@drtimbracey@GI_Pearls@PathPro@TobyASchmitt@Pathoutlines I fully agree. There is a high suspicion of Hp in presence of superficial band of inflammation. If I don’t easily see Hp I order stains. I also order stains if there’s a prior hx of Hp.
Interesting I didn’t realize it wasn’t standard practice to stain all sentinel LN. We’ve been doing it since the beginning. But that’s brings up questions. 1. Why did we have the category of ITC in the first place? It’s like saying there’s no LVI and yet you have nodal metastasis. (Sort of like you’re only a little pregnant) 2. Are you and other institutions going to routinely stain sLN now that they have prognostic significance? I can say that there have been many instances where I only identified Mets because of IHC. This is now supported by the article that it has prog. sig.
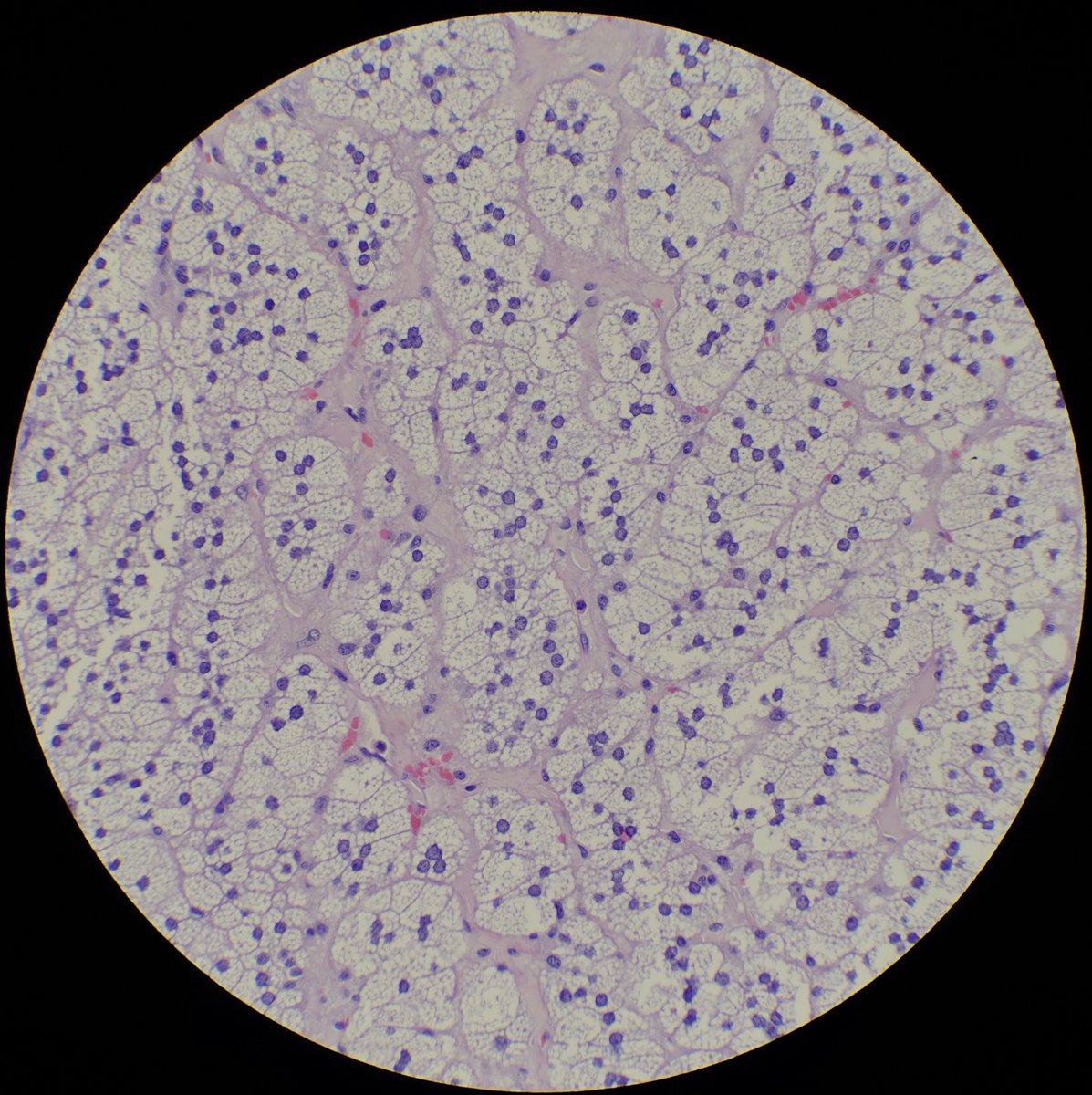
These 2 abdominal tumors came today. They have similar architecture but different cytologic features. Which is the bad and which is the Ugly? #PathTwitter#pathart#GuPath#surgpath
It’s like meeting an old friend in an unexpected place. This is an Inverted Papilloma. As izzypath noted “basiloid cells with peripheral palisading”. They most commonly occur in the trigone region of the bladder so it’s reasonable to assume that this was biopsied during the TURP.
