Aripiprazole LAIs are often framed as an adherence solution in schizophrenia.
But clinically, they are more than “oral aripiprazole in injection form.”
To use Abilify Maintena or Aristada well, clinicians need to understand partial agonism, plasma exposure, oral overlap, and CYP interactions. 🧵👇
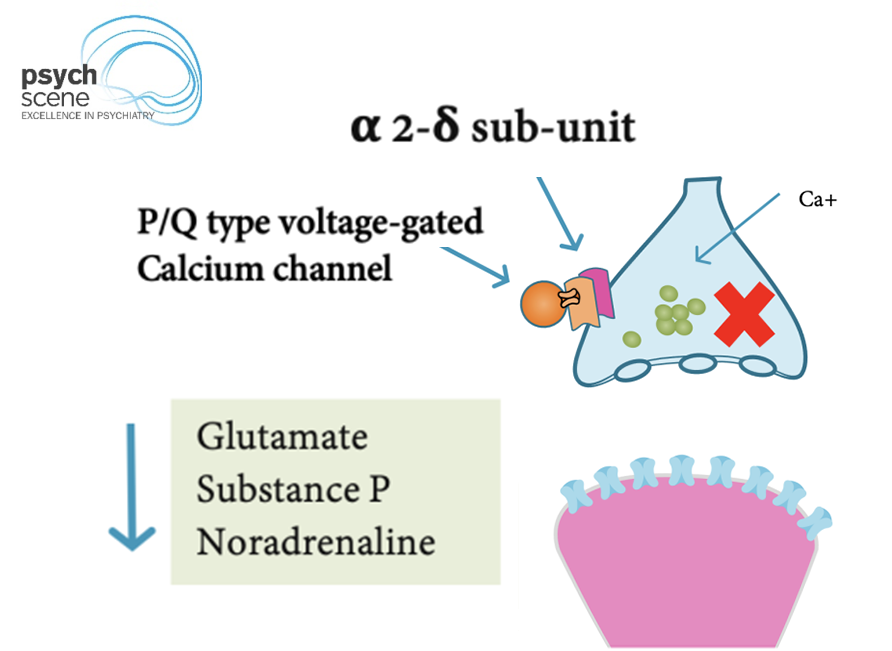
Gabapentin and pregabalin are often described as “GABA-like.”
But clinically, that can be misleading.
They do not act by binding to GABA receptors.
To understand their role in psychiatry, let's start with what gabapentinoids actually do. 🧵👇
Desde que Salud Digna ofrece USG de tiroides por 100 pesitos, tengo muchísimos px en lista de espera súper espantados por los "hallazgos"
Colegas, ayúdenme a orientarlos y evitar que caigan en manos de cirujanos mano larga.
Por eso les traigo hilo de nódulo tiroideo:
🧵
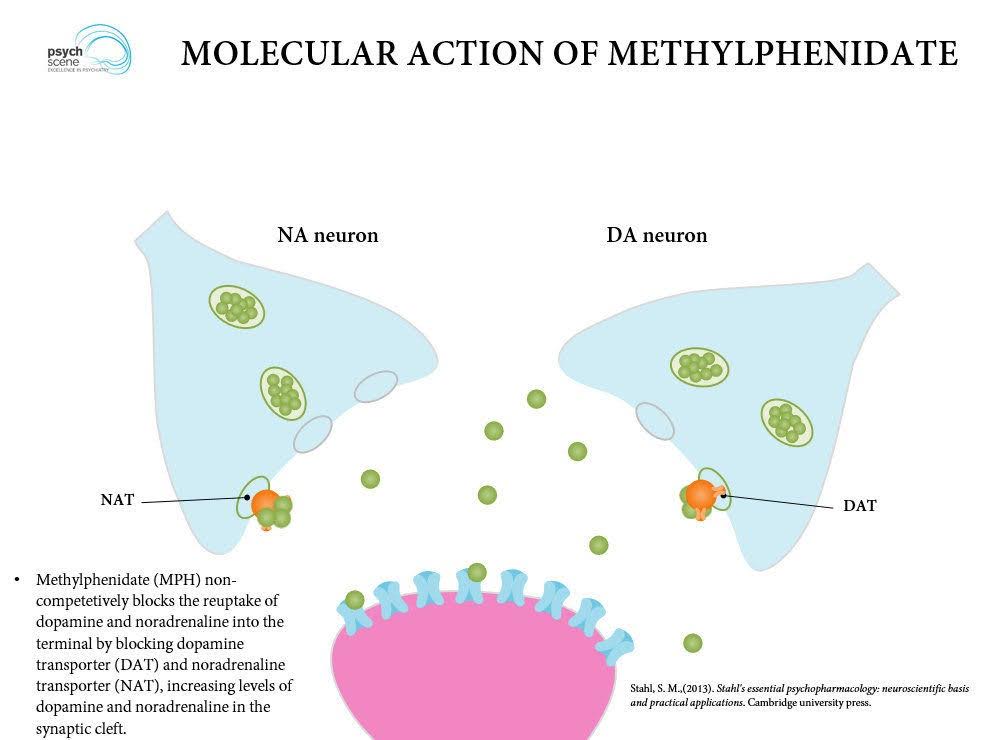
Methylphenidate is not simply “a stimulant.”
Its clinical effect depends on how dopamine and noradrenaline are increased, released, sustained, and worn off.
That is where formulation choice becomes clinically important. 🧵👇
Cambios relevantes en SII según Roma V
- Reincorpora discomfort abdominal (además del dolor)
- Frecuencia 3 días al mes por 3 meses (antes 1 día a la semana)
- Dolor abdominal intermitente, no continuo (diferenciándolo de origen central)
- Trastornos de interacción intestino-cerebro (antes “funcionales”)
Gastroenterology 2026;170:1083–1098
🧠💔 El mayor error en depresión:
creer que es solo “falta de serotonina”.
No lo es.
Es una enfermedad:
endocrina, inflamatoria, metabólica y circadiana.
Y esto cambia TODO.
🧵👇
Ayer tuve un paciente que me preguntó por qué la presión arterial parece ir a peor con los años, incluso cuando “se cuida”.
Se lo expliqué en consulta, pero como es un tema padrísimo, voy a hacer un hilo. Será largo, como siempre… pero es para quienes disfrutan entender estas cosas. 🤓 🧵
🧠 Neurology - Concepts you should never forget : 2️⃣
🟢Cortical vs Subcortical stroke
Let’s break it down step-by-step. 👇
🟦 1️⃣ What is a Cortical Stroke?
A cortical stroke involves the cerebral cortex the outer layer of the brain responsible for higher neurological functions.
Key cortical areas include:
🔻 Frontal lobe → motor control, executive function, speech production (Broca)
🔻 Parietal lobe → sensory perception & spatial awareness
🔻 Temporal lobe → auditory processing, language comprehension (Wernicke), memory
🔻 Occipital lobe → vision
When these higher cortical functions are affected → it strongly suggests cortical involvement.
Most commonly affected vessels:
🔻 Middle Cerebral Artery (MCA) mc
🔻 Anterior Cerebral Artery (ACA)
🔻 Posterior Cerebral Artery (PCA)
These are typically large vessel strokes.
