.
https://t.co/8iQACPEt8D
https://t.co/diGtI3DtSY
Perhaps something similar could be explored in painful S1 radiculopathy
as a future research project? How weak is weak enough?
@Seth0Neill
A major announcement from the UAE: @yasisland is set to become home to @SphereAbuDhabi — the first Sphere venue outside the US. Abu Dhabi is clearly betting big on tourism and entertainment, so I spoke with @dctabudhabi Chairman Mohamed Khalifa Al Mubarak about what this project says about the UAE’s ambitions.
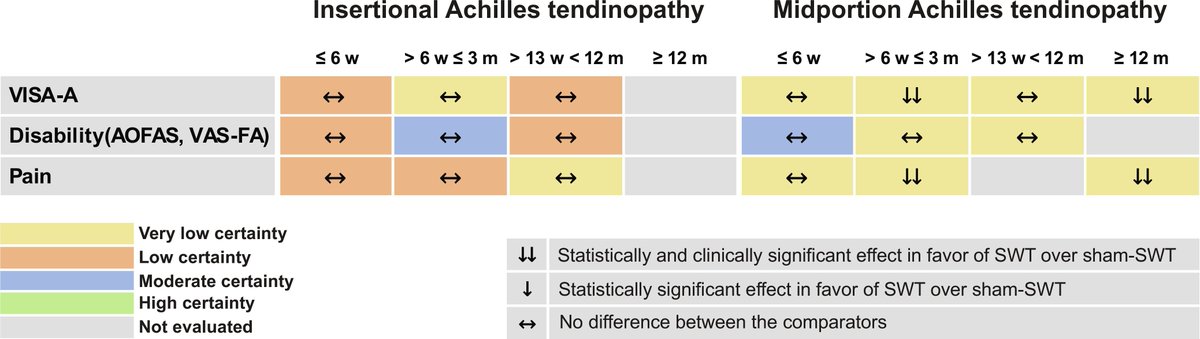
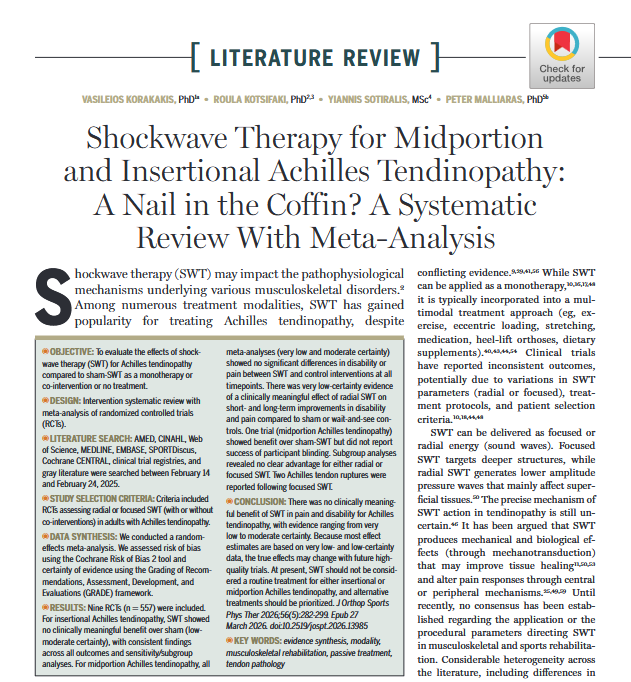
Are we putting a nail in the coffin for #Shockwave in #AchillesTendinopathy?
Our May #Review calls into question the benefits shockwave therapy & suggests sticking to treatments with robust evidence (i.e. exercise-based therapies)
Read it 👉 https://t.co/3mQLQjUm2W
#yourJOSPT
📣 NEW #Infographic ✅
📹 Video analysis of muscle strains in sport: qualitative and quantitative situational characteristics across muscle groups 💪
Full article ➡️ https://t.co/bDSkMucYxa
5 year prognosis for patellar tendinopathy
https://t.co/aStkKTAupF
71% returned to pre injury sport BUT only 68% of these (less than 50% of people overall) returned to pre-injury level of competition.
