“🚨 Podcast 🚨”
Dive deep into the world of neuro-oncology with ‘Neuro-oncology Talks | The Deep Dive.’ Explore groundbreaking research, AI in medicine, and the future of brain tumor treatment. 🎙️
Listen now: https://t.co/dQsgTQTKEh
#NeuroOncology#CancerResearch#AIInMedicine
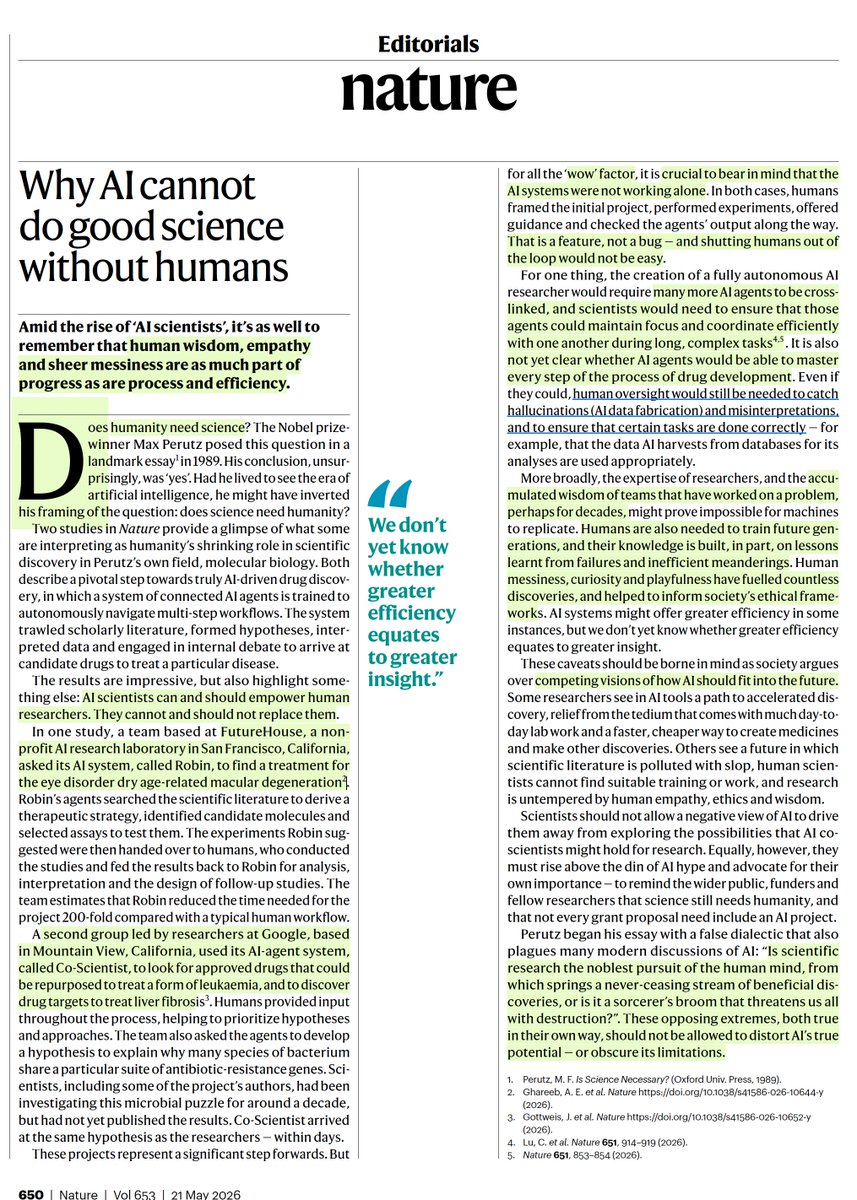
Important editorial @Nature on the new "AI-scientist" papers
"AI scientists can and should empower human
researchers. They cannot and should not replace them."
https://t.co/CZQUrMV8D1
To call it or not to call it? That is the question!
Do you feel a bit wacky & wobbly when it comes to calling normal pressure hydrocephalus on imaging?
You don’t want to overcall it, but you don’t want to miss it either!