🟦 2️⃣ Clinical clues of a Cortical Stroke
Because the cortex handles complex processing, strokes here produce cortical signs.
Look for:
🔻 Aphasia (dominant hemisphere language dysfunction)
🔻 Neglect (classically right parietal cortex)
🔻 Visual field defects (homonymous hemianopia)
🔻 Gaze deviation
🔻 Apraxia or agnosia
🔻 Cortical sensory loss (astereognosis, agraphesthesia)
🔻 Early seizures
Weakness may occur, but cortical signs usually accompany it.
🟦 3️⃣ What is a Subcortical Stroke?
A subcortical stroke affects deep brain structures beneath the cortex.
Common locations include:
🔻 Internal capsule
🔻 Basal ganglia
🔻 Thalamus
🔻 Pons
These areas mainly carry motor and sensory pathways but do not control higher cortical functions like language or spatial awareness.
🟦 4️⃣ Blood vessels involved in Subcortical stroke
These strokes involve small penetrating arteries, such as:
🔻 Lenticulostriate arteries (branch of MCA)
🔻 Thalamoperforators (branch of PCA)
🔻 Anterior choroidal artery (branch of ICA)
🔻 Paramedian pontine perforators
This is why they are called lacunar strokes.
Most commonly caused by:
➡️ Chronic hypertension or diabetes
➡️ Small vessel disease due to lipohyalinosis or microatheroma
🟦 5️⃣ Lacunar strokes: The classic “3 NO’s”
A quick way to localize small vessel (subcortical) stroke is remembering the 3 NO’s:
❌ No cortical symptoms
Meaning no:
• aphasia
• neglect
• visual field defects
• gaze deviation
❌ No higher cortical dysfunction
Meaning:
• language intact
• cognition preserved
• no behavioral changes
Because the cortex is spared, deficits are usually pure motor or sensory.
🟦 6️⃣ Clinical patterns of Subcortical (lacunar) stroke
Classic lacunar syndromes include:
🔻 Pure motor hemiparesis (internal capsule)
🔻 Pure sensory stroke (thalamus)
🔻 Sensorimotor stroke
🔻 Ataxic hemiparesis
🔻 Dysarthria–clumsy hand syndrome
🟦 7️⃣ The 10-second bedside trick
When a patient presents with weakness, ask yourself 4 quick questions:
1️⃣ Is language affected?
2️⃣ Is there neglect?
3️⃣ Is there visual field loss?
4️⃣ Is there gaze deviation?
If any of these are present → think cortical stroke.
If none are present → think lacunar / small vessel stroke.
🟦 8️⃣ Language test
Ask the patient to repeat a sentence or name objects.
Example:
🗣 “No ifs, ands, or buts.”
If speech is impaired → aphasia → cortical stroke
Language centers lie in the dominant cerebral cortex.
🟦 9️⃣ Neglect test
Ask the patient to raise both limbs or perform simultaneous sensory stimulation.
If they ignore one side → hemispatial neglect
This is classic for right parietal cortical stroke.
Subcortical strokes rarely produce neglect.
#MedTwitter #MedX #NeuroTwitter
Revisión de diarrea crónica no infecciosa, en JAMA (Feb 2026). Puntos clave:
🔵 La diarrea crónica se define como heces laxas o acuosas por más de 4 semanas. Más del 90% de los casos son de origen no infeccioso, siendo el SII-D y la diarrea funcional las causas predominantes.
🔵 Todo abordaje debe incluir biometría hemática (para detectar anemia), calprotectina fecal (para descartar EII) y serología para enfermedad celíaca mediante IgA-tTG junto con niveles de IgA total.
🔵Realizar colonoscopia con biopsias y endoscopia superior en pacientes de 45 años o más, o ante la presencia de signos de alarma: pérdida de peso, sangrado rectal, anemia ferropénica, esteatorrea o diarrea nocturna.
🔵 Para SII, el manejo inicial se basa en higiene dietética y una dieta baja en FODMAP. Como fármacos de primera línea se recomiendan loperamida, antiespasmódicos y antagonistas de 5-HT₃ como el ondansetrón.
Vamos a revisarla a fondo para las apps (https://t.co/O3HpYX0dAx). Lo subí al canal (https://t.co/3O93s10lns).
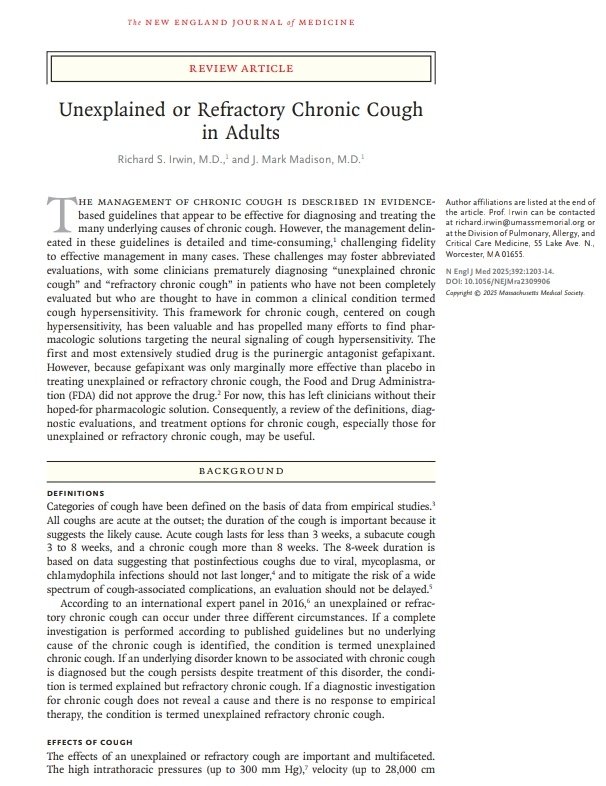
💎Abordaje de la Tos Crónica Refractaria en el Paciente Adulto 🗣️
🔰📚N Engl J Med 2025
DOI: 10.1056/NEJMra2309906
Enlace a Articulo Completo👇🏼🆓✅
https://t.co/rPEDXf65lm
Hyperparathyroidism (HPT) is a condition where the parathyroid glands produce excessive parathyroid hormone (PTH), disrupting the body's calcium and phosphate balance.
A study guide from Pathology Navigator detailing the four key types of hyperparathyroidism.
https://t.co/guwXqsZqho
🚨🧠𝗦𝘁𝗮𝘁𝘂𝘀 𝗘𝗽𝗶𝗹𝗲𝗽𝘁𝗶𝗰𝘂𝘀 (𝗦𝗘): “𝘁𝗶𝗺𝗲 𝗶𝘀 𝗯𝗿𝗮𝗶𝗻”⏱️⚡️
@sciencedirect
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
📌SE = crisis prolongada o crisis repetidas 𝙨𝙞𝙣 𝙧𝙚𝙘𝙪𝙥𝙚𝙧𝙖𝙧 𝙡𝙞𝙣𝙚𝙖 𝙙𝙚 𝙗𝙖𝙨𝙚 🧠🌀.
