Do you have details? Was it doubling time related or absolute or uptake related? In general data says 95%+ concordance - do you think it is significantly different here due to these other factors? I think we need to be moving that way - would just be surprised, for this trial, at this timeline, moving the primary was able to capture what we have learned in the past 24 months or so. Thanks in advance.
@seanmmcbride Yes. Normally it isn't a bad thing to look at but here - 100% up front vs likely the same thing later, carries much less value. Plus as we iterate faster, there is a larger and larger benefit to delay. The available drug might be 3x better than current ones.
@DrSpratticus@ChapinMD Well done on the thread. I'm afraid 99% of people will only see this👇 When, if it were me, I'd avoid intensification almost across the board. Hopefully biomarker / predictive items continue to show ability to parse this cohort.
Consider this. If they believe this, insurance should be paying for our MOC. They could make more in that model. Of course they don't believe this. Other option is drive down radiation billing so in budget neutrality they can get more for radiology. But most likely just conflated data that lets a board member promote "benefit" - saying see, you must keep paying - it benefits the system.
@SprakerMDPhD I don't doubt that younger people use less fractions. And even isolated 65 yr olds using more fractions than 65 yr olds working in environments with younger people, but to think that is MOC causality is laughable "science". And the link to dollars is not that simple. Just poor
ABR board member says there is value in MOC. Article paywalled but no mention of site of service and likely proton codes not eval'd. Just a partial look at one variable in a complex system and then conflating data.
We see this exact error all the time.
https://t.co/K9i8MNuROr
$39 dollars for IMRT in CA. New Jersey at $21. These are real Medicaid rates post the CMS restructuring. Goal: 1) Raise awareness, 2) Actionable letter.
Rome burns.
@savadMG Medicare is federally run. Medicaid programs are state run and states got to "reset" payments when the federal program "restructured" radiation payments.
14 facility closures year to date. More than 20 considering closer by end of summer.
Industry has sold the US equipment and sees our market shrinking so their interest is elsewhere in the globe.
If you lead a large program - your voice is critical to these financial issues.
AI says RayStation python scripting can handle this essentially in one click via the route you are discussing. Burning dose into the pixels so the "dumb" PACS end can display. We're busy and don't control the PACS but have a few doing projects - I'll see... What AI says vs. reality isn't always right, but it followed right along with your thread easily. 10 min of steps into a repeatable script. Again, give me a bit.
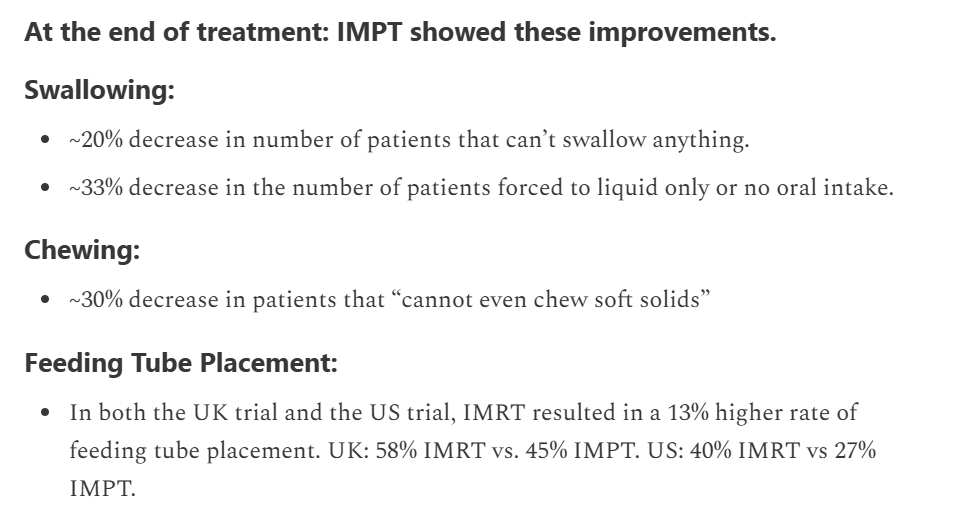
@Nat83052921@HardenedBeam Maybe but 640 randomized pts point to far less tube requirements. It would be quite ironic for this to be bias in favor of protons.