Not a good stat. We need to do better for patellar tendinopathy.
Posterior knee pain differential diagnosis.
I’ve focused on the more common injuries but it’s worth noting that bone stress injuries (such as tibial stress fractures) and bone tumours can also cause posterior knee pain, although they are more rare.
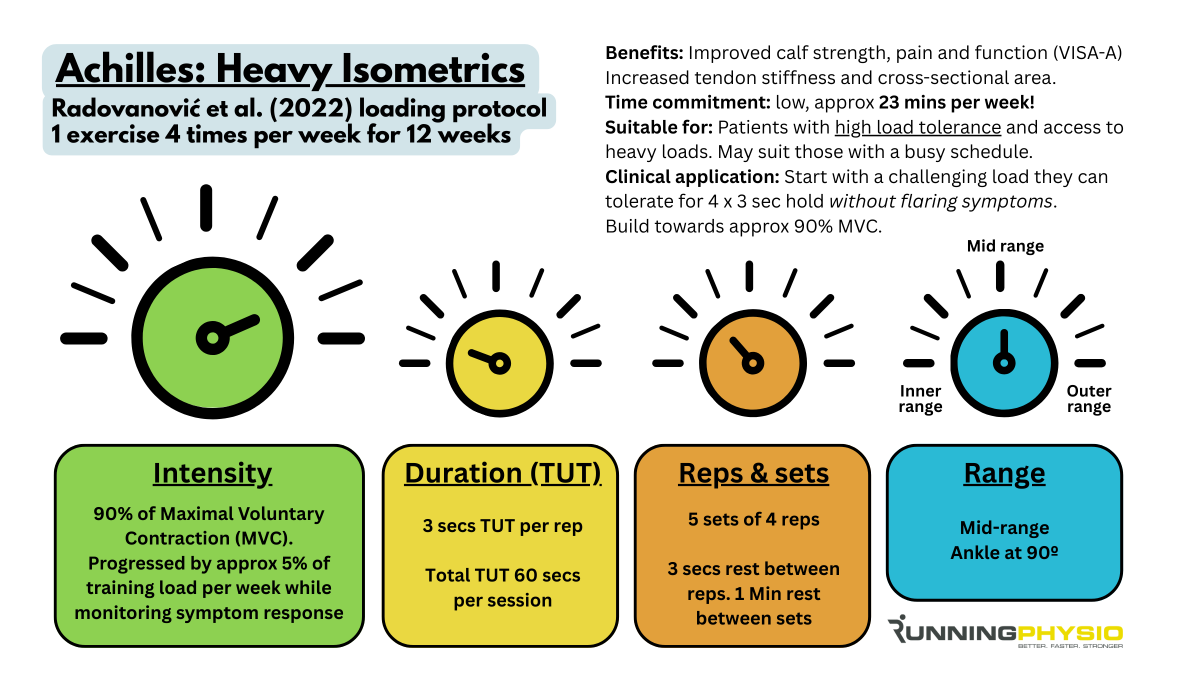
The heavy isometric programme for Achilles Tendinopathy from Radovanonić et al. (2022) has somewhat gone under the radar but has lots of potential benefits 💪
It’s just one exercise and takes less than 25 mins per week!
