Just a daily reminder that big PBMs suck.
Filled a 90-day prescription for hydrochlorothiazide.
Patient OOP met for the year through their employer-based insurance plan.
We got paid 60 cents.
I don’t care if I were somehow able to obtain those meds for free.
60 cents doesn’t pay the bills.
Never has, never will.
I just wonder what the employer was billed for this drug.
It definitely wasn’t 60 cents, that I know for sure.
@AnthemBCBS
🚨 FLORIDA VS. CVS: State officials subpoenaed the pharmacy giant’s contracts, audits, and rebate records in an investigation into alleged anti-competitive practices driving up prescription drug prices for consumers.
@AGJamesUthmeier: "It appears one company has gotten so big that they are controlling market power in a way that might manipulate pricing at the cost of consumers."
The supposedly most transparent actors in the drug supply chain would pretty please like to make sure that its contract with a public entity not be transparently accessible to the public.
@KenPaxtonTX@TAMU https://t.co/RvIBbfpFAt
⭐️NEW EPISODE⭐️
Express Scripts terminated Martella's Pharmacies. 13 months of fighting back - attorneys, legislators, DC - & still out of network.
Now they're taking it to the people.
🎧Catch It Now!🎧
https://t.co/HN8JncOcv6
@LaurenDC5@MoniqueWhitney #podcast #PBMreform
“Oh, we got rid of PBM spread pricing years ago”
I can’t tell you how many times I’ve heard this phrase, but I can tell you that almost every time, it’s wrong.
Thanks @iastateauditor for working with us to bring transparency & accountability to Medicaid
https://t.co/m83J7YffHt
This bill has overwhelming support from the New York Senate and Assembly as well as the people of New York. The people of New York have spoken and spoken loudly. Too many pharmacies have been forced to close. Governor Kathy Hochul please sign this bill into law sooner than later.
$275 billion.
That's how much taxpayers spend on prescription drugs through Medicare and Medicaid each year, yet we're still unable to fully follow where the money goes once PBMs get involved. Read our latest blog and help us #FollowTheMoney: https://t.co/N9cq8gtWvP
#PBMReform
How about some love for rural pharmacies in Ohio?
I own one.
If the PBMs get their way (they usually do), my store could become yet another casualty in their pricing games.
Ohio has now fewer than 2,000 pharmacies statewide. A number that hasn’t been that low in over a decade.
We’ve lost 200+ stores in just the last couple of years.
It’s a crisis. All we get is “dog and pony show”-esque theater from Washington when it comes to PBMs.
Their abuse needs to end. Today.
Story time:
Had a patient who lives over 30 minutes away transfer their prescriptions to us.
For reference, there are probably 10 other pharmacies between us and the patient.
So why choose us?
Well, it’s simple.
On @AmbetterHealth’s website, it showed our pharmacy as offering the “cheapest” prices on their plan.
Patient was recently retired, but not quite old enough to get Medicare, so they chose this ACA plan through the marketplace. They weren’t too happy with that, but that’s not important for this story.
The driving force for them picking us over Walmart was the 90-day supply price for valsartan 160mg, a common blood pressure medication.
Walmart’s price through his ACA plan was over $170.
Our independent pharmacy price through the same insurance for the same 90-day supply was just $22.39.
How could that be possible?
Your prescription insurance is made to bleed your local pharmacy dry, then leave consumers with the most expensive options.
I will die on that hill until I’m proven otherwise or the system gets blown to pieces.
That is the sole reason as to why I’m such a jaded asshole on this platform towards your insurance company and PBM cohorts.
Oh, and if we do go out of business, the PBMs just blame us for not negotiating better rates.
PBM contracts are non-negotiable! They couldn’t care less if we are profitable.
Tennessee just did what Congress can't.
They passed a law to break up the health insurance giants.
Specifically, they made it illegal for pharmacy benefit managers — the companies in charge of pharmacy insurance — and pharmacies to be owned by the same company.
That makes perfect sense.
For example: CVS Caremark is the PBM, and CVS is the pharmacy. So if you have Aetna insurance, you have CVS Caremark as your PBM, and they're going to do everything they can to make sure you use CVS as your pharmacy. Aetna, Caremark, CVS — all the same company.
That causes all kinds of incredibly obvious problems that this law hopes to fix.
If your insurance company is in charge of approving your medication, deciding how much to pay for it, AND deciding who gets that money — while also being the pharmacy that gets paid at the end — guess what happens to prices?
They go up.
Governor Lee signed the law last week. CVS immediately filed a federal lawsuit because they said it will force them to close all 136 stores they have in Tennessee.
Let that sink in.
I'm not sure most people realize what that says about CVS and health insurance in general. They had to choose between owning the middleman (the PBM) or the healthcare provider (the pharmacy).
Without hesitation, they chose the middleman.
The biggest pharmacy chain in the country — with a store on every corner — would drop all 136 of their Tennessee locations in a second if it means keeping their middleman business.
It is more profitable for them to be a health insurance middleman getting between you and your healthcare than it is to actually provide the healthcare.
That is the problem with healthcare in America.
We have made the middleman so powerful that they've taken complete control of the entire system. Three PBMs — Caremark, Express Scripts, and OptumRx — handle around 80% of all prescriptions in this country.