Hoy se considera SE si:
⏱️ ≥𝟱 𝙢𝙞𝙣 convulsivo continuo, o ≥𝟭𝟬 𝙢𝙞𝙣 focal con alteración de conciencia, o 𝟭𝟬–𝟭𝟱 𝙢𝙞𝙣 ausencias.
👉 Después de esos tiempos, la probabilidad de que pare sola es baja 😬 y hay riesgo de lesión neuronal 🔥.
🧠🧬 𝙋𝙤𝙧 𝙦𝙪𝙚́ 𝙪𝙧𝙜𝙚: 𝙛𝙖𝙧𝙢𝙖𝙘𝙤𝙧𝙧𝙚𝙨𝙞𝙨𝙩𝙚𝙣𝙘𝙞𝙖 + 𝙡𝙚𝙨𝙞𝙤́𝙣 𝙣𝙚𝙪𝙧𝙤𝙣𝙖𝙡 🧨
En minutos ocurre:
⬇️ 𝙞𝙣𝙩𝙚𝙧𝙣𝙖𝙡𝙞𝙯𝙖𝙘𝙞𝙤́𝙣 𝙙𝙚 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙂𝘼𝘽𝘼 (↓ respuesta a benzos 😱)
⬆️ 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙉𝙈𝘿𝘼/𝙜𝙡𝙪𝙩𝙖𝙢𝙖𝙩𝙤 (más excitación ⚡️)
➡️ SE puede causar apoptosis/necrosis, disfunción mitocondrial 🔋⬇️, acidosis, hipoxia, hipotensión… incluso en NCSE 🧠🩸.
🛟 𝘼𝘽𝘾 + 𝟮 “𝙢𝙪𝙨𝙩” 𝙞𝙣𝙢𝙚𝙙𝙞𝙖𝙩𝙤𝙨 ✅✅
Antes (y durante) el fármaco:
🫁 A/B/C: oxígeno, posición lateral, BVM si apnea 😮💨
🩸 𝙂𝙡𝙪𝙘𝙤𝙨𝙖 𝙘𝙖𝙥𝙞𝙡𝙖𝙧 𝙎𝙄𝙀𝙈𝙋𝙍𝙀 🍬📉
🤰 𝙋𝙧𝙪𝙚𝙗𝙖 𝙙𝙚 𝙚𝙢𝙗𝙖𝙧𝙖𝙯𝙤 en mujeres en edad fértil ✅
⚠️ Considera 𝙝𝙞𝙥𝙤𝙣𝙖𝙩𝙧𝙚𝙢𝙞𝙖 𝙨𝙚𝙫𝙚𝙧𝙖 como causa reversible: si Na muy bajo + convulsión → 𝟯% 𝟭𝟬𝟬–𝟭𝟱𝟬 𝙢𝙇 en 10 min (repetible hasta 2 veces) 🧂💉.
💉🥇 𝟭ª 𝙡𝙞́𝙣𝙚𝙖: 𝘽𝙀𝙉𝙕𝙊𝘿𝙄𝘼𝘾𝙀𝙋𝙄𝙉𝘼𝙎 𝙗𝙞𝙚𝙣 𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙙𝙖𝙨 (𝙮 𝙧𝙖́𝙥𝙞𝙙𝙤) ⚡️
El mayor error es 𝙨𝙪𝙗𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙧 😬 (¡pasa mucho!).
Opciones eficaces:
💉 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 𝙄𝙈 𝟬.𝟯–𝟬.𝟱 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
💉 𝙇𝙤𝙧𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟭 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰 𝙢𝙜)
💉 𝘿𝙞𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟮 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
🔁 Si continúa: repetir una vez a los 𝟱 𝙢𝙞𝙣 ⏱️
👉 IM midazolam puede ser superior si no hay IV (se da antes) 🚑⚡️.
💊🥈 𝟮ª 𝙡𝙞́𝙣𝙚𝙖 (𝟮𝟬–𝟰𝟬 𝙢𝙞𝙣): “𝙀𝙎𝙀𝙏𝙏 = 𝙚𝙢𝙥𝙖𝙩𝙚” ⚖️
Si persiste tras benzos → 𝙎𝙀 𝙚𝙨𝙩𝙖𝙗𝙡𝙚𝙘𝙞𝙙𝙤:
✅ 𝙇𝙚𝙫𝙚𝙩𝙞𝙧𝙖𝙘𝙚𝙩𝙖𝙢 𝟲𝟬 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰𝟱𝟬𝟬 𝙢𝙜) 🚀
✅ 𝙑𝙖𝙡𝙥𝙧𝙤𝙖𝙩𝙤 𝟰𝟬 𝙢𝙜/𝙠𝙜 (𝗺𝗮́𝘅 𝟯𝟬𝟬𝟬 𝙢𝙜; +𝟮𝟬 𝙢𝙜/𝙠𝙜 𝙚𝙭𝙩𝙧𝙖 𝙥𝙤𝙨𝙞𝙗𝙡𝙚)
✅ 𝙁𝙤𝙨𝙛𝙚𝙣𝙞𝙩𝙤𝙞́𝙣𝙖 𝟮𝟬 𝙢𝙜𝙋𝙀/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟱𝟬𝟬 𝙢𝙜𝙋𝙀)
📌 ESETT: 𝙨𝙞𝙣 𝙙𝙞𝙛𝙚𝙧𝙚𝙣𝙘𝙞𝙖 𝙘𝙡𝙖𝙧𝙖 entre estos 3 si se usan a dosis correctas.
🧯🥉 𝙍𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤: 𝙖𝙣𝙚𝙨𝙩𝙚𝙨𝙞𝙖 + 𝙞𝙣𝙩𝙪𝙗𝙖𝙘𝙞𝙤́𝙣 + 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 🛌🧠📉
Si sigue tras benzos + 2 ASM → 𝙧𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤 😱
➡️ intubar + infusión anestésica:
🟣 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 bolos + infusión
🟠 𝙋𝙧𝙤𝙥𝙤𝙛𝙤𝙡 bolos + infusión
🟢 𝙆𝙚𝙩𝙖𝙢𝙞𝙣𝙖 (NMDA) = atractiva por farmacorresistencia + mejor perfil hemodinámico 💪🫀
🧠 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 para titular y detectar NCSE ✅.
🫥🧠 𝙉𝘾𝙎𝙀: 𝙡𝙖 𝙘𝙖𝙪𝙨𝙖 𝙤𝙘𝙪𝙡𝙩𝙖 𝙙𝙚𝙡 “𝙘𝙤𝙢𝙖 𝙞𝙣𝙚𝙭𝙥𝙡𝙞𝙘𝙖𝙙𝙤” 👀⚠️
NCSE es común en UCI y puede presentarse como:
😵💫 confusión/agitación | 😶🌫️ estupor/coma | 👁️ movimientos oculares anómalos | 🤖 automatismos
📌 33–46% viene tras convulsivo inicial; y puede progresar a refractario.
