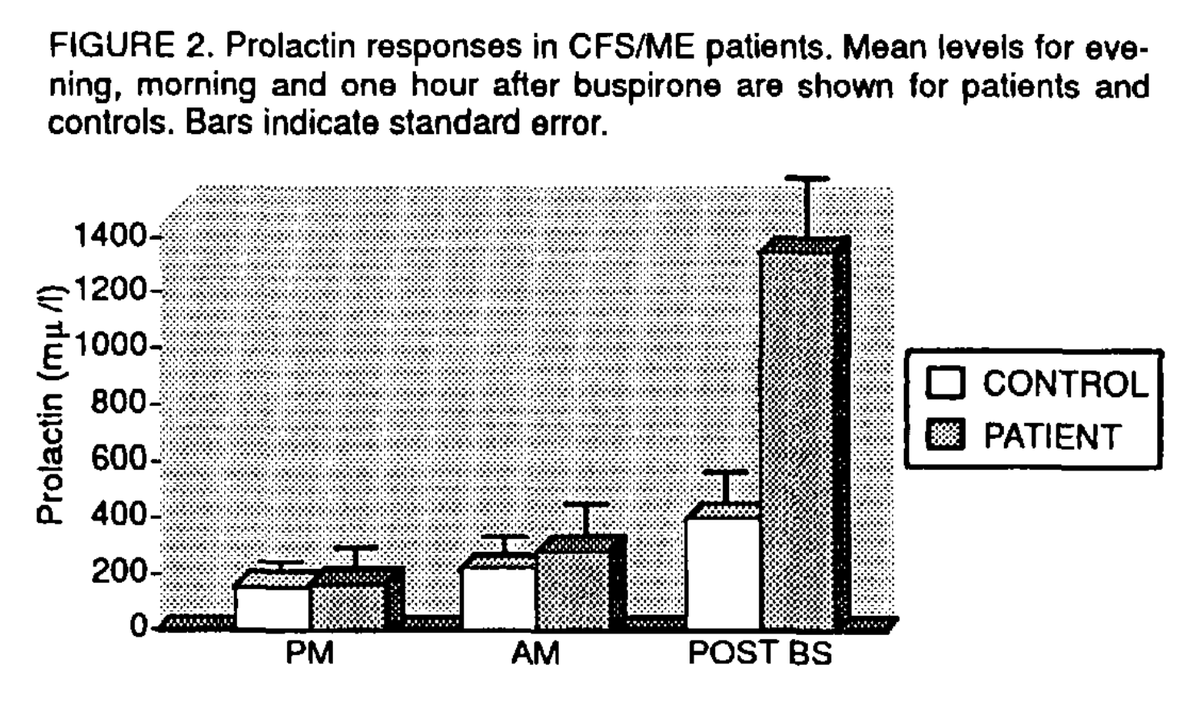
1) With genetic evidence pointing to the brain, there is renewed interest on the S4ME forum for the buspirone tests done in the 1990s.
A couple of small studies found an increased prolactin response in ME/CFS patients but these findings were never studied further.
They perform the idea of helping us. They don’t actually do it.
They could have bought America’s largest mobile phlebotomy company outright. Instead they’ll schedule another meeting to plan a plan.
Since I got Long COVID, the government cycle has been:
Admit not enough is being done → plan a meeting → meet → say a plan is needed → make half a plan → do none of it or do it bad → repeat.
Just do something already, we don’t want another letter.
The world's first genomic study into ME, or Myalgic Encephalomyelitis, has been announced.
Researchers are hoping that by building a genetic map of the illness, it will help pave the way for a future diagnostic test and even treatments.
But charities have warned that there is more to do and this must only be the start.
Another uncomfortable client call looms where I have to inform them that they need to secure a £60k per annum pay rise before October in order to absorb the upcoming increase in their mortgage rate
@HalfThePerson@hoc9718@C_Scheibenbogen@ImmunoFever@mitodicure We're similar, but I can't run for more than 10s...
If I overdo exercise (rowing/reclined) I clunk into tired but wired, sleep poorly, then get destroyed by flu-like symptoms plus migraine the next day–it usually starts early afternoon.
Is this PEM/PESE, or not, in your model?