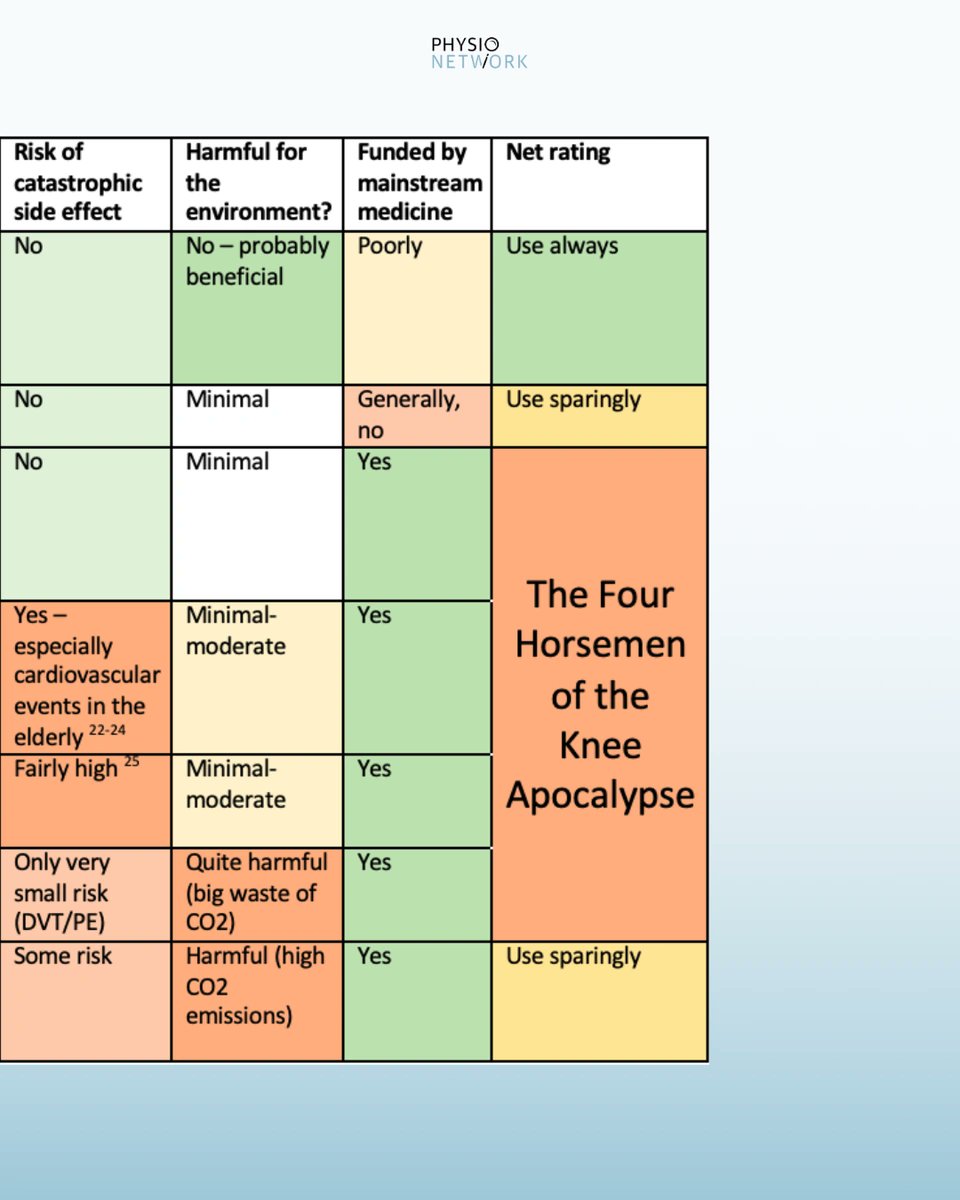
Risks & benefits of knee OA treatments
👉🏻 Swipe to have a closer look at this table
This is taken from a great blog on OA by @DrJohnOrchard for BJSM
“The evidence for KT is highly inconclusive & of very low certainty. While it may serve as a useful adjunctive therapy for immediate pain relief, it lacks impact on objective kinematic outcomes like strength and ROM.”