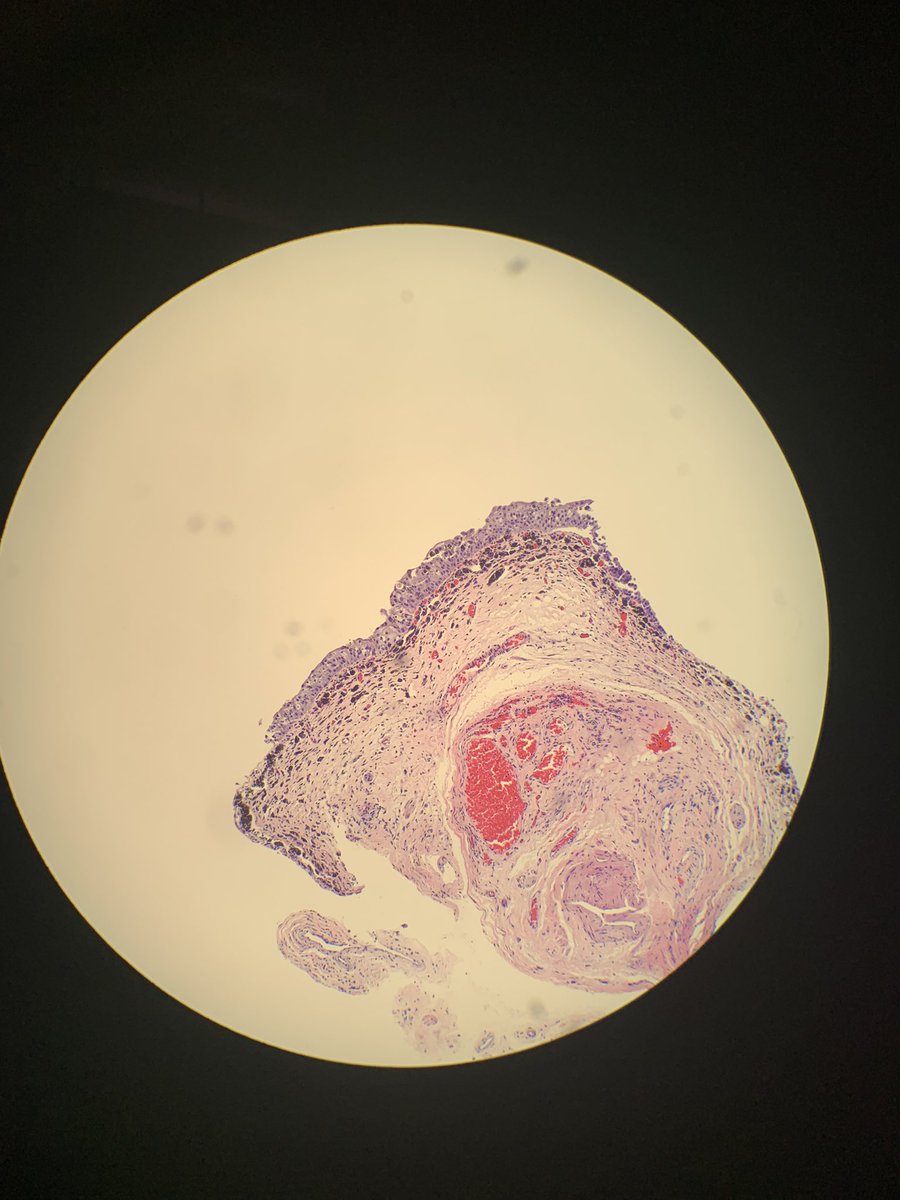
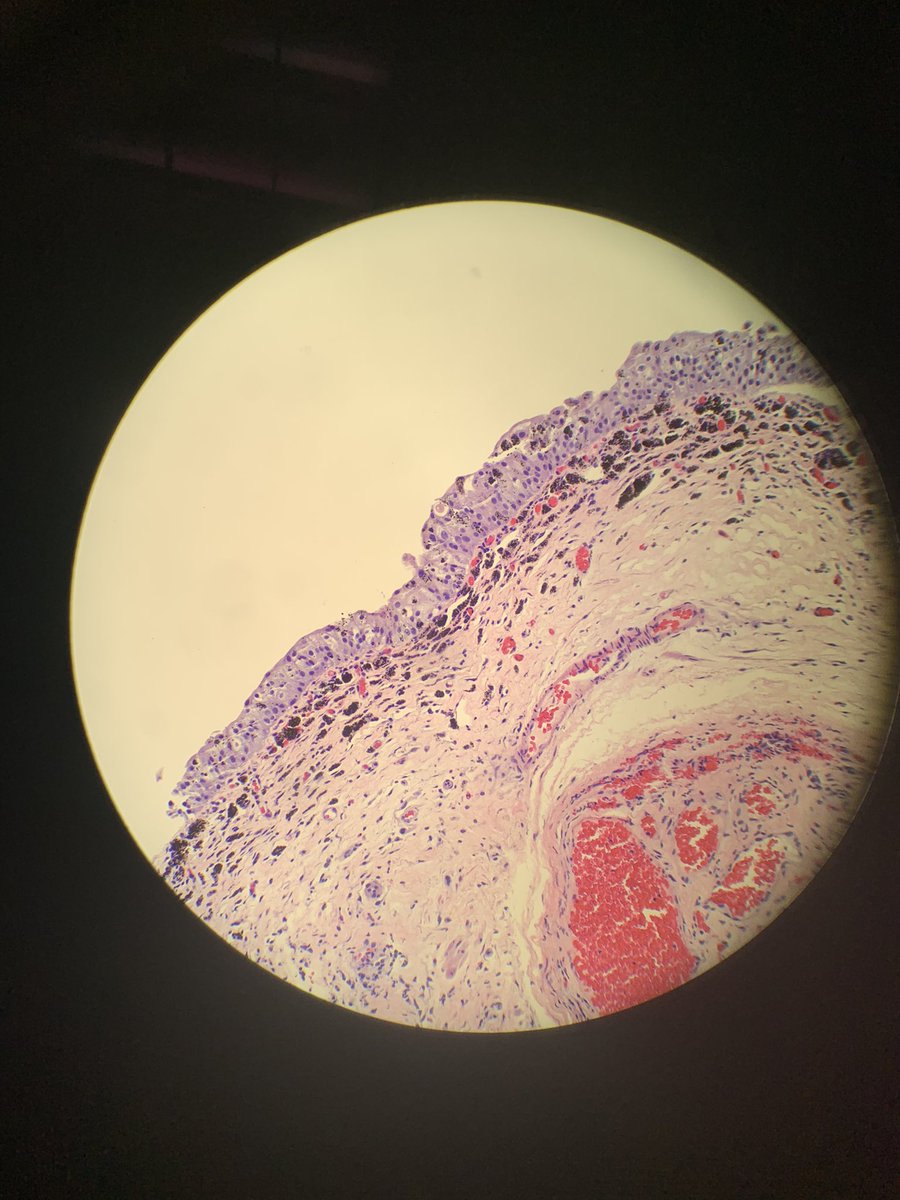
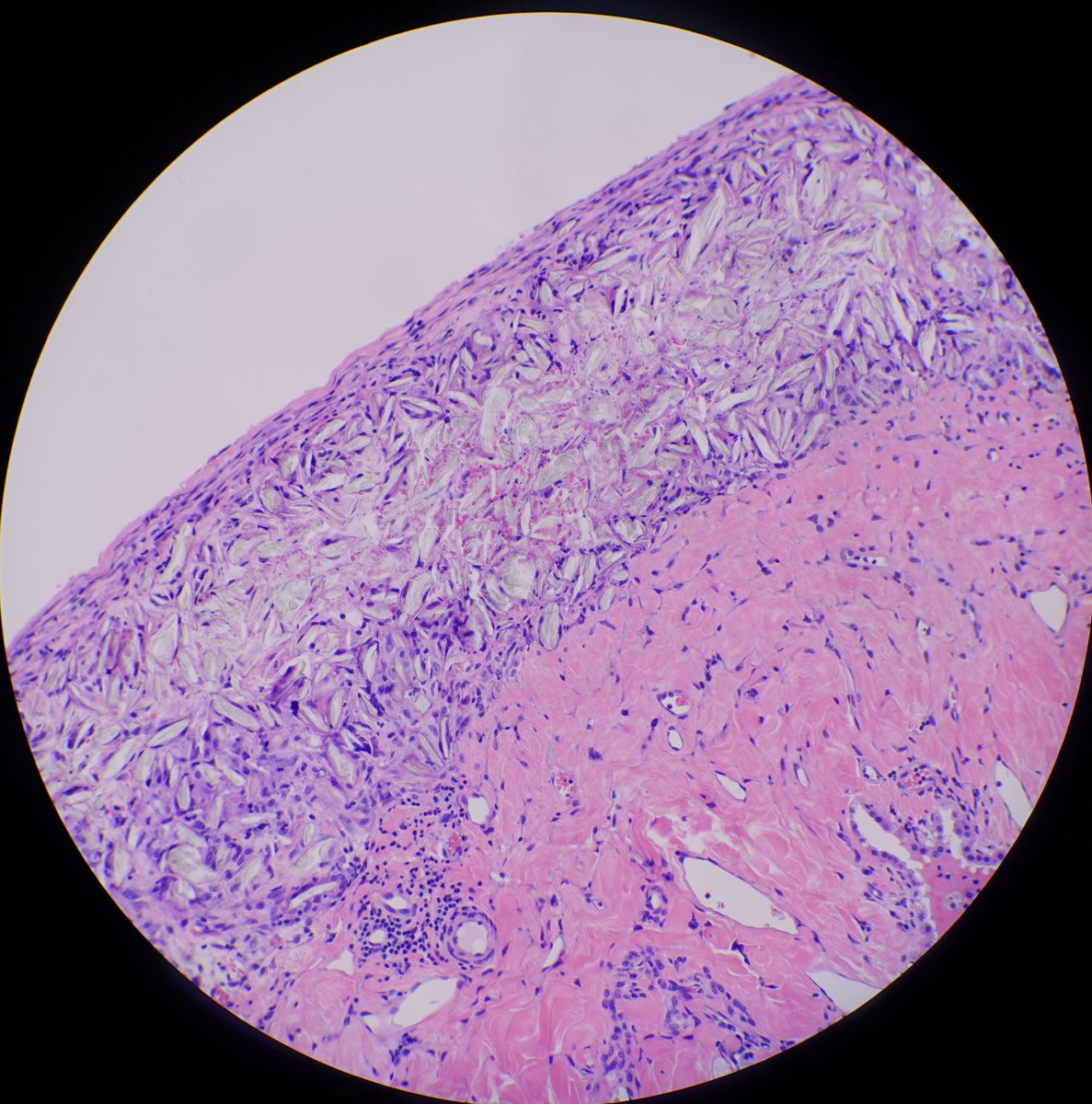
It’s the result of talc peurodesis. A procedure that involves injecting sterilize talc powder into the plural space, causing a tissue reaction, coating the plural, and trying to prevent the recurrence of pneumothorax.
Hx is everything. Gentleman in his late 70s with severe emphysema, blebs and spontaneous pneumothorax. He under went VATS, decortication, wedge resection and talc pleurodesis but with continued bronchopleural fistula.
@pathphyo Idk. Non-necrotizing, could be cross contamination. Be sure to correlate with serological studies. Otherwise congratulations on a successful hunt.