✅ Indicaciones prácticas de EEG continuo:
•todo intubado por SE
•no mejora alerta en 10 min o sigue alterado >30 min tras parar convulsión.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más #MedED en #ClubCrit 😄🧠🫶
📚📖 Más en el blog #ClubCrit 👉 [https://t.co/wbCJFKHCXL]
#Neurocritical #NeuroX #NeuroICU #Neurocritical #StatusEpilepticus #Neurology #EEG #POCUS #BNP #HeartFailure #Radiology #Dyspnea #POCUS #LungUltrasound #JVP #ICU #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #Diagnóstico #icu #intensivecare #diagnosis #management #UCI #Tratamiento #MedicinaBasadaEnEvidencia #POCUS #MedEd #Medicina #Emergencias #FOAMed #FOAMcc #MedX #IntensiveCare #EducaciónMédica #MedIntensiva #MedXCommunity #MedicinaCrítica #MedED #CritCare #ICUmanagement #MustRead #LecturaRecomendada

















![MarlonVFZR's tweet photo. 🚨🧠𝗦𝘁𝗮𝘁𝘂𝘀 𝗘𝗽𝗶𝗹𝗲𝗽𝘁𝗶𝗰𝘂𝘀 (𝗦𝗘): “𝘁𝗶𝗺𝗲 𝗶𝘀 𝗯𝗿𝗮𝗶𝗻”⏱️⚡️
@sciencedirect
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
📌SE = crisis prolongada o crisis repetidas 𝙨𝙞𝙣 𝙧𝙚𝙘𝙪𝙥𝙚𝙧𝙖𝙧 𝙡𝙞𝙣𝙚𝙖 𝙙𝙚 𝙗𝙖𝙨𝙚 🧠🌀.
Hoy se considera SE si:
⏱️ ≥𝟱 𝙢𝙞𝙣 convulsivo continuo, o ≥𝟭𝟬 𝙢𝙞𝙣 focal con alteración de conciencia, o 𝟭𝟬–𝟭𝟱 𝙢𝙞𝙣 ausencias.
👉 Después de esos tiempos, la probabilidad de que pare sola es baja 😬 y hay riesgo de lesión neuronal 🔥.
🧠🧬 𝙋𝙤𝙧 𝙦𝙪𝙚́ 𝙪𝙧𝙜𝙚: 𝙛𝙖𝙧𝙢𝙖𝙘𝙤𝙧𝙧𝙚𝙨𝙞𝙨𝙩𝙚𝙣𝙘𝙞𝙖 + 𝙡𝙚𝙨𝙞𝙤́𝙣 𝙣𝙚𝙪𝙧𝙤𝙣𝙖𝙡 🧨
En minutos ocurre:
⬇️ 𝙞𝙣𝙩𝙚𝙧𝙣𝙖𝙡𝙞𝙯𝙖𝙘𝙞𝙤́𝙣 𝙙𝙚 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙂𝘼𝘽𝘼 (↓ respuesta a benzos 😱)
⬆️ 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙉𝙈𝘿𝘼/𝙜𝙡𝙪𝙩𝙖𝙢𝙖𝙩𝙤 (más excitación ⚡️)
➡️ SE puede causar apoptosis/necrosis, disfunción mitocondrial 🔋⬇️, acidosis, hipoxia, hipotensión… incluso en NCSE 🧠🩸.
🛟 𝘼𝘽𝘾 + 𝟮 “𝙢𝙪𝙨𝙩” 𝙞𝙣𝙢𝙚𝙙𝙞𝙖𝙩𝙤𝙨 ✅✅
Antes (y durante) el fármaco:
🫁 A/B/C: oxígeno, posición lateral, BVM si apnea 😮💨
🩸 𝙂𝙡𝙪𝙘𝙤𝙨𝙖 𝙘𝙖𝙥𝙞𝙡𝙖𝙧 𝙎𝙄𝙀𝙈𝙋𝙍𝙀 🍬📉
🤰 𝙋𝙧𝙪𝙚𝙗𝙖 𝙙𝙚 𝙚𝙢𝙗𝙖𝙧𝙖𝙯𝙤 en mujeres en edad fértil ✅
⚠️ Considera 𝙝𝙞𝙥𝙤𝙣𝙖𝙩𝙧𝙚𝙢𝙞𝙖 𝙨𝙚𝙫𝙚𝙧𝙖 como causa reversible: si Na muy bajo + convulsión → 𝟯% 𝟭𝟬𝟬–𝟭𝟱𝟬 𝙢𝙇 en 10 min (repetible hasta 2 veces) 🧂💉.
💉🥇 𝟭ª 𝙡𝙞́𝙣𝙚𝙖: 𝘽𝙀𝙉𝙕𝙊𝘿𝙄𝘼𝘾𝙀𝙋𝙄𝙉𝘼𝙎 𝙗𝙞𝙚𝙣 𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙙𝙖𝙨 (𝙮 𝙧𝙖́𝙥𝙞𝙙𝙤) ⚡️
El mayor error es 𝙨𝙪𝙗𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙧 😬 (¡pasa mucho!).
Opciones eficaces:
💉 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 𝙄𝙈 𝟬.𝟯–𝟬.𝟱 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
💉 𝙇𝙤𝙧𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟭 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰 𝙢𝙜)
💉 𝘿𝙞𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟮 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
🔁 Si continúa: repetir una vez a los 𝟱 𝙢𝙞𝙣 ⏱️
👉 IM midazolam puede ser superior si no hay IV (se da antes) 🚑⚡️.
💊🥈 𝟮ª 𝙡𝙞́𝙣𝙚𝙖 (𝟮𝟬–𝟰𝟬 𝙢𝙞𝙣): “𝙀𝙎𝙀𝙏𝙏 = 𝙚𝙢𝙥𝙖𝙩𝙚” ⚖️
Si persiste tras benzos → 𝙎𝙀 𝙚𝙨𝙩𝙖𝙗𝙡𝙚𝙘𝙞𝙙𝙤:
✅ 𝙇𝙚𝙫𝙚𝙩𝙞𝙧𝙖𝙘𝙚𝙩𝙖𝙢 𝟲𝟬 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰𝟱𝟬𝟬 𝙢𝙜) 🚀
✅ 𝙑𝙖𝙡𝙥𝙧𝙤𝙖𝙩𝙤 𝟰𝟬 𝙢𝙜/𝙠𝙜 (𝗺𝗮́𝘅 𝟯𝟬𝟬𝟬 𝙢𝙜; +𝟮𝟬 𝙢𝙜/𝙠𝙜 𝙚𝙭𝙩𝙧𝙖 𝙥𝙤𝙨𝙞𝙗𝙡𝙚)
✅ 𝙁𝙤𝙨𝙛𝙚𝙣𝙞𝙩𝙤𝙞́𝙣𝙖 𝟮𝟬 𝙢𝙜𝙋𝙀/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟱𝟬𝟬 𝙢𝙜𝙋𝙀)
📌 ESETT: 𝙨𝙞𝙣 𝙙𝙞𝙛𝙚𝙧𝙚𝙣𝙘𝙞𝙖 𝙘𝙡𝙖𝙧𝙖 entre estos 3 si se usan a dosis correctas.