128 systematic reviews. 78% having critically low quality
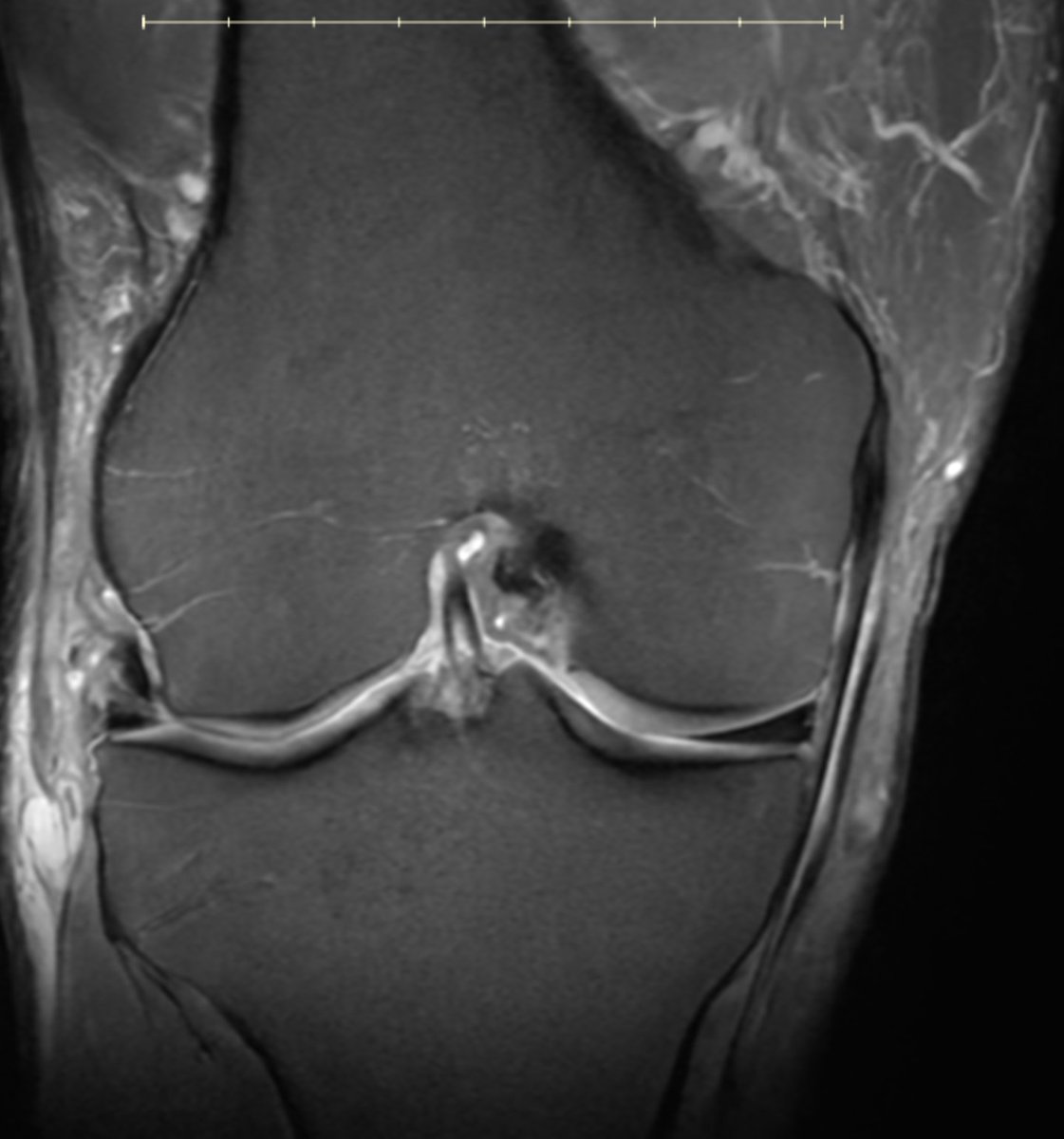
60 yo runner. Also lifts 3x/week. Stable lateral meniscus tear and a small cartilage defect for 10 years. New pain.. worse. Mostly anterior, anterolateral. Pain with loading, jumping, etc... but on landing, not the jump. in other words... axial load hurts.
New MRI: mostly anterior BME deep to PT insertion.
Stress reaction from the tendon or load??