@LAzzaliniMD Still, there’s something abnl going on
Slow resting coronary flow (by angio) is confirmed by the broad blue TD curves ➡️ long transit time = 2.4 sec (usu ~ 1.0 s)
Hence, rest IMR very high… but normalizes w/ adenosine. No CMD, but something telling microvasc to vasoconstrict
@IhabFathiSulima@Abdul_alkindy Great example of a mid-LAD myocardial bridge. Usually not clinically important, but can in some patients be symptomatic. Also, many bridges cause diastolic restriction as can be seen subtly in your first screenshot 👀
More info 👇🏼
#CUBISM by SHOCKWAVE
Remarkably circumferential coronary calcium (1.4 mm thick!) 👀
➡️ Beautifully fractured by #Shockwave IVL alone
“Violin and Candlestick” by Georges #Braque#CardioTwitter#OCT
@jbspadoni Fantastic case 👏👏
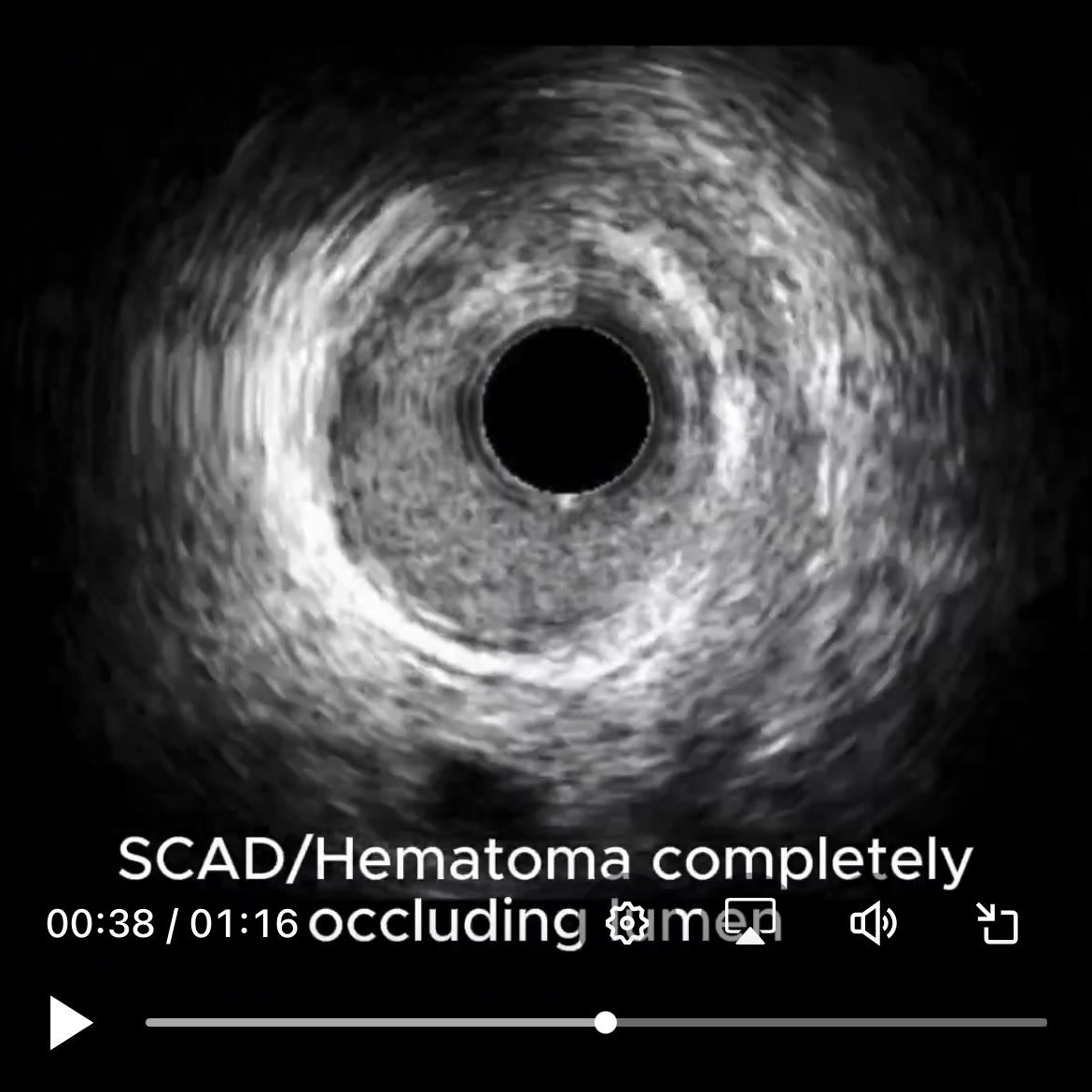
Btw, your #IVUS is another great example supporting “mechano-cardiac” (@rajivxgulati) causes for SCAD, eg takosubo, #myocardialbridge. Your patient’s bridge is exactly at proximal end of hematoma (bridges are not only found in LAD!):
@MichaelMegalyMD@MichaelMegalyMD So do you not modify your use of contrast in CKD patients, e.g limiting numbers of angiographic views, tending away from OCT, staging PCIs, etc?