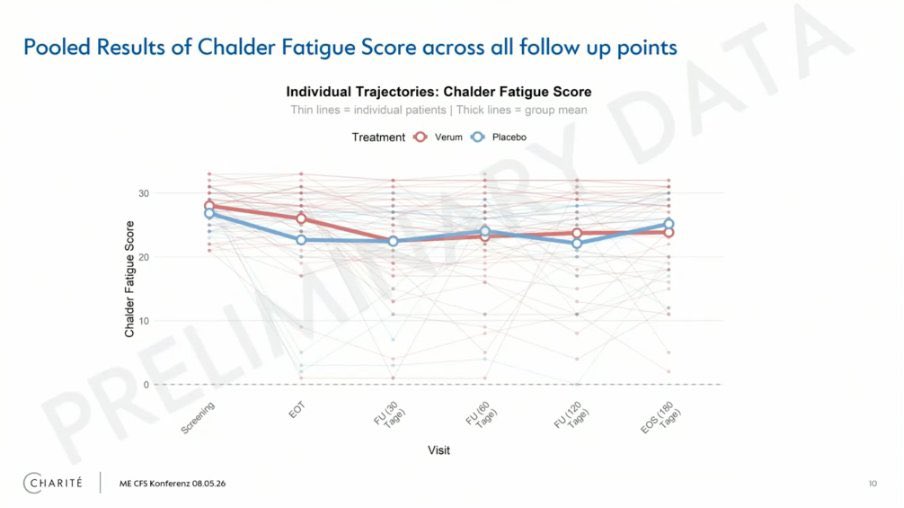
This trial is not a fail. Look at the individual trajectories: a subgroup had substantial gains while pooled means hide it.
We need to stop blindly trialling everyone and use exploratory biomarker analysis to find who responds.
Precision medicine is the way out of LC & ME/CFS.
Very interesing connection - fits with #MECFS patient reports that they are better off if they drink a good amount of water while still in bed in the a.m.:
https://t.co/UyRoSEp0NM
(and fits with similar current POTS recommendations as well😀)
We’ve noticed this too. Many patients say they have PEM, but deeper questioning reveals different phenomena entirely. 10+ different presentations all saying worse after exertion, but with completely different internal meaning.
A single question will just lump them together.
@ABrokenBattery I think VZV is massively underlooked... There's a lot more to it than chickenpox and shingles. Enteric shingles, for example, or VZV in the CNS–it's known to cause autonomic failure, so peripheral autonomic neuropathies are a reasonable assumption too.
This is an incredible $10M donation to our PolyBio Long COVID Cure Initiative (LCCI) Program. Funds are from the Park-Pagliuca Fund: a philanthropic collaboration between the families of Todd Park & Steve Pagliuca, each of whom have family members impacted by Long COVID
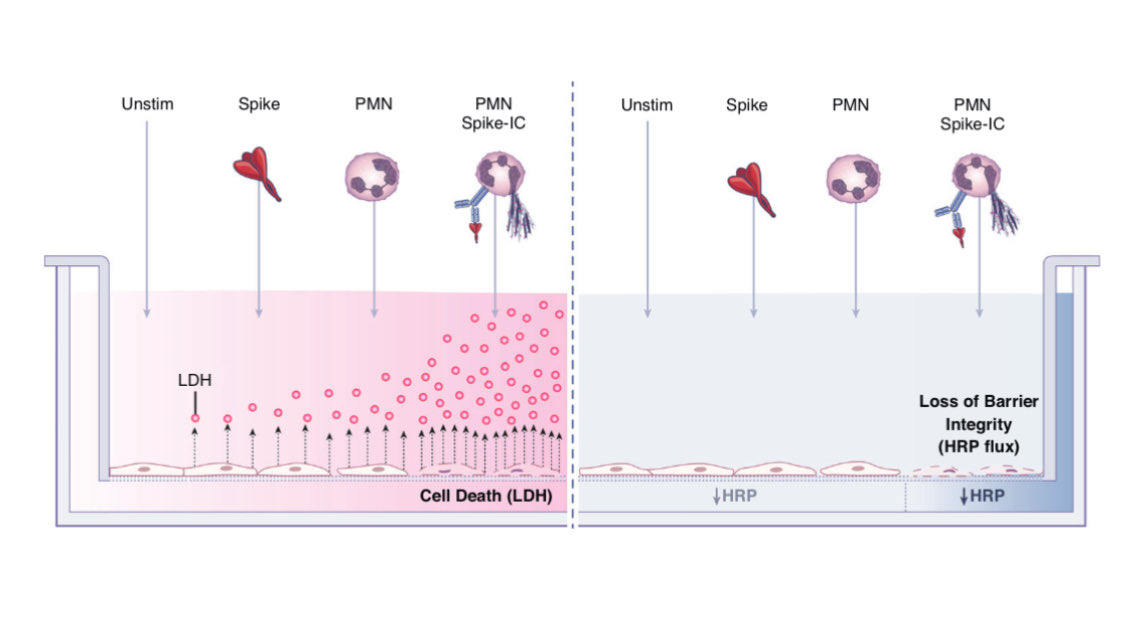
Breaking: New PolyBio-supported Study Identifies Microclots, Endothelial Injury Markers and Neutrophil Activation in Children and Young Adults with Long COVID
A new study supported by PolyBio Research Foundation studied children and young adults with Long COVID, providing evidence linking endovascular inflammation, increased quantity and size of fibrin-amyloid “microclots,” and neutrophil activation, and finding detectable Spike protein in a subset.
