1/ Imagine if a simple blood sample could tell doctors which parts of your body are aging faster than expected.
Not your age on a calendar.
Not a single “biological age” score.
But whether specific cell types—such as brain-supporting cells, muscle cells, immune cells, or lung cells—appear older or younger than they should.
That is the idea behind a remarkable new Nature Medicine study involving more than 60,000 people.
Researchers analyzed thousands of proteins circulating in blood and used them to estimate the biological age of hundreds of different cell populations throughout the body.
The most important finding wasn’t that we age.
It was that we don’t all age in the same way.
One person might have relatively youthful muscle cells but older immune cells.
Another might show signs of accelerated aging in lung-related cells while everything else appears normal.
The future of medicine may be less about asking “How old are you?” and more about asking “Which parts of you are aging fastest?”
3/ The next decade may be defined not by a single breakthrough, but by the convergence of multiple immunotherapy technologies.
CAR-T therapy has demonstrated that genetically engineered immune cells can produce remarkable responses in some blood cancers.
CAR-NK therapies aim to make cellular immunotherapy faster, safer, and potentially available “off the shelf.”
Engineered macrophage and monocyte therapies seek to solve one of oncology’s greatest challenges: solid tumors.
Cancer vaccines are becoming increasingly personalized through genomic sequencing.
Artificial intelligence is accelerating the discovery of tumor-specific targets.
Advanced manufacturing technologies are reducing production times that once required months.
Yet major challenges remain.
Many tumors still resist immune attack.
Responses can be temporary.
Costs remain extraordinarily high.
And some therapies can trigger severe immune toxicities.
The story of immunotherapy is therefore not one of victory.
It is the story of a rapidly evolving scientific field attempting to transform the immune system itself into a programmable therapeutic platform.
The implications extend far beyond cancer.
1/ Immunotherapy: Reprogramming the Immune System to Fight Cancer
For most of medical history, cancer treatment was surprisingly straightforward: cut it out, poison it, or irradiate it.
Surgery, chemotherapy, and radiation remain essential tools. They have saved millions of lives. But they all share a common limitation: they attack the tumor directly.
Immunotherapy approaches cancer from a radically different angle.
Instead of asking, “How do we kill this cancer?” immunotherapy asks, “Why isn’t the immune system killing it already?”
The human immune system evolved over hundreds of millions of years to identify and destroy abnormal cells. Every day, immune cells patrol our bodies, recognizing infected, damaged, and potentially cancerous cells before they become dangerous.
Cancer succeeds because it learns how to hide, suppress, or manipulate those defenses.
Modern immunotherapy attempts to remove those disguises, reactivate exhausted immune cells, or engineer entirely new immune responses.
The result has been one of the most important shifts in oncology in decades: treatments that don’t attack the tumor directly—but instead transform the patient into the therapy.
Not all cancers respond. Not all patients benefit. But the concept has fundamentally changed how scientists think about cancer treatment.
🔴 Democratic TILs?
OBX-115 TIL in advanced #melanoma (Agni-01 #ASCO26) by @DrBetofMDPhD
ORR 67% | DCR 93% | mDoR not reached | n=15
☢️mbIL15 engineered TILs replace high-dose IL-2. Low-dose LD. CNB-enabled manufacturing.
🔍Small cohort, short follow-up. If it holds in Ph2, it dismantles the main toxicity barrier of TIL therapy.