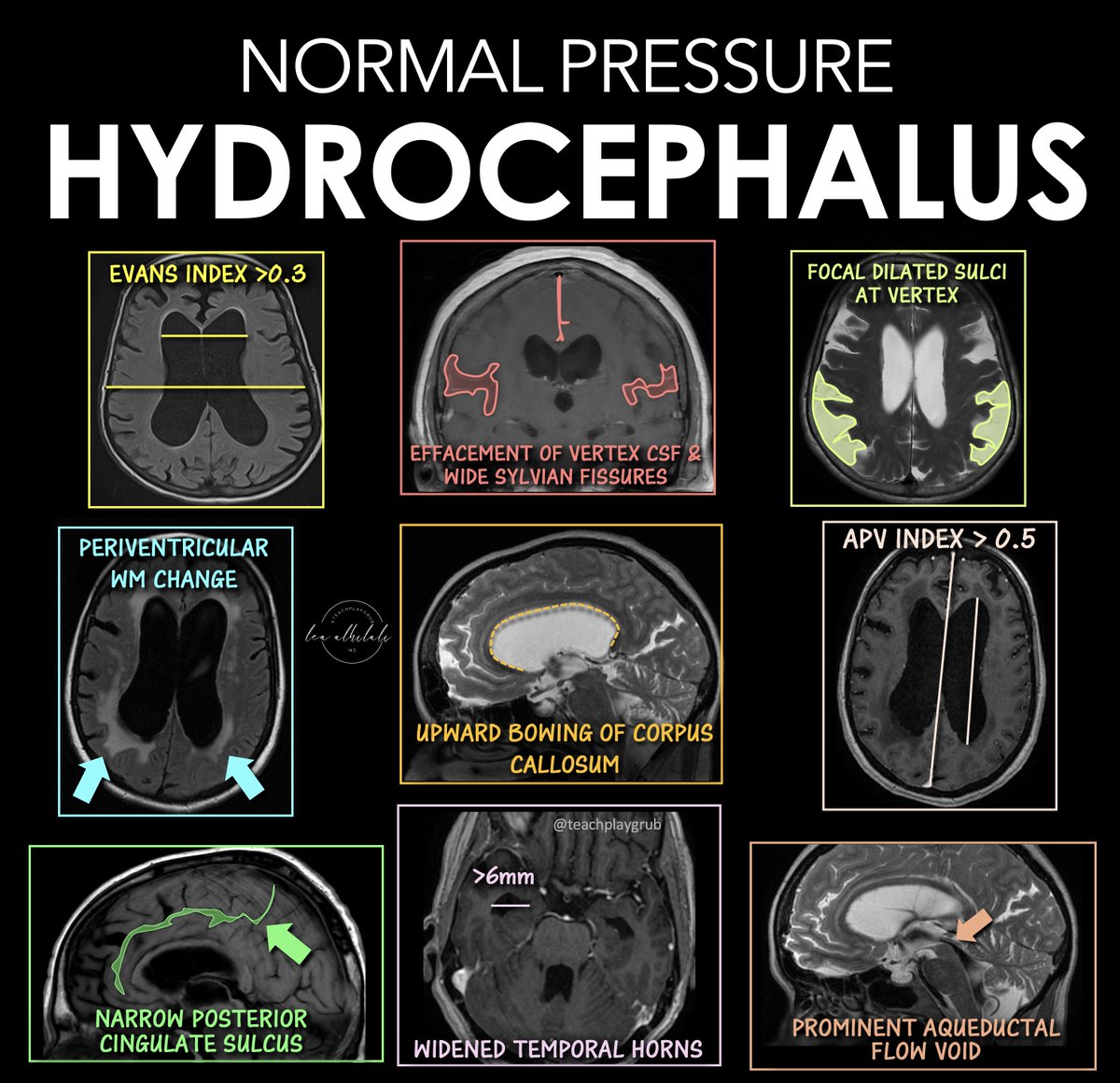
Here are the signs of NPH
🔹 Evans Index > 0.3
--Enlarged frontal horns relative to skull width → ventriculomegaly.