🧯🥉 𝙍𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤: 𝙖𝙣𝙚𝙨𝙩𝙚𝙨𝙞𝙖 + 𝙞𝙣𝙩𝙪𝙗𝙖𝙘𝙞𝙤́𝙣 + 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 🛌🧠📉
Si sigue tras benzos + 2 ASM → 𝙧𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤 😱
➡️ intubar + infusión anestésica:
🟣 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 bolos + infusión
🟠 𝙋𝙧𝙤𝙥𝙤𝙛𝙤𝙡 bolos + infusión
🟢 𝙆𝙚𝙩𝙖𝙢𝙞𝙣𝙖 (NMDA) = atractiva por farmacorresistencia + mejor perfil hemodinámico 💪🫀
🧠 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 para titular y detectar NCSE ✅.
🫥🧠 𝙉𝘾𝙎𝙀: 𝙡𝙖 𝙘𝙖𝙪𝙨𝙖 𝙤𝙘𝙪𝙡𝙩𝙖 𝙙𝙚𝙡 “𝙘𝙤𝙢𝙖 𝙞𝙣𝙚𝙭𝙥𝙡𝙞𝙘𝙖𝙙𝙤” 👀⚠️
NCSE es común en UCI y puede presentarse como:
😵💫 confusión/agitación | 😶🌫️ estupor/coma | 👁️ movimientos oculares anómalos | 🤖 automatismos
📌 33–46% viene tras convulsivo inicial; y puede progresar a refractario.
✅ Indicaciones prácticas de EEG continuo:
•todo intubado por SE
•no mejora alerta en 10 min o sigue alterado >30 min tras parar convulsión.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más #MedED en #ClubCrit 😄🧠🫶
📚📖 Más en el blog #ClubCrit 👉 [https://t.co/wbCJFKHCXL]
#Neurocritical #NeuroX #NeuroICU #Neurocritical #StatusEpilepticus #Neurology #EEG #POCUS #BNP #HeartFailure #Radiology #Dyspnea #POCUS #LungUltrasound #JVP #ICU #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #Diagnóstico #icu #intensivecare #diagnosis #management #UCI #Tratamiento #MedicinaBasadaEnEvidencia #POCUS #MedEd #Medicina #Emergencias #FOAMed #FOAMcc #MedX #IntensiveCare #EducaciónMédica #MedIntensiva #MedXCommunity #MedicinaCrítica #MedED #CritCare #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HCKorm3XkAANPCD.jpg)
![MarlonVFZR's tweet photo. 🚨🧠𝗦𝘁𝗮𝘁𝘂𝘀 𝗘𝗽𝗶𝗹𝗲𝗽𝘁𝗶𝗰𝘂𝘀 (𝗦𝗘): “𝘁𝗶𝗺𝗲 𝗶𝘀 𝗯𝗿𝗮𝗶𝗻”⏱️⚡️
@sciencedirect
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
📌SE = crisis prolongada o crisis repetidas 𝙨𝙞𝙣 𝙧𝙚𝙘𝙪𝙥𝙚𝙧𝙖𝙧 𝙡𝙞𝙣𝙚𝙖 𝙙𝙚 𝙗𝙖𝙨𝙚 🧠🌀.
Hoy se considera SE si:
⏱️ ≥𝟱 𝙢𝙞𝙣 convulsivo continuo, o ≥𝟭𝟬 𝙢𝙞𝙣 focal con alteración de conciencia, o 𝟭𝟬–𝟭𝟱 𝙢𝙞𝙣 ausencias.
👉 Después de esos tiempos, la probabilidad de que pare sola es baja 😬 y hay riesgo de lesión neuronal 🔥.
🧠🧬 𝙋𝙤𝙧 𝙦𝙪𝙚́ 𝙪𝙧𝙜𝙚: 𝙛𝙖𝙧𝙢𝙖𝙘𝙤𝙧𝙧𝙚𝙨𝙞𝙨𝙩𝙚𝙣𝙘𝙞𝙖 + 𝙡𝙚𝙨𝙞𝙤́𝙣 𝙣𝙚𝙪𝙧𝙤𝙣𝙖𝙡 🧨
En minutos ocurre:
⬇️ 𝙞𝙣𝙩𝙚𝙧𝙣𝙖𝙡𝙞𝙯𝙖𝙘𝙞𝙤́𝙣 𝙙𝙚 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙂𝘼𝘽𝘼 (↓ respuesta a benzos 😱)
⬆️ 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙉𝙈𝘿𝘼/𝙜𝙡𝙪𝙩𝙖𝙢𝙖𝙩𝙤 (más excitación ⚡️)
➡️ SE puede causar apoptosis/necrosis, disfunción mitocondrial 🔋⬇️, acidosis, hipoxia, hipotensión… incluso en NCSE 🧠🩸.
🛟 𝘼𝘽𝘾 + 𝟮 “𝙢𝙪𝙨𝙩” 𝙞𝙣𝙢𝙚𝙙𝙞𝙖𝙩𝙤𝙨 ✅✅
Antes (y durante) el fármaco:
🫁 A/B/C: oxígeno, posición lateral, BVM si apnea 😮💨
🩸 𝙂𝙡𝙪𝙘𝙤𝙨𝙖 𝙘𝙖𝙥𝙞𝙡𝙖𝙧 𝙎𝙄𝙀𝙈𝙋𝙍𝙀 🍬📉
🤰 𝙋𝙧𝙪𝙚𝙗𝙖 𝙙𝙚 𝙚𝙢𝙗𝙖𝙧𝙖𝙯𝙤 en mujeres en edad fértil ✅
⚠️ Considera 𝙝𝙞𝙥𝙤𝙣𝙖𝙩𝙧𝙚𝙢𝙞𝙖 𝙨𝙚𝙫𝙚𝙧𝙖 como causa reversible: si Na muy bajo + convulsión → 𝟯% 𝟭𝟬𝟬–𝟭𝟱𝟬 𝙢𝙇 en 10 min (repetible hasta 2 veces) 🧂💉.
💉🥇 𝟭ª 𝙡𝙞́𝙣𝙚𝙖: 𝘽𝙀𝙉𝙕𝙊𝘿𝙄𝘼𝘾𝙀𝙋𝙄𝙉𝘼𝙎 𝙗𝙞𝙚𝙣 𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙙𝙖𝙨 (𝙮 𝙧𝙖́𝙥𝙞𝙙𝙤) ⚡️
El mayor error es 𝙨𝙪𝙗𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙧 😬 (¡pasa mucho!).
Opciones eficaces:
💉 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 𝙄𝙈 𝟬.𝟯–𝟬.𝟱 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
💉 𝙇𝙤𝙧𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟭 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰 𝙢𝙜)
💉 𝘿𝙞𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟮 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
🔁 Si continúa: repetir una vez a los 𝟱 𝙢𝙞𝙣 ⏱️
👉 IM midazolam puede ser superior si no hay IV (se da antes) 🚑⚡️.