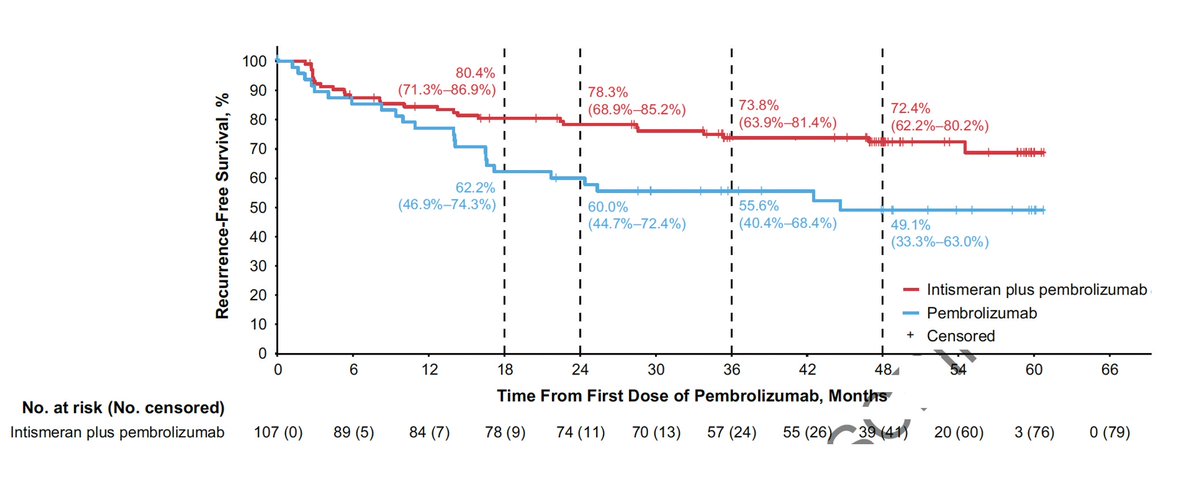
Post-PD-1: RP1+nivo (IGNYTE, anti-PD-1-failed) ORR 33.6%, 3-yr OS 47.8%, durable, ph III pending @MKWongMDPhD
Cell therapy: the contest is IL-2-free TIL (OBX-115, GC-101) vs PRAME TCR-T (anzu-cel). @DrBetofMDPhD@diwakardavar Lu Si. Details in another post
$IOVA - I have been saving this clip for today’s news that Australia has approved Amtagvi for second line metastatic melanoma. An Ausie experienced the life saving power of Amtagvi first hand. The Australian melanoma community has been waiting for a long time. Today their dream came true. Massive melanoma market in Australia; that has the highest melanoma rate globally.
https://t.co/7EskxgbPRr
Happening live at #ASCO26, Lilit Karapetyan, MD (@KarapetLilit), presents research exploring immune features within melanoma tumors and their potential role in durable responses to tumor-infiltrating lymphocyte (TIL) therapy. #MoffittASCO26
Another major advance vs cancer! @ASCO#ASCO26
Personalized neoantigen mRNA vaccine 5 year follow-up vs metastatic melanoma reduced recurrence and death by 49% (on top of Keytruda)
https://t.co/NadITTYIT2
$IOVA #ASCO26#Melanoma
Went through the ASCO26 melanoma abstracts. A few notable updates:
OBX-115: next-gen TIL from Obsidian Tx
https://t.co/dmcZf71A7q
1. ACZ dosing can continue up to 24 weeks post-TIL infusion.
2. Cell dose range is 1–100 × 10^9 cells, broadly similar to Amtagvi.
3. OBX-115 reported 67% ORR (10/15) in patients with ≤2 prior lines of therapy. Amtagvi reported 52% ORR (12/23) in patients with ≤2 prior lines. Given the small numbers, I don’t think OBX-115 has shown a materially higher ORR yet.
4. Durability remains the key question. Less intense lymphodepletion and no IL-2 are both factors that could potentially reduce durability. OBX-115 removes high-dose IL-2 and uses lower-dose LD, so durability is the real test.
5. Both core needle biopsy (CNB) and surgical excision were allowed for tumor harvest/manufacturing, but only 13% of products were manufactured from CNB. The vast majority still required surgical excision.
6. LD is low dose, but only 27% of patients received LD in the outpatient setting. Most still received inpatient LD (require hospitalization).
7. Fifteen patients were successfully manufactured and infused at the RP2D, but the manufacturing success rate was not disclosed. That is an important missing detail. An obvious number to report but omitted usually means bad data.
8. Safety does look improved so far, with no treatment-related mortality. That said, the sample size remains small. Rare grade 5 events at low-single-digit incidence may not appear until much larger cohorts are treated.
9. Overall, OBX-115 so far looks consistent with what I would expect from an Amtagvi-like TIL product using lower-dose LD and no IL-2: potentially better tolerability, but durability remains unproven.
