Studies find that legacy right ventricular pacing can lead to "pacing induced heart failure." Learn about physiological conduction system pacing #DontDisTheHis
@ArlenWms@epaleezeldin@Terry_M_Wms2 The Toxic Substance Control Act mentioned could apply to qualification of new material in contact with body tissue. Thanks for the heads up!
Tripolar R&LBB lead commercialization negotiations have halted previously posted intentions to disclose "auto-locking LBB connector pin, enhanced tortional stiffness and TV insufficiency avoidance."
You may have seen the LBB-helix performance compared to 3830, posted Jan 23. The first lead designed for BB pacing.
In the coming weeks, see the auto-locking LBB connector pin, enhanced tortional stiffness and TV insufficiency avoidance.
Strategic partnership hinges on speed to market. An attractive, effective lead will inspire and accelerate the life-saving elimination of "pacing-induce cardiomyopathy" of the legacy pacing paradigm.
The LBB transseptal helical blunt dissection electrode is designed (and anecdotally worked) for chronic extraction with no special tools.
It has high impedance for low battery drain (similar to Medtronic CapSure Z) and has half the 6-month pulse width pacing threshold of 3830.
Thanks for asking. Pushing the electrode across the septum is similar to pushing your fork through a tender rare steak, until you hit that tough left ventricular endocardial membrane that is. (A fork with 4 tines takes approximately 4 times the force of one 2-French transseptal lead member. Please refer to our previous post figures.)
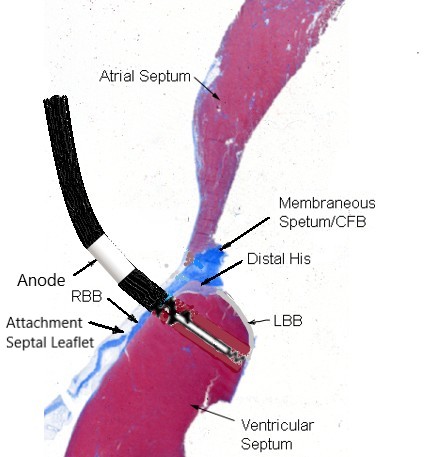
See the tip electrode and tenting of the LV tough endocardial membrane near the LBB. It seems inappropriate to approach the LV endocardial membrane with anything sharp, including the little blunt helical fixation screw. It can allow for tactile plunge electrode position feedback.
Two and a half decades ago, DAVID and MOST suggested conventional pacing that bypasses the cardiac conduction system was unsafe. Visionary EP implanters have boldly introduced a win for paced patients and their loved ones by eliminating pacing induced cardiomyopathy. I believe a company, or companies, will win along with the patients they wish to serve.
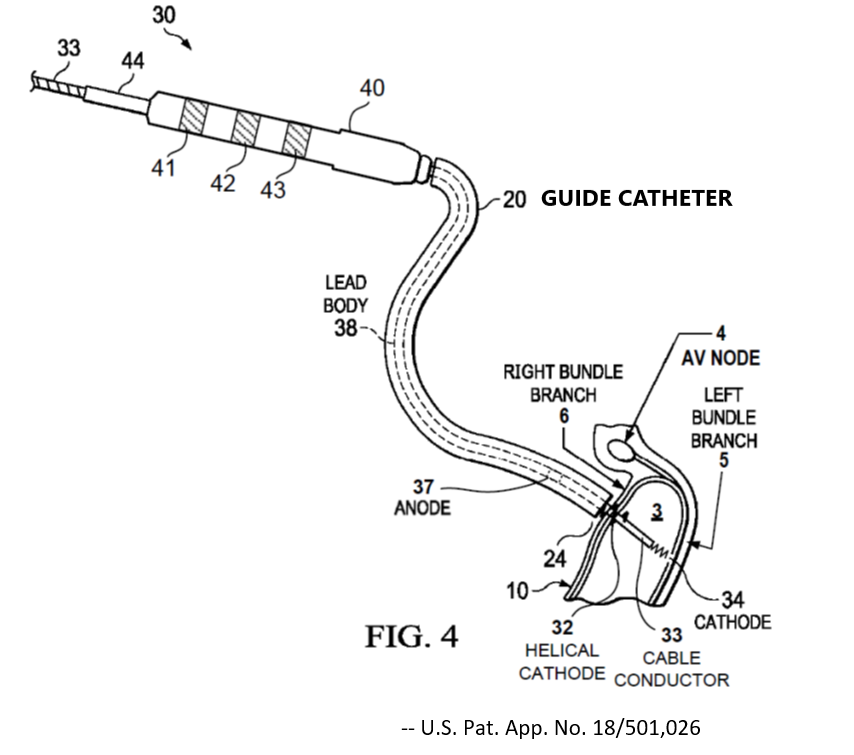
The unipolar, Medtronic Model 10538 (inner assembly of the L&RBB transseptal tripolar lead below) was designed for chronic extractability. Reportedly, limited clinical results found it extractable with no special tools, years after implantation. It replaces the inner assembly of modified Model 3830, below.
Congratulations! After years of mainstream conduction system pacing, a large (23,186 patient) study was published this month. Medicare data aligned with small studies finding all-cause mortality and HFH benefits of CSP.
<Heart Rhythm, Volume 22, Issue 3, p735-743, March, 2025>
Please note that the LBB positive fixation helical tip electrode is blunt. It's inappropriate to approach the LV endocardial membrane with anything sharp. Even with a blunt dissection plunge helical electrode. (Patent pending.)
Terry
Multi-option conduction system pacing lead
1 Anchor the RBB cathode
2 Using the RBB cathode as a fulcrum, retract and advance the guide catheter for LBB mapping trajectory
3 Advance the thin LBB plunge cathode without rotation
4 Rotate the LBB cathode a turn for fixation
The Model 3830 Lead & introduction catheters, and visionary leadership by Dr. Vijayaraman, and others, finding 20% death and HF hospitalization after 5 years of pacing, suggests that many tens of thousands of lives have already been saved. (Based on 2 million pacemakers/year.)
Medtronic's first clinical pass-pull attempt at His bundle pacing with a catheter introduced lumen-less lead to mainstream.
The date: February 18, 1994
The vision: eliminate PICm forever
The business plan: “Do the right thing for the patient and everything else will work out.”