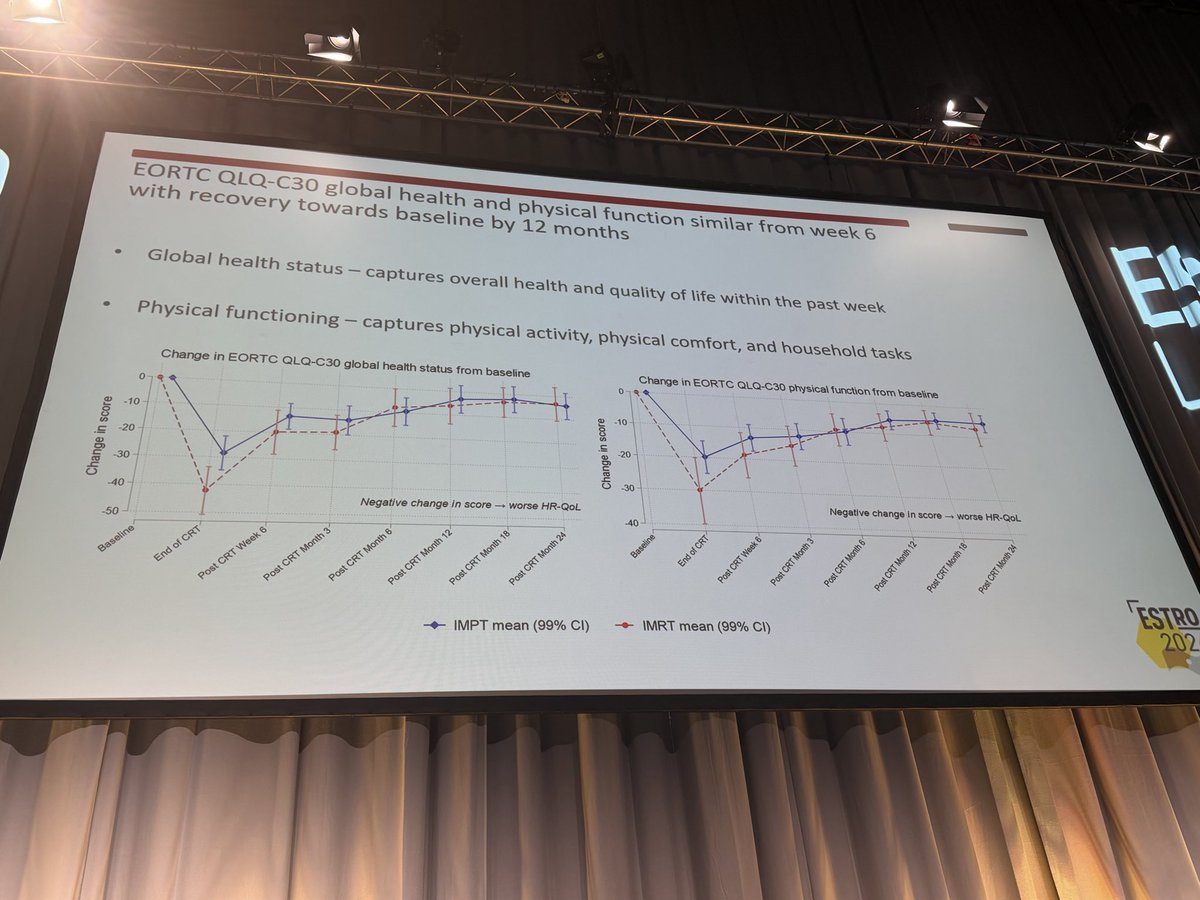
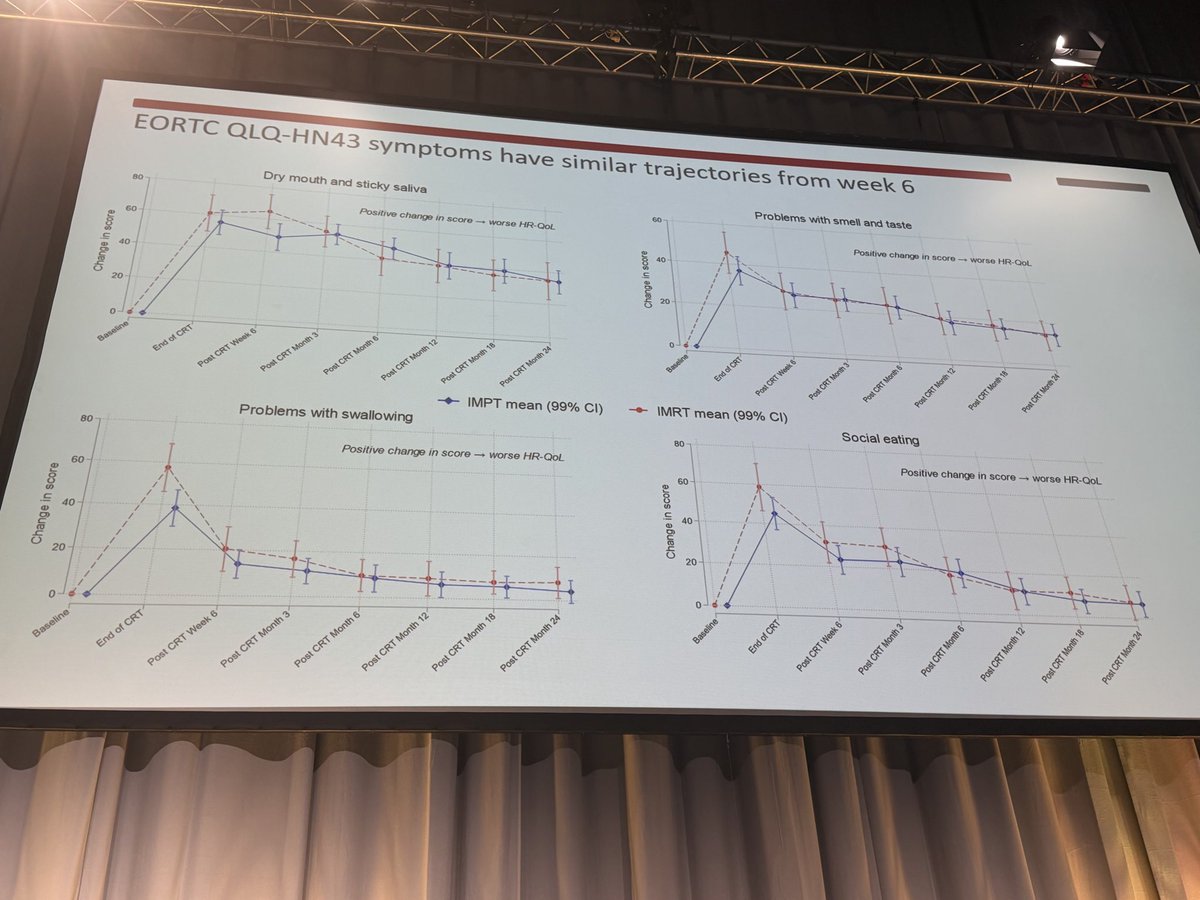
This isn't quite right though. There were improvements even in the negative TORPEDO trial - just temporary. This is kind of the opposite take to leaning into an OS survival.
"No QoL". From a patient perspective, I'd think they 100% think these are improvements.
No QoL difference with IMPT vs IMRT in oropharyngeal cancer in the TORPEdO 🇬🇧 trial.
How to explain the differences w/ @SJFrankMD 🇺🇸 trial? Planning? Patients? Crossover in the 🇺🇸 trial? Real absence of difference?
Cc @EmmaHall71 @