Remember it: “One out of three is too big for me!”
🔹 Periventricular White Matter Change
--T2/FLAIR hyperintensity from transependymal CSF flow.
Remember it: “Leaking pressure leaves a glow.”
🔹 Narrowing of the Posterior Cingulate Sulcus
--Tight high-convexity sulci from crowding at the vertex.
Remember it: “The top gets squeezed shut.”
🔹 Effaced Vertex CSF + Wide Sylvian Fissures
--Tight sulci up top but enlarged fissures laterally (DESH pattern).
Remember it: “Dry on top, wet on the sides.”
🔹 Upward Bowing of the Corpus Callosum
--Ventricular expansion pushes the corpus callosum upward.
Remember it: “If the corpus callosum is arched, the patient can’t march (wobbly)”
🔹 Temporal Horns > 6 mm
--Early temporal horn dilation from hydrocephalus.
Remember it: “Big horns before big vents.”
🔹 Focally Dilated Sulci at the Vertex
--Patchy enlarged sulci despite surrounding crowding.
Remember it: “Holes in a leaky roof = too much water on the brain!”
🔹 APV Index > 0.5
--Increased ventricular-to-parenchymal proportion suggesting hydrocephalus.
Remember it: “Glass half full is too much!”
🔹 Prominent Aqueductal Flow Void
--Increased CSF flow through the aqueduct on MRI.
Remember it: “If the aqueductal flow is super black, the ventricles are out of whack.”
Classic NPH imaging theme: enlarged ventricles + tight high convexities + disproportionate CSF redistribution.
Hopefully now you won't wobble on the diagnosis of NPH!!
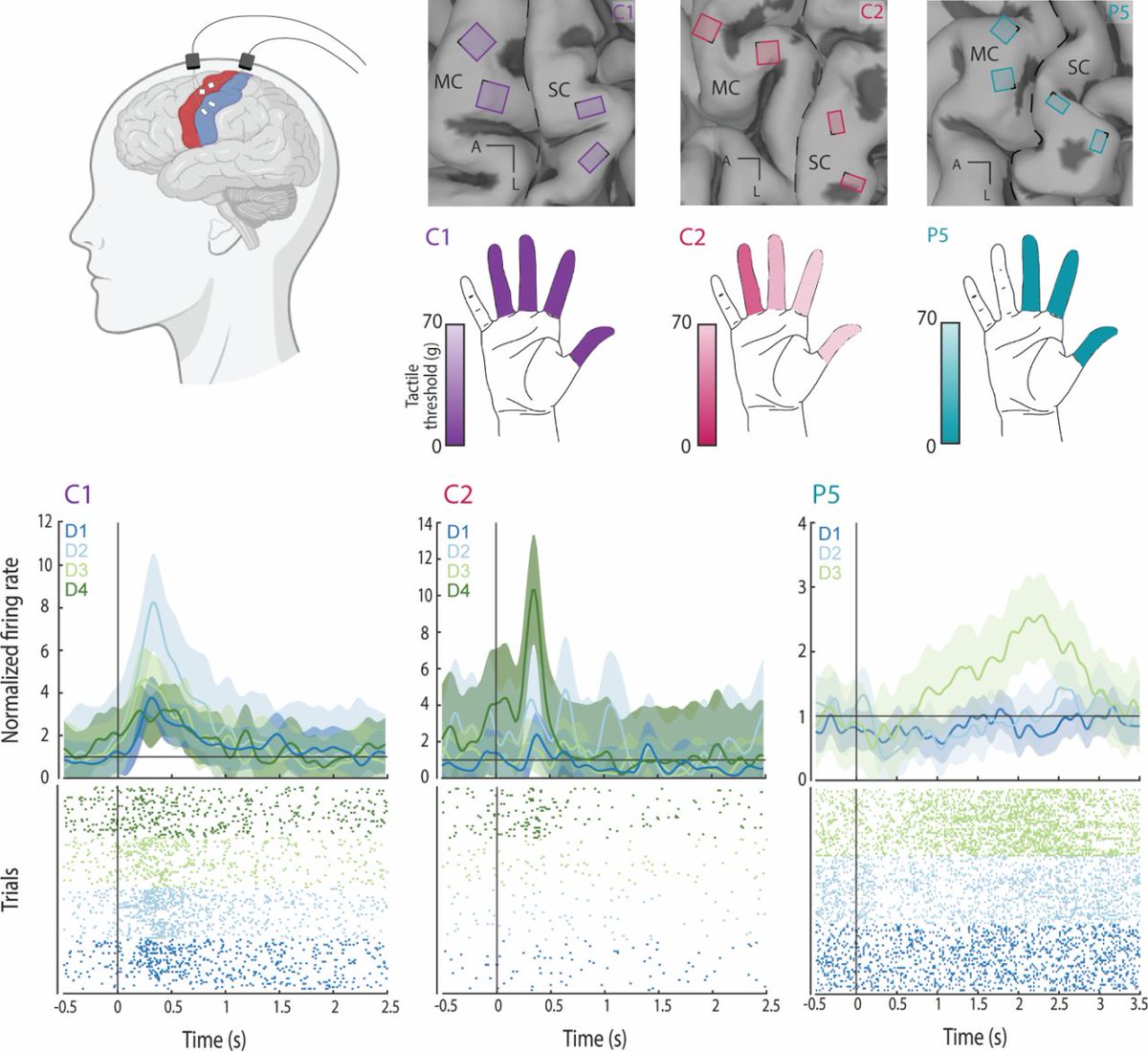
NEW PREPRINT OUT!
Happy to share that our #preprint on how the human #brain encodes #touch: https://t.co/ntS6Ytjhjb
We investigate how touch is encoded in the human #somatosensory and #motor cortices recorded via #microelectrode arrays across different tactile conditions
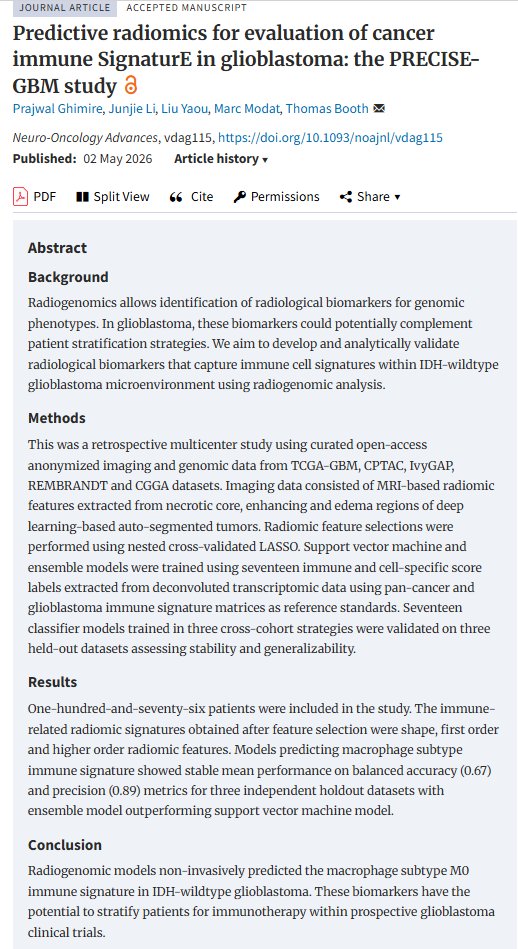
Predictive Radiomics for Evaluation of Cancer Immune SignaturE in Glioblastoma: the PRECISE-GBM study
Prajwal Ghimire, Junjie Li, Liu Yaou, Marc Modat, Thomas Booth
https://t.co/S07cxRYWlX [𝚌𝚜.𝙻𝙶]
New Research Alert! 🧠💻
1/3
Can AI map the #glioblastoma immune environment without a biopsy? Our new PRECISE-GBM study in @EditorNeuro says YES.