https://t.co/hOR1mWHRdc
I respectfully disagree. As a general pediatrician caring for a large neurodiverse population (ASD, ADHD, dyslexia, CAPD, concussion, anxiety), I’m seeing a very different reality over the last 5 years. 🧵1/14
Xolair (Omalizumab) literally resolved all my downstream psychiatric symptoms related to MCAS=>hyperadrenergic dysautonomia episodes - agitation, irritability, aggressiveness, intense feeling of doom etc
It’s body=>mind most of the time
I developed a POTS-like condition that turned me into a semi-invalid for five years. Every doctor I saw diagnosed some version of stress/anxiety/panic disorder—except, ironically, the psychiatrist I consulted. None of them realizes they got it wrong. I think about that a lot.
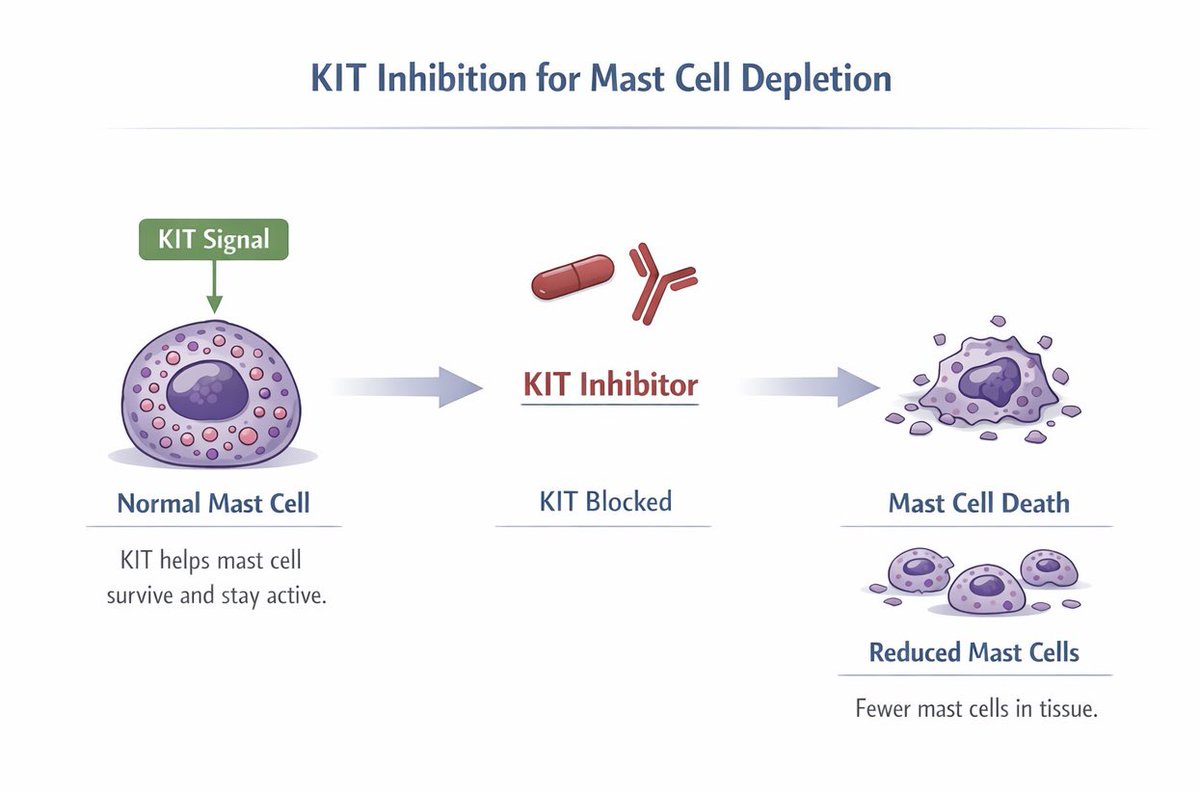
The strongest new mast cell-targeting drugs are in CSU, and the best of them may represent potential remission-level treatments for central mast cell diseases by directly reducing the pathological cell rather than just blocking one pathway.