IMA203: $IMTX
https://t.co/pu9wjZUgpA
The update looks underwhelming compared with what was already disclosed at ASCO25 and in the corporate deck. I’m a bit surprised this received an oral presentation. In my view, this felt more like a publication-only abstract.
RP1 + nivolumab: $REPL
https://t.co/sLYXdksXUl
The 3-year landmark OS rate of 45.5% looks numerically impressive versus Amtagvi’s ~30%. But this likely reflects a much easier-to-treat population: more superficial/shallow injectable lesions, less heavily pretreated patients, and other selection factors. Without a proper control arm, the comparison is hard to interpret.
PRAME TCR-T bispecifics: $IMTX
https://t.co/Hwy0Vk9rMM
Underwhelming melanoma activity, with ORR ≤20% even in combination with anti-PD-1.
GC101 TIL: late-breaking abstract
https://t.co/Hwy0Vk9rMM
Data drop on June 1. Since this is a late-breaking abstract, there may be something interesting here.
NICE-TIL: NKG2D-CAR + mbIL15 + TIL
https://t.co/DrMELPdlyr
This combines cytokine engineering and CAR-T engineering into a TIL product. The first treated patient achieved a PR. Still very early, but conceptually interesting.
Finally, ASCO has a full Clinical Science Symposium focused on cell therapy in melanoma:
“Accelerating Adoptive Cell Therapy in Melanoma: Are We Sold on Cells?”
https://t.co/eej69PW8Tx
To me, that is a clear signal that the field is paying increasing attention to adoptive cell therapy in melanoma.
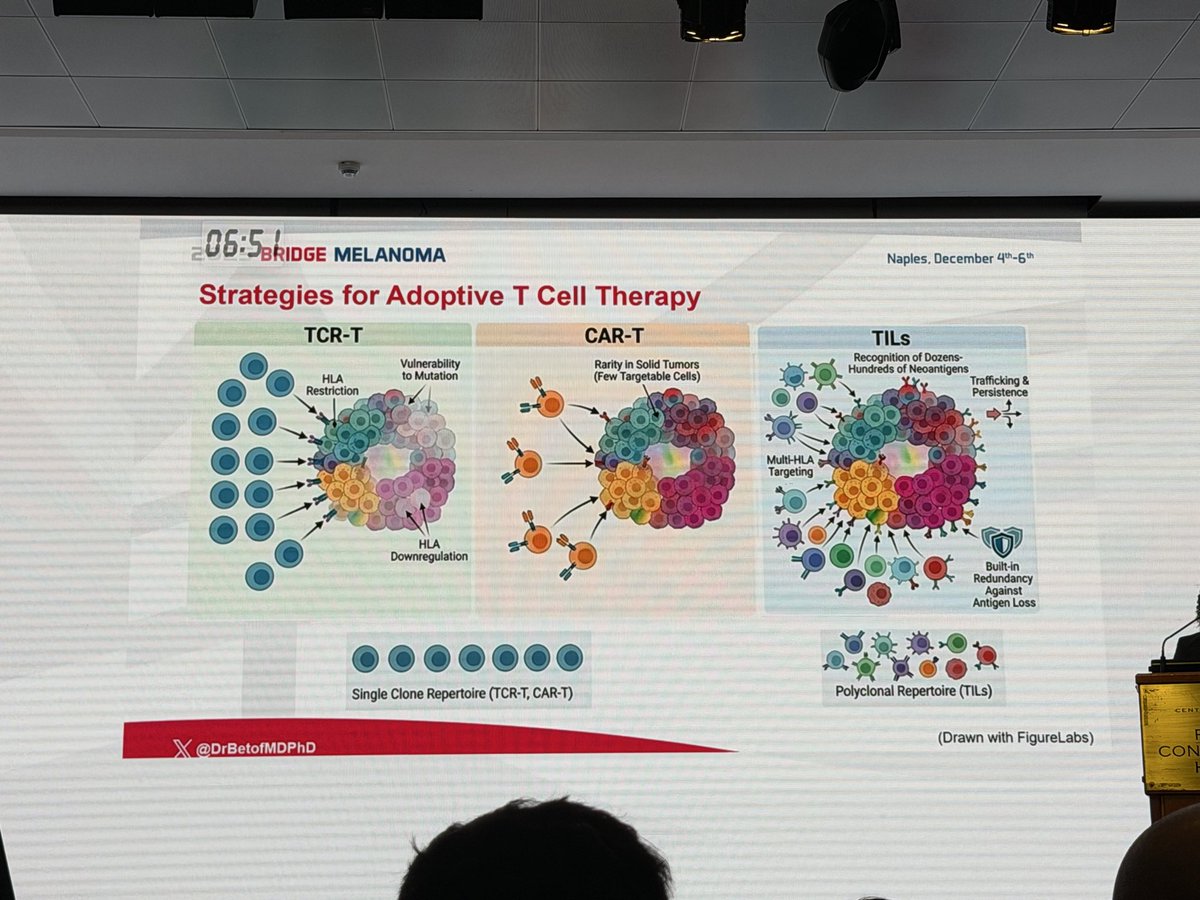
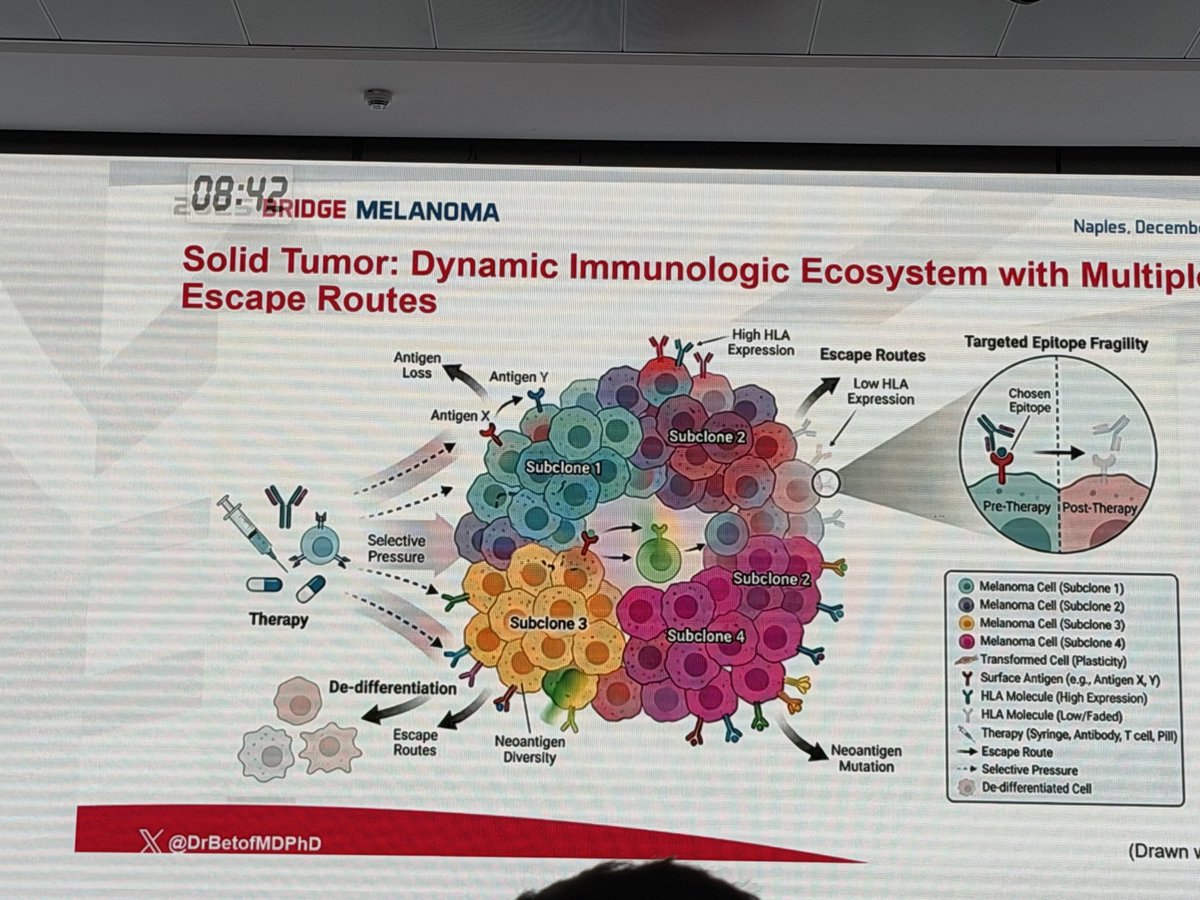
@DrBetofMDPhD#Melanoma immunotherapy expert @Stanford gives brilliant defense of TIL vs TCR-T or CAR-T cell therapy/Concept is #TIL are polyclonal and can better deal with variants: see slides/+ patients with CR have 96% 10 yr disease-free survival (NCI Surgery Branch data).