We’ve developed a radiogenomic pipeline to non-invasively predict macrophage M0 signatures using standard pre-operative MRI:
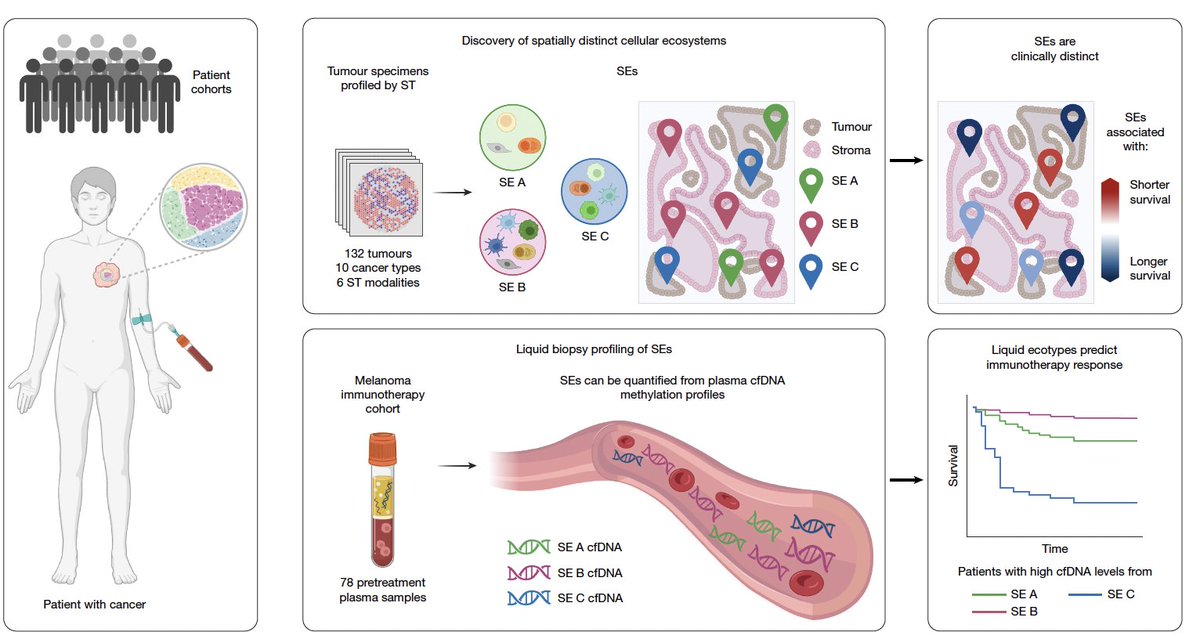
We've known how important the tumor microenvironment is for cancer progression and treatment, but we never had a non-invasive blood test to assess it. Today, as reported @nature, one has been discovered https://t.co/rDaF5YUwTq
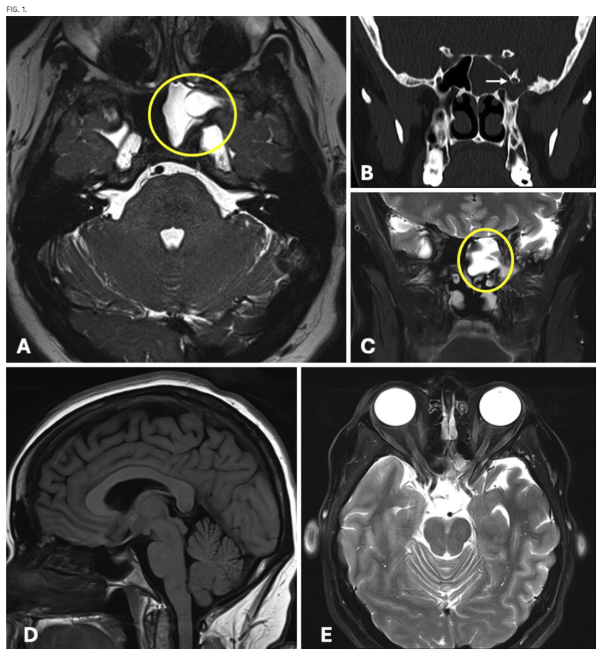
#JNSCaseLessons. Researchers highlight variant case of spontaneous CSF rhinorrhea arising from combined Sternberg canal defect and intracranial hypertension.
https://t.co/702Ph3lSMW
Building strong medical AI means large datasets.