💊🥈 𝟮ª 𝙡𝙞́𝙣𝙚𝙖 (𝟮𝟬–𝟰𝟬 𝙢𝙞𝙣): “𝙀𝙎𝙀𝙏𝙏 = 𝙚𝙢𝙥𝙖𝙩𝙚” ⚖️
Si persiste tras benzos → 𝙎𝙀 𝙚𝙨𝙩𝙖𝙗𝙡𝙚𝙘𝙞𝙙𝙤:
✅ 𝙇𝙚𝙫𝙚𝙩𝙞𝙧𝙖𝙘𝙚𝙩𝙖𝙢 𝟲𝟬 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰𝟱𝟬𝟬 𝙢𝙜) 🚀
✅ 𝙑𝙖𝙡𝙥𝙧𝙤𝙖𝙩𝙤 𝟰𝟬 𝙢𝙜/𝙠𝙜 (𝗺𝗮́𝘅 𝟯𝟬𝟬𝟬 𝙢𝙜; +𝟮𝟬 𝙢𝙜/𝙠𝙜 𝙚𝙭𝙩𝙧𝙖 𝙥𝙤𝙨𝙞𝙗𝙡𝙚)
✅ 𝙁𝙤𝙨𝙛𝙚𝙣𝙞𝙩𝙤𝙞́𝙣𝙖 𝟮𝟬 𝙢𝙜𝙋𝙀/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟱𝟬𝟬 𝙢𝙜𝙋𝙀)
📌 ESETT: 𝙨𝙞𝙣 𝙙𝙞𝙛𝙚𝙧𝙚𝙣𝙘𝙞𝙖 𝙘𝙡𝙖𝙧𝙖 entre estos 3 si se usan a dosis correctas.
🧯🥉 𝙍𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤: 𝙖𝙣𝙚𝙨𝙩𝙚𝙨𝙞𝙖 + 𝙞𝙣𝙩𝙪𝙗𝙖𝙘𝙞𝙤́𝙣 + 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 🛌🧠📉
Si sigue tras benzos + 2 ASM → 𝙧𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤 😱
➡️ intubar + infusión anestésica:
🟣 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 bolos + infusión
🟠 𝙋𝙧𝙤𝙥𝙤𝙛𝙤𝙡 bolos + infusión
🟢 𝙆𝙚𝙩𝙖𝙢𝙞𝙣𝙖 (NMDA) = atractiva por farmacorresistencia + mejor perfil hemodinámico 💪🫀
🧠 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 para titular y detectar NCSE ✅.
🫥🧠 𝙉𝘾𝙎𝙀: 𝙡𝙖 𝙘𝙖𝙪𝙨𝙖 𝙤𝙘𝙪𝙡𝙩𝙖 𝙙𝙚𝙡 “𝙘𝙤𝙢𝙖 𝙞𝙣𝙚𝙭𝙥𝙡𝙞𝙘𝙖𝙙𝙤” 👀⚠️
NCSE es común en UCI y puede presentarse como:
😵💫 confusión/agitación | 😶🌫️ estupor/coma | 👁️ movimientos oculares anómalos | 🤖 automatismos
📌 33–46% viene tras convulsivo inicial; y puede progresar a refractario.
✅ Indicaciones prácticas de EEG continuo:
•todo intubado por SE
•no mejora alerta en 10 min o sigue alterado >30 min tras parar convulsión.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más #MedED en #ClubCrit 😄🧠🫶
📚📖 Más en el blog #ClubCrit 👉 [https://t.co/wbCJFKHCXL]
#Neurocritical #NeuroX #NeuroICU #Neurocritical #StatusEpilepticus #Neurology #EEG #POCUS #BNP #HeartFailure #Radiology #Dyspnea #POCUS #LungUltrasound #JVP #ICU #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #Diagnóstico #icu #intensivecare #diagnosis #management #UCI #Tratamiento #MedicinaBasadaEnEvidencia #POCUS #MedEd #Medicina #Emergencias #FOAMed #FOAMcc #MedX #IntensiveCare #EducaciónMédica #MedIntensiva #MedXCommunity #MedicinaCrítica #MedED #CritCare #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HCKorj6XYAIqRLp.jpg)
![MarlonVFZR's tweet photo. 🚨🧠𝗦𝘁𝗮𝘁𝘂𝘀 𝗘𝗽𝗶𝗹𝗲𝗽𝘁𝗶𝗰𝘂𝘀 (𝗦𝗘): “𝘁𝗶𝗺𝗲 𝗶𝘀 𝗯𝗿𝗮𝗶𝗻”⏱️⚡️
@sciencedirect
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
📌SE = crisis prolongada o crisis repetidas 𝙨𝙞𝙣 𝙧𝙚𝙘𝙪𝙥𝙚𝙧𝙖𝙧 𝙡𝙞𝙣𝙚𝙖 𝙙𝙚 𝙗𝙖𝙨𝙚 🧠🌀.
Hoy se considera SE si:
⏱️ ≥𝟱 𝙢𝙞𝙣 convulsivo continuo, o ≥𝟭𝟬 𝙢𝙞𝙣 focal con alteración de conciencia, o 𝟭𝟬–𝟭𝟱 𝙢𝙞𝙣 ausencias.
👉 Después de esos tiempos, la probabilidad de que pare sola es baja 😬 y hay riesgo de lesión neuronal 🔥.
🧠🧬 𝙋𝙤𝙧 𝙦𝙪𝙚́ 𝙪𝙧𝙜𝙚: 𝙛𝙖𝙧𝙢𝙖𝙘𝙤𝙧𝙧𝙚𝙨𝙞𝙨𝙩𝙚𝙣𝙘𝙞𝙖 + 𝙡𝙚𝙨𝙞𝙤́𝙣 𝙣𝙚𝙪𝙧𝙤𝙣𝙖𝙡 🧨
En minutos ocurre:
⬇️ 𝙞𝙣𝙩𝙚𝙧𝙣𝙖𝙡𝙞𝙯𝙖𝙘𝙞𝙤́𝙣 𝙙𝙚 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙂𝘼𝘽𝘼 (↓ respuesta a benzos 😱)
⬆️ 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙉𝙈𝘿𝘼/𝙜𝙡𝙪𝙩𝙖𝙢𝙖𝙩𝙤 (más excitación ⚡️)
➡️ SE puede causar apoptosis/necrosis, disfunción mitocondrial 🔋⬇️, acidosis, hipoxia, hipotensión… incluso en NCSE 🧠🩸.
🛟 𝘼𝘽𝘾 + 𝟮 “𝙢𝙪𝙨𝙩” 𝙞𝙣𝙢𝙚𝙙𝙞𝙖𝙩𝙤𝙨 ✅✅
Antes (y durante) el fármaco:
🫁 A/B/C: oxígeno, posición lateral, BVM si apnea 😮💨
🩸 𝙂𝙡𝙪𝙘𝙤𝙨𝙖 𝙘𝙖𝙥𝙞𝙡𝙖𝙧 𝙎𝙄𝙀𝙈𝙋𝙍𝙀 🍬📉
🤰 𝙋𝙧𝙪𝙚𝙗𝙖 𝙙𝙚 𝙚𝙢𝙗𝙖𝙧𝙖𝙯𝙤 en mujeres en edad fértil ✅
⚠️ Considera 𝙝𝙞𝙥𝙤𝙣𝙖𝙩𝙧𝙚𝙢𝙞𝙖 𝙨𝙚𝙫𝙚𝙧𝙖 como causa reversible: si Na muy bajo + convulsión → 𝟯% 𝟭𝟬𝟬–𝟭𝟱𝟬 𝙢𝙇 en 10 min (repetible hasta 2 veces) 🧂💉.