The ramp up of cancer immunotherapy is remarkable. Now we're seeing vaccines achieve some cures or remissions in the most refractory cancers: pancreatic, melanoma, glioblastoma, renal, triple-negative breast cancer.
✓ out the new Ground Truths (link in profile)
$IOVA - The leader in TIL therapy is already making a difference. It’s just beginning. Look at “Melanoma (metastatic): 16% to 35%” Amtagvi will continue to do its part to lift the number higher.
Next, “Lung (metastatic): 2% to 10%.” Even though there is improvement, look how low survival rates are for lung cancer. Amtagvi already demonstrated “best in class” interim data with ORR at 26% and duration of response NOT REACHED in NSCLC. This is unbelievable data. In case you don’t know, NSCLC is much deadlier and harder to treat than metastatic melanoma. So the 26% ORR is very good. Approximately 12 thousand people die from lung cancer every month IN THE US ALONE! Amtagvi is possibly a year away from potential approval for NSCLC.
Don’t forget, on February 24, 2026,“The U.S. FDA granted Fast Track Designation (FTD) for Amtagvi (lifileucel) for the treatment of adults with metastatic nonsquamous (NSQ) NSCLC that has progressed on or after chemo and anti-PD-1 therapies and at least one line of FDA-approved targeted therapy, if indicated, for actionable tumor mutations excluding ALK, ROS1 and EGFR.”
For those who spread FUD about single arm trial for LUN-202. The FDA and Iovance AGREED on the design of the trial. The FDA doesn’t just freely hand out Fast Track Designation these days. This tells me the FDA is 100% on board with everything. The fast track will now allow for even more communications between the company and the FDA. Iovance brought in multiple former high ranking FDA officials to make sure the company is fully cooperating with the FDA. CEO Fred Vogt works hard without going on CNBC to cry and whine.
Iovance is executing its plans extremely well. Everyone @IovanceBio is working hard to make the company profitable as soon as possible. It’s about to get real and fun. 🔜🤑
🧬 Can we convert “cold” tumors into immunotherapy responders?
Most MMR-proficient (MSS) cancers don’t benefit from checkpoint inhibitors.
This Cancer Discovery study tests a bold idea:
👉 Pharmacologically induce MMR deficiency
🔬 What they did
Developed NP1867 - a first-in-class PMS2 inhibitor
→ Directly blocks mismatch repair (MMR)
📊 Biological impact
NP1867-treated cells developed:
• ↑ Tumor Mutational Burden (TMB)
• MSI-High phenotype
• MMR-deficient mutational signatures
🧪 Functional impact (key finding)
Previously resistant tumors became:
👉 Sensitive to anti-PD-1 therapy
In murine models:
• ↑ Tumor-infiltrating lymphocytes
• ↑ T-cell and cytotoxic activity
• ↑ Antigen presentation (MHC pathways)
• ↓ Tumor growth with PD-1 blockade
🧠 Concept shift
This is NOT just immunotherapy
👉 It’s tumor reprogramming
Turning MSS → MMR-deficient → CPI-responsive
⚠️ Reality check
• Entirely preclinical
• Lead drug NOT suitable for long-term in vivo use yet
• Safety of inducing MMR deficiency in humans remains unknown
📌 Takeaway
A provocative strategy:
👉 Instead of selecting the right patients for IO
👉 Engineer tumors to become IO-sensitive
Could expand checkpoint benefit beyond MSI-H disease.
