**TCOL Alert!** Editor’s Pick of the Month
Ileal Pouch Anastomosis for Ulcerative Colitis: What are the differences between two-stage and three-stage procedures?
Stay tuned for this month's virtual discussion in Techniques in Coloproctology, hosted by Dr. Kotze, and the authors!
Primary entry trocar design and entry-related complications at laparoscopy in obese patients: meta-analysis
https://t.co/vMyww0K1Ak
Our latest systematic review and meta-analysis reports the frequency of resultant visceral and vascular complications, at first entry and by entry device type, in specified obese classes of patients undergoing laparoscopic abdominal surgery.
#SoMe4Surgery #SurgEd #MedTwitter
@BJSAcademy@BJSurgery@juliomayol@young_bjs
Global cost of postoperative ileus following abdominal surgery: meta-analysis
https://t.co/VU14LMc6yq
Background
Following abdominal surgery, postoperative ileus is a common complication significantly increasing patient morbidity and cost of hospital admission. This is the first systematic review aimed at determining the average global hospital cost per patient associated with postoperative ileus.
Methods
A systematic search of electronic databases was performed from January 2000 to March 2023. Studies included compared patients undergoing abdominal surgery who developed postoperative ileus to those who did not, focusing on costing data. The primary outcome was the total cost of inpatient stay. Risk of bias was assessed using the Newcastle–Ottawa assessment tool. Summary meta-analysis was performed.
Results
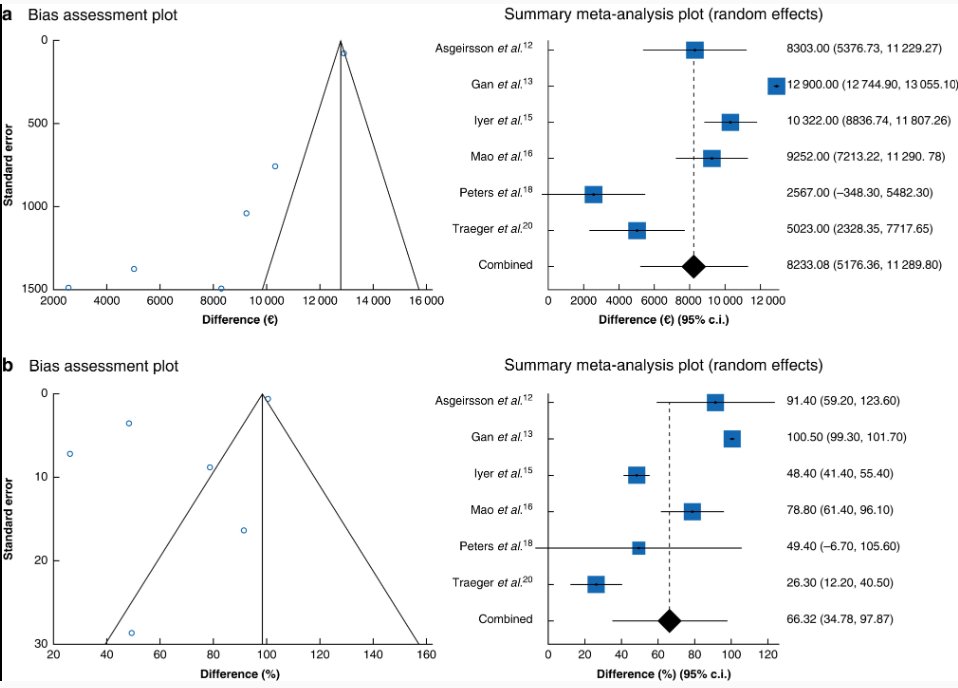
Of the 2071 studies identified, 88 papers were assessed for full eligibility. The systematic review included nine studies (2005–2022), investigating 1 860 889 patients undergoing general, colorectal, gynaecological and urological surgery. These studies showed significant variations in the definition of postoperative ileus. Six studies were eligible for meta-analysis showing an increase of €8233 (95 per cent c.i. (5176 to 11 290), P < 0.0001, I2 = 95.5 per cent) per patient with postoperative ileus resulting in a 66.3 per cent increase in total hospital costs (95 per cent c.i. (34.8 to 97.9), P < 0.0001, I2 = 98.4 per cent). However, there was significant bias between studies. Five colorectal-surgery-specific studies showed an increase of €7242 (95 per cent c.i. (4502 to 9983), P < 0.0001, I2 = 86.0 per cent) per patient with postoperative ileus resulting in a 57.3 per cent increase in total hospital costs (95 per cent c.i. (36.3 to 78.3), P < 0.0001, I2 = 85.7 per cent).
Conclusion
The global financial burden of postoperative ileus following abdominal surgery is significant. While further multicentre data using a uniform postoperative ileus definition would be useful, reducing the incidence and impact of postoperative ileus are a priority to mitigate healthcare-related costs, and improve patient outcomes.
#SoMe4Surgery #SurgEd #MedTwitter #systematicreview @BJSAcademy@BJSurgery@juliomayol@young_bjs
Efficacy and safety of advanced oral small molecules for inflammatory bowel disease: Systematic review and meta-analysis. @vipuljairath
https://t.co/r80V9GzMX2
Fig 2: JAK inhibitors for inducing clinical remission in UC
@Y_ECCO_IBD@DignassAxel@RajaAtreya@I_Blumenstein
@JeffSternberg1 this is becoming my go to for Pilonidal disease. Patient did amazingly well and very happy. Thanks!! Head over to @surgeonapp1 to watch Dr. Sternberg discuss The Cleft Procedure for Pilonidal disease. https://t.co/q5i8v2wDLq
Better pCR but worse local recurrence w short course TNT in RAPIDO is counterintuitive.
This piece suggests could be due to fragmentation.
Fragmentation occurs after prolonged delay between RT and surgery and leads to pockets of isolated tumor cells including outside mesorectum.
So RO resection (even pCR), but still residual cancer - hence local recurrence.
A good read.
https://t.co/ioImiltXqO