💉🥇 𝟭ª 𝙡𝙞́𝙣𝙚𝙖: 𝘽𝙀𝙉𝙕𝙊𝘿𝙄𝘼𝘾𝙀𝙋𝙄𝙉𝘼𝙎 𝙗𝙞𝙚𝙣 𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙙𝙖𝙨 (𝙮 𝙧𝙖́𝙥𝙞𝙙𝙤) ⚡️
El mayor error es 𝙨𝙪𝙗𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙧 😬 (¡pasa mucho!).
Opciones eficaces:
💉 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 𝙄𝙈 𝟬.𝟯–𝟬.𝟱 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
💉 𝙇𝙤𝙧𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟭 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰 𝙢𝙜)
💉 𝘿𝙞𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟮 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
🔁 Si continúa: repetir una vez a los 𝟱 𝙢𝙞𝙣 ⏱️
👉 IM midazolam puede ser superior si no hay IV (se da antes) 🚑⚡️.
💊🥈 𝟮ª 𝙡𝙞́𝙣𝙚𝙖 (𝟮𝟬–𝟰𝟬 𝙢𝙞𝙣): “𝙀𝙎𝙀𝙏𝙏 = 𝙚𝙢𝙥𝙖𝙩𝙚” ⚖️
Si persiste tras benzos → 𝙎𝙀 𝙚𝙨𝙩𝙖𝙗𝙡𝙚𝙘𝙞𝙙𝙤:
✅ 𝙇𝙚𝙫𝙚𝙩𝙞𝙧𝙖𝙘𝙚𝙩𝙖𝙢 𝟲𝟬 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰𝟱𝟬𝟬 𝙢𝙜) 🚀
✅ 𝙑𝙖𝙡𝙥𝙧𝙤𝙖𝙩𝙤 𝟰𝟬 𝙢𝙜/𝙠𝙜 (𝗺𝗮́𝘅 𝟯𝟬𝟬𝟬 𝙢𝙜; +𝟮𝟬 𝙢𝙜/𝙠𝙜 𝙚𝙭𝙩𝙧𝙖 𝙥𝙤𝙨𝙞𝙗𝙡𝙚)
✅ 𝙁𝙤𝙨𝙛𝙚𝙣𝙞𝙩𝙤𝙞́𝙣𝙖 𝟮𝟬 𝙢𝙜𝙋𝙀/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟱𝟬𝟬 𝙢𝙜𝙋𝙀)
📌 ESETT: 𝙨𝙞𝙣 𝙙𝙞𝙛𝙚𝙧𝙚𝙣𝙘𝙞𝙖 𝙘𝙡𝙖𝙧𝙖 entre estos 3 si se usan a dosis correctas.
🧯🥉 𝙍𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤: 𝙖𝙣𝙚𝙨𝙩𝙚𝙨𝙞𝙖 + 𝙞𝙣𝙩𝙪𝙗𝙖𝙘𝙞𝙤́𝙣 + 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 🛌🧠📉
Si sigue tras benzos + 2 ASM → 𝙧𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤 😱
➡️ intubar + infusión anestésica:
🟣 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 bolos + infusión
🟠 𝙋𝙧𝙤𝙥𝙤𝙛𝙤𝙡 bolos + infusión
🟢 𝙆𝙚𝙩𝙖𝙢𝙞𝙣𝙖 (NMDA) = atractiva por farmacorresistencia + mejor perfil hemodinámico 💪🫀
🧠 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 para titular y detectar NCSE ✅.
🫥🧠 𝙉𝘾𝙎𝙀: 𝙡𝙖 𝙘𝙖𝙪𝙨𝙖 𝙤𝙘𝙪𝙡𝙩𝙖 𝙙𝙚𝙡 “𝙘𝙤𝙢𝙖 𝙞𝙣𝙚𝙭𝙥𝙡𝙞𝙘𝙖𝙙𝙤” 👀⚠️
NCSE es común en UCI y puede presentarse como:
😵💫 confusión/agitación | 😶🌫️ estupor/coma | 👁️ movimientos oculares anómalos | 🤖 automatismos
📌 33–46% viene tras convulsivo inicial; y puede progresar a refractario.
✅ Indicaciones prácticas de EEG continuo:
•todo intubado por SE
•no mejora alerta en 10 min o sigue alterado >30 min tras parar convulsión.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más #MedED en #ClubCrit 😄🧠🫶
📚📖 Más en el blog #ClubCrit 👉 [https://t.co/wbCJFKHCXL]
#Neurocritical #NeuroX #NeuroICU #Neurocritical #StatusEpilepticus #Neurology #EEG #POCUS #BNP #HeartFailure #Radiology #Dyspnea #POCUS #LungUltrasound #JVP #ICU #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #Diagnóstico #icu #intensivecare #diagnosis #management #UCI #Tratamiento #MedicinaBasadaEnEvidencia #POCUS #MedEd #Medicina #Emergencias #FOAMed #FOAMcc #MedX #IntensiveCare #EducaciónMédica #MedIntensiva #MedXCommunity #MedicinaCrítica #MedED #CritCare #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HCKorhhXwAE0lM_.jpg)









![MarlonVFZR's tweet photo. 🚨🧠𝗦𝘁𝗮𝘁𝘂𝘀 𝗘𝗽𝗶𝗹𝗲𝗽𝘁𝗶𝗰𝘂𝘀 (𝗦𝗘): “𝘁𝗶𝗺𝗲 𝗶𝘀 𝗯𝗿𝗮𝗶𝗻”⏱️⚡️
@sciencedirect
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
📌SE = crisis prolongada o crisis repetidas 𝙨𝙞𝙣 𝙧𝙚𝙘𝙪𝙥𝙚𝙧𝙖𝙧 𝙡𝙞𝙣𝙚𝙖 𝙙𝙚 𝙗𝙖𝙨𝙚 🧠🌀.
Hoy se considera SE si:
⏱️ ≥𝟱 𝙢𝙞𝙣 convulsivo continuo, o ≥𝟭𝟬 𝙢𝙞𝙣 focal con alteración de conciencia, o 𝟭𝟬–𝟭𝟱 𝙢𝙞𝙣 ausencias.
👉 Después de esos tiempos, la probabilidad de que pare sola es baja 😬 y hay riesgo de lesión neuronal 🔥.
🧠🧬 𝙋𝙤𝙧 𝙦𝙪𝙚́ 𝙪𝙧𝙜𝙚: 𝙛𝙖𝙧𝙢𝙖𝙘𝙤𝙧𝙧𝙚𝙨𝙞𝙨𝙩𝙚𝙣𝙘𝙞𝙖 + 𝙡𝙚𝙨𝙞𝙤́𝙣 𝙣𝙚𝙪𝙧𝙤𝙣𝙖𝙡 🧨
En minutos ocurre:
⬇️ 𝙞𝙣𝙩𝙚𝙧𝙣𝙖𝙡𝙞𝙯𝙖𝙘𝙞𝙤́𝙣 𝙙𝙚 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙂𝘼𝘽𝘼 (↓ respuesta a benzos 😱)
⬆️ 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧𝙚𝙨 𝙉𝙈𝘿𝘼/𝙜𝙡𝙪𝙩𝙖𝙢𝙖𝙩𝙤 (más excitación ⚡️)
➡️ SE puede causar apoptosis/necrosis, disfunción mitocondrial 🔋⬇️, acidosis, hipoxia, hipotensión… incluso en NCSE 🧠🩸.