🔖 Bookmark this - conceptually important for future IO combinations
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #Immunotherapy #CancerDiscovery
@OncoAlert@JCOPO_ASCO@ASCO@myESMO
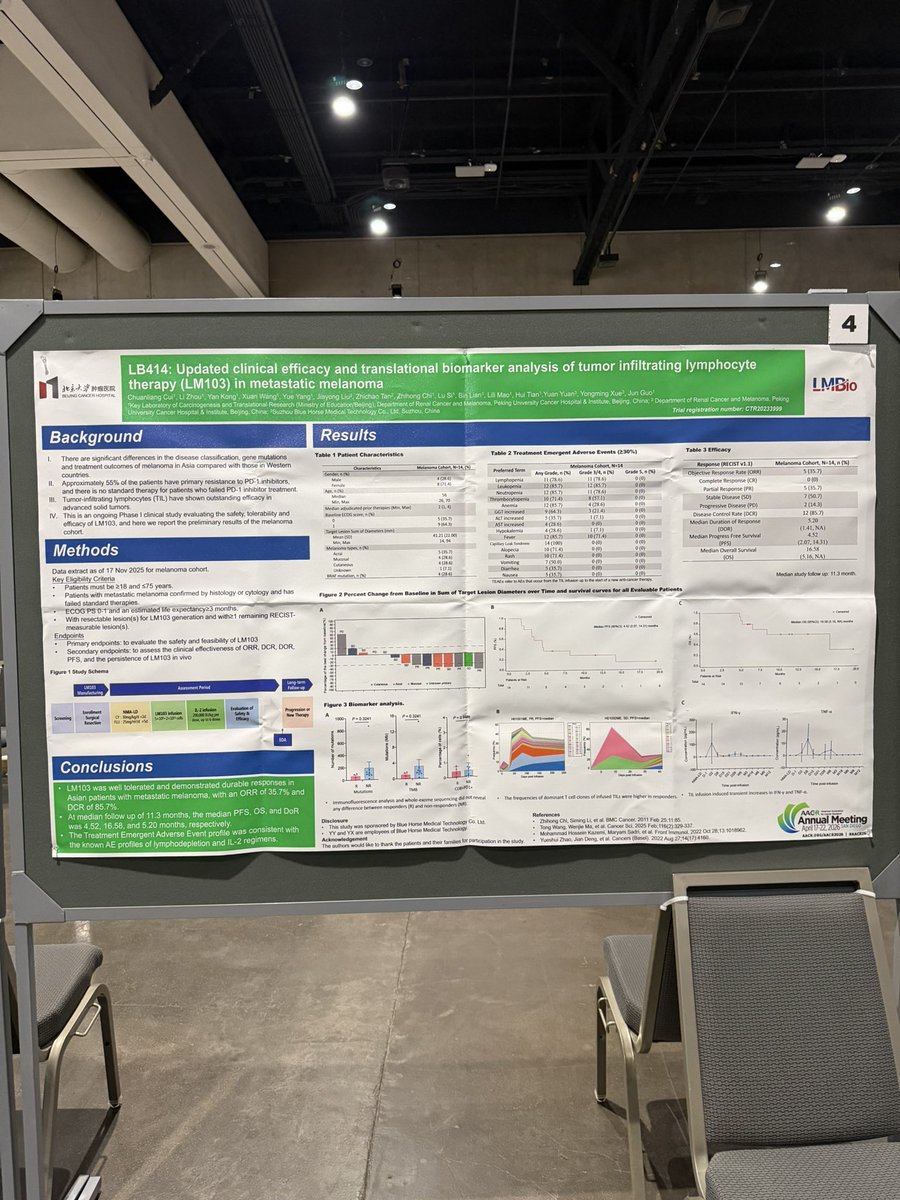
🧬 New data for LM103 presented at #AACR shows highly promising efficacy in Asian patients—a population historically underrepresented in trials and with distinct melanoma profiles compared to Western cohorts.