But in healthcare, data is hard to get. A new study shows you may not need it. By focusing training on key clinical concepts, a vision-language model achieved state-of-the-art performance using just 1% of the typical data while preserving its reasoning ability.
What do we think of this shift? Does progress in medical AI come less from more data and more from teaching models what actually matters?
https://t.co/R0L126zwwN
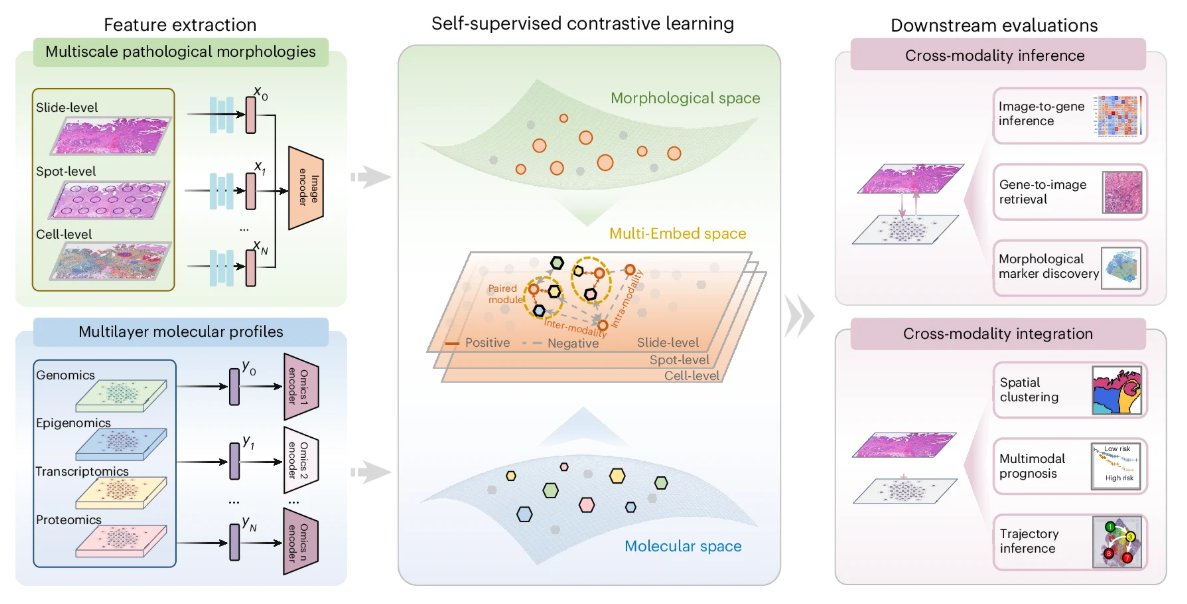
Multi-Embed is an interpretable framework that enables integrated analyses of histological images and multilayer molecular profiles.
https://t.co/MMn2ClZi1l
1/Do radiologists sound like they are speaking a different language when they talk about MRI?
T1 shortening what? T2 prolongation who?
Here’s a translation w/an introductory thread to MRI.