🛟 𝘼𝘽𝘾 + 𝟮 “𝙢𝙪𝙨𝙩” 𝙞𝙣𝙢𝙚𝙙𝙞𝙖𝙩𝙤𝙨 ✅✅
Antes (y durante) el fármaco:
🫁 A/B/C: oxígeno, posición lateral, BVM si apnea 😮💨
🩸 𝙂𝙡𝙪𝙘𝙤𝙨𝙖 𝙘𝙖𝙥𝙞𝙡𝙖𝙧 𝙎𝙄𝙀𝙈𝙋𝙍𝙀 🍬📉
🤰 𝙋𝙧𝙪𝙚𝙗𝙖 𝙙𝙚 𝙚𝙢𝙗𝙖𝙧𝙖𝙯𝙤 en mujeres en edad fértil ✅
⚠️ Considera 𝙝𝙞𝙥𝙤𝙣𝙖𝙩𝙧𝙚𝙢𝙞𝙖 𝙨𝙚𝙫𝙚𝙧𝙖 como causa reversible: si Na muy bajo + convulsión → 𝟯% 𝟭𝟬𝟬–𝟭𝟱𝟬 𝙢𝙇 en 10 min (repetible hasta 2 veces) 🧂💉.
💉🥇 𝟭ª 𝙡𝙞́𝙣𝙚𝙖: 𝘽𝙀𝙉𝙕𝙊𝘿𝙄𝘼𝘾𝙀𝙋𝙄𝙉𝘼𝙎 𝙗𝙞𝙚𝙣 𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙙𝙖𝙨 (𝙮 𝙧𝙖́𝙥𝙞𝙙𝙤) ⚡️
El mayor error es 𝙨𝙪𝙗𝙙𝙤𝙨𝙞𝙛𝙞𝙘𝙖𝙧 😬 (¡pasa mucho!).
Opciones eficaces:
💉 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 𝙄𝙈 𝟬.𝟯–𝟬.𝟱 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
💉 𝙇𝙤𝙧𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟭 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰 𝙢𝙜)
💉 𝘿𝙞𝙖𝙯𝙚𝙥𝙖𝙢 𝙄𝙑 𝟬.𝟮 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟬 𝙢𝙜)
🔁 Si continúa: repetir una vez a los 𝟱 𝙢𝙞𝙣 ⏱️
👉 IM midazolam puede ser superior si no hay IV (se da antes) 🚑⚡️.
💊🥈 𝟮ª 𝙡𝙞́𝙣𝙚𝙖 (𝟮𝟬–𝟰𝟬 𝙢𝙞𝙣): “𝙀𝙎𝙀𝙏𝙏 = 𝙚𝙢𝙥𝙖𝙩𝙚” ⚖️
Si persiste tras benzos → 𝙎𝙀 𝙚𝙨𝙩𝙖𝙗𝙡𝙚𝙘𝙞𝙙𝙤:
✅ 𝙇𝙚𝙫𝙚𝙩𝙞𝙧𝙖𝙘𝙚𝙩𝙖𝙢 𝟲𝟬 𝙢𝙜/𝙠𝙜 (𝙢𝙖́𝙭 𝟰𝟱𝟬𝟬 𝙢𝙜) 🚀
✅ 𝙑𝙖𝙡𝙥𝙧𝙤𝙖𝙩𝙤 𝟰𝟬 𝙢𝙜/𝙠𝙜 (𝗺𝗮́𝘅 𝟯𝟬𝟬𝟬 𝙢𝙜; +𝟮𝟬 𝙢𝙜/𝙠𝙜 𝙚𝙭𝙩𝙧𝙖 𝙥𝙤𝙨𝙞𝙗𝙡𝙚)
✅ 𝙁𝙤𝙨𝙛𝙚𝙣𝙞𝙩𝙤𝙞́𝙣𝙖 𝟮𝟬 𝙢𝙜𝙋𝙀/𝙠𝙜 (𝙢𝙖́𝙭 𝟭𝟱𝟬𝟬 𝙢𝙜𝙋𝙀)
📌 ESETT: 𝙨𝙞𝙣 𝙙𝙞𝙛𝙚𝙧𝙚𝙣𝙘𝙞𝙖 𝙘𝙡𝙖𝙧𝙖 entre estos 3 si se usan a dosis correctas.
🧯🥉 𝙍𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤: 𝙖𝙣𝙚𝙨𝙩𝙚𝙨𝙞𝙖 + 𝙞𝙣𝙩𝙪𝙗𝙖𝙘𝙞𝙤́𝙣 + 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 🛌🧠📉
Si sigue tras benzos + 2 ASM → 𝙧𝙚𝙛𝙧𝙖𝙘𝙩𝙖𝙧𝙞𝙤 😱
➡️ intubar + infusión anestésica:
🟣 𝙈𝙞𝙙𝙖𝙯𝙤𝙡𝙖𝙢 bolos + infusión
🟠 𝙋𝙧𝙤𝙥𝙤𝙛𝙤𝙡 bolos + infusión
🟢 𝙆𝙚𝙩𝙖𝙢𝙞𝙣𝙖 (NMDA) = atractiva por farmacorresistencia + mejor perfil hemodinámico 💪🫀
🧠 𝙀𝙀𝙂 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 para titular y detectar NCSE ✅.
🫥🧠 𝙉𝘾𝙎𝙀: 𝙡𝙖 𝙘𝙖𝙪𝙨𝙖 𝙤𝙘𝙪𝙡𝙩𝙖 𝙙𝙚𝙡 “𝙘𝙤𝙢𝙖 𝙞𝙣𝙚𝙭𝙥𝙡𝙞𝙘𝙖𝙙𝙤” 👀⚠️
NCSE es común en UCI y puede presentarse como:
😵💫 confusión/agitación | 😶🌫️ estupor/coma | 👁️ movimientos oculares anómalos | 🤖 automatismos
📌 33–46% viene tras convulsivo inicial; y puede progresar a refractario.
✅ Indicaciones prácticas de EEG continuo:
•todo intubado por SE
•no mejora alerta en 10 min o sigue alterado >30 min tras parar convulsión.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más #MedED en #ClubCrit 😄🧠🫶
📚📖 Más en el blog #ClubCrit 👉 [https://t.co/wbCJFKHCXL]
#Neurocritical #NeuroX #NeuroICU #Neurocritical #StatusEpilepticus #Neurology #EEG #POCUS #BNP #HeartFailure #Radiology #Dyspnea #POCUS #LungUltrasound #JVP #ICU #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #Diagnóstico #icu #intensivecare #diagnosis #management #UCI #Tratamiento #MedicinaBasadaEnEvidencia #POCUS #MedEd #Medicina #Emergencias #FOAMed #FOAMcc #MedX #IntensiveCare #EducaciónMédica #MedIntensiva #MedXCommunity #MedicinaCrítica #MedED #CritCare #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HCKosYXWMAALLTi.jpg)
































