@PatsyDiabetes Good advice. Evidence shows wearing enough masks to simulate COPD or emphysema offers gold standard protection from function gained virus. I typically wear 8-10 until I find my breathing sufficiently impaired. Better that than intubation!
@PatsyDiabetes No toxic nail polish entering through the feet. Hope your shelf has room for more Healer Cups. You remain a thought leader despite the need for shoes and socks to conceal your brilliance.
@PatsyDiabetes@MiocanDanijel@MohammedAlo He's recovering from an accumulation of endocrine disrupters from Tuperware. Has switched to Owens Corning and recovering.
@PatsyDiabetes Absolutely not. The vax mandate should have been crafted to withstand any legal challenge. After all, the function was unable to be gained further.
This viral thread from @bschermd is a great read.
Veins and arteries see the exact same LDL/ApoB, yet plaque forms almost exclusively in arteries — and a pristine vein grafted into arterial flow rapidly develops atherosclerosis.
That points strongly to hemodynamic stress and endothelial injury as the primary trigger (Response to Injury) over a pure Response to Retention model.
Our Keto-CTA data in a metabolically healthy cohort with a wide spread of LDL/ApoB (going from under 100 to over 500) show no association with either the presentation or progression of plaque.
Which is why we've needed to do this exact research for so long.
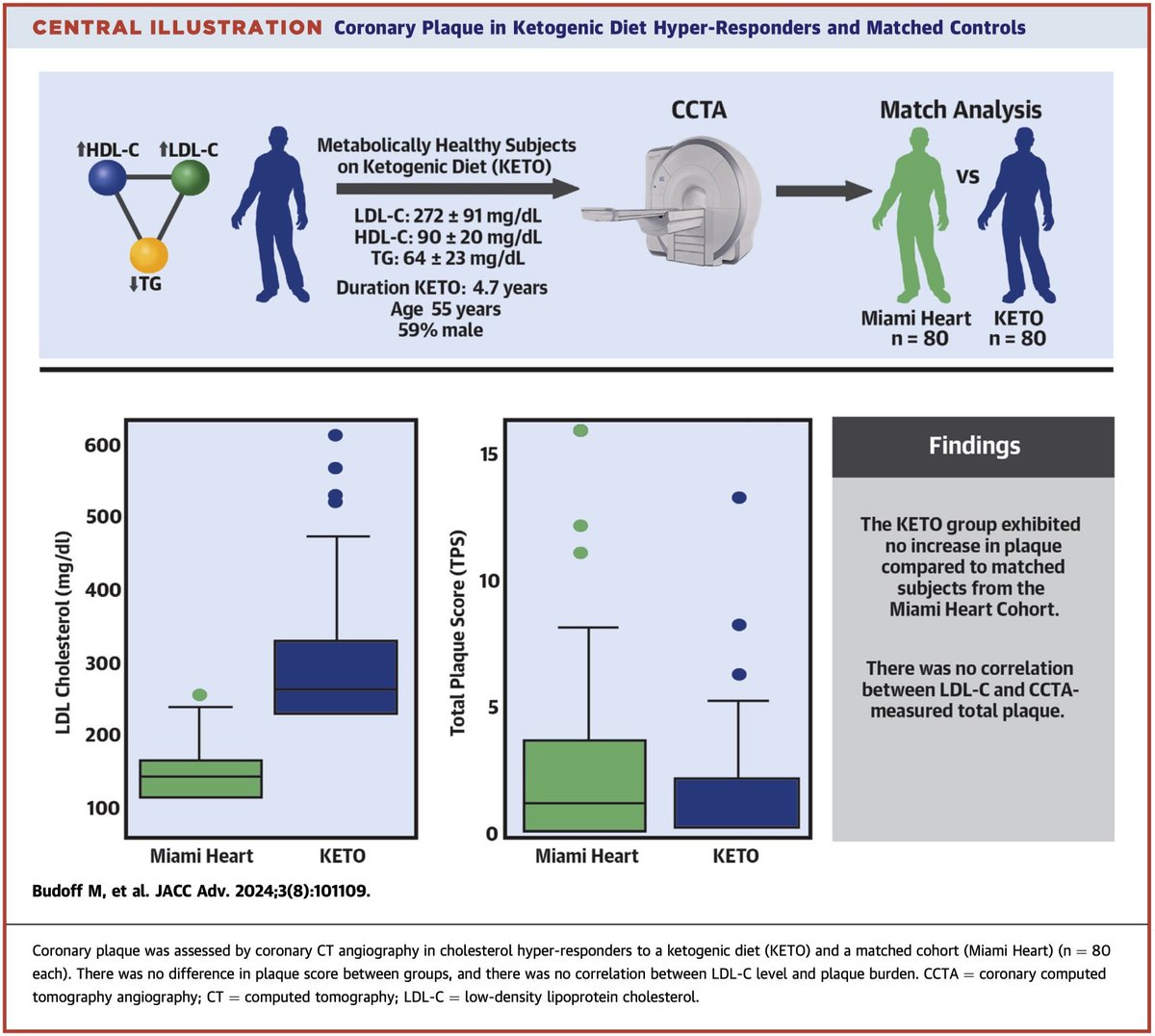
This central illustration is from our match analysis in JACC Advances (Budoff et al., 2024), where we compared 80 metabolically healthy ketogenic hyper-responders (mean LDL-C 272 mg/dL, HDL-C 90, TG 64, after 4.7 years on keto) to 80 tightly matched controls from the Miami Heart cohort (mean LDL-C 123 mg/dL).
Despite the ~149 mg/dL difference in LDL-C, there was no significant difference in coronary plaque burden by CCTA total plaque score, CAC score, or other measures. And crucially, there was no correlation between LDL-C levels and plaque burden in either group.
(Full paper: https://t.co/D6MY66oEoC)