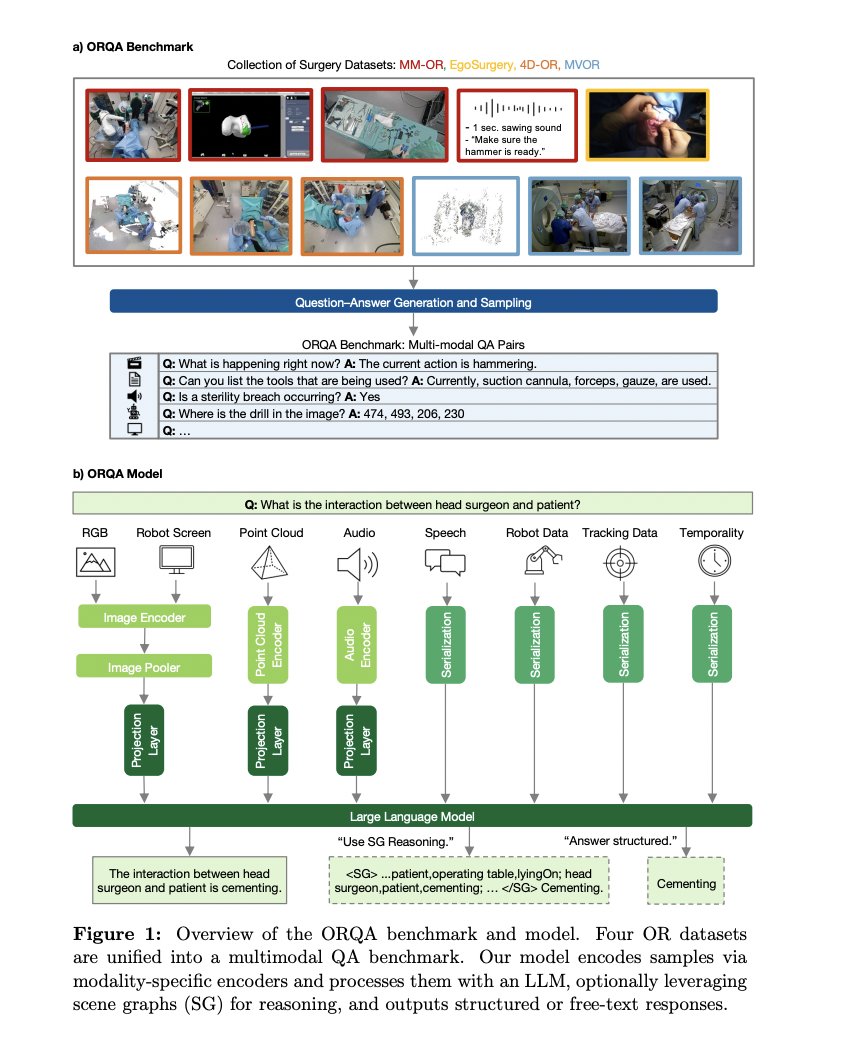
The operating room is one of the hardest environments for AI: constant motion, multiple devices, and high stakes. There is really zero room for error. But general-purpose models are not built for that reality.
A new study introduced ORQA, a specialized multimodal foundation model that understands surgical scenes using video, audio, and structured data. It significantly outperformed generalist AI systems and was designed in multiple sizes for real-world deployment.
How do we continue building systems specifically trained for the complexity of care?
https://t.co/9mcXaYRRVW
Can't remember the types of craniotomies off the top of your head?
Do you need another thing to memorize like you need a hole in your head?
Here's a quick figure with a review of some common craniotomies to help you out!
Let’s dig deeper into these holes!
Frontal: For large midline anterior and sometimes middle skull base lesions
Temporal: For middle cranial fossa lesions, including intra-axial lesions in the mesial temporal lobe
Parietal: For mid to posterior cerebral hemisphere lesions while sparing the motor and sensory cortices.
Parietal interhemispheric approach for parafalcine, medial parietal, and splenial lesions. Parietal transcortical route for intra-axial lesions through the functionally “silent” superior parietal lobule
Pterional (frontotemporal): Access to the frontal lobe, temporal lobe, and Sylvian fissure and allow for direct visualization of the microvasculature surrounding lesions in the suprasellar cistern
Mapping nerves in a whole embryos.
We find that across species and development stages, embryonic nerves display (beautiful) fractal geometry.
More here: https://t.co/LqZrO7Wnfp


























![Memoirs's tweet photo. Predictive Radiomics for Evaluation of Cancer Immune SignaturE in Glioblastoma: the PRECISE-GBM study
Prajwal Ghimire, Junjie Li, Liu Yaou, Marc Modat, Thomas Booth
https://t.co/S07cxRYWlX [𝚌𝚜.𝙻𝙶] https://t.co/KImYvICgs9](https://pbs.twimg.com/media/HIN-gE2XQAA4lwC.png)