@jbspadoni Hmm, doesn’t look like bridge or SCAD / hematoma to me. Maybe a vein coursing around the coronary?
@jbspadoni do you know what this is? (Why was IVUS done in this otw normal looking coronary?)
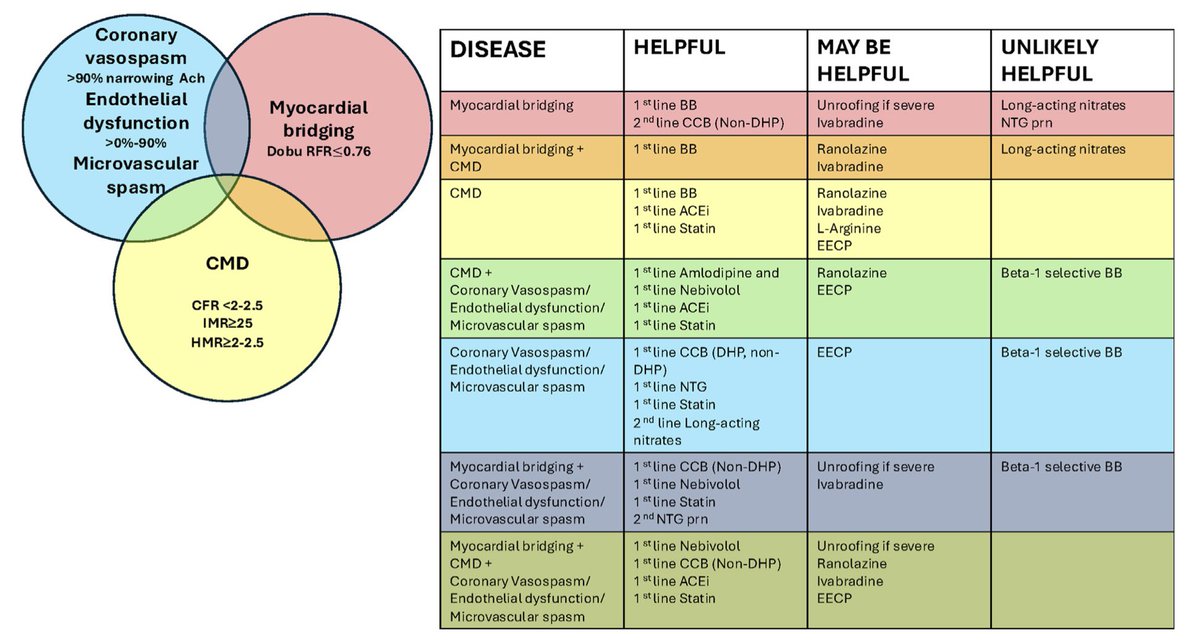
@sbrugaletta@AntonioMariaLe2@ehj_ed@ESC_Journals@escardio Our current terminology is problematic for these reasons but also because these same entities (ie vasospasm, microvascular dysfunction, myocardial bridges, etc) can often cause angina / ischemia in pts who ALSO have epicardial CAD, eg those who don’t improve with PCI / CABG