How on earth can we expect healthcare to work well and remain affordable if that's where the money is?
We all auto-pay our insurance straight out of our paycheck before we even see the money. And not surprisingly, they're keeping a ton of it.
That's why we fired them.
And they can't file a lawsuit to stop us.
That lets us offer fair, transparent prices. No PBMs. No insurance games. No hidden markups. You see the cost, you pay the cost.
This morning, HB 1959 passed the House on a 86-7 vote. This bill prevents PBM ownership of pharmacies. As Senate passed it yesterday, the bill moves to the Governor for signature. We are grateful for the leadership of Rep. Rick Scarbrough! #PBMReform#PatientsOverProfits
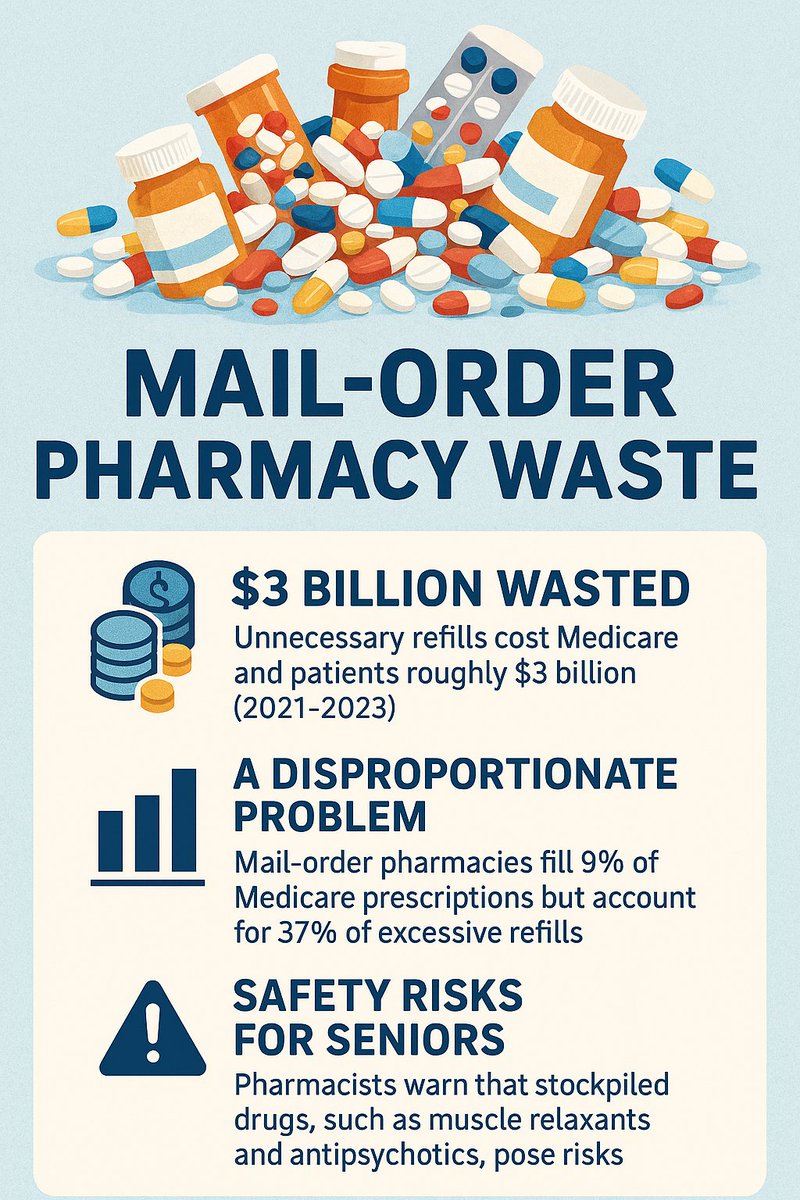
🚨 Mail‑order pharmacy waste is costing billions. A 2025 @WSJ analysis found unnecessary refills cost Medicare & patients ~$3B (2021–23). Though just 9% of scripts, mail‑order drives 37% of excess! 🔗 https://t.co/Gzx1Y22ZNx
#UnmaskTheMiddleman#PatientSafety#HealthcareWaste
Spending Sat morning trying to match prescription # from MTF site to ICN# (don’t know what this stands for) from Beacon site to track down missing payments from a government program that forces us to give 0% loans to drug manufacturers. Why? WTF are we doin here? This doesnt work
BREAKING: Law Firm Announces Filing of Racketeering Class Action Against Express Scripts! this is what happens to the mob! #PBMs#PBMob
https://t.co/Q4KyoIfq9Q
The daily life of an independent pharmacy in America.
Revenue of $13,000 + in one day filling 153 prescriptions.
Not bad.
Until you adjust for the Medicare Drug Negotiated Rebates you have to wait 4-6 weeks for payment.
That leaves the adjusted gross profit for the day at NEGATIVE $795.
Unsustainable.
The claims highlighted in yellow are the Medicare Negotiated Drugs.
Pharmacies are not financial lenders, yet @CMSGov deemed it appropriate to let them float the money to make the program work.