El SOP —ahora PMOS (síndrome ovárico metabólico poliendocrino)— afecta a ~12% de las gestaciones globales (~17M/año), pero los registros perinatales solo capturan una prevalencia del 2-4%.
Nueva revisión en @NatureRevEndo ➡️factor de riesgo independiente de edad e IMC para DMG (OR 2,41), HTA gestacional (OR 2,20), preeclampsia (OR 2,30) y parto pretérmino (OR 1,53). Paradoja de crecimiento fetal: ↑IMC/DMG pero patrón de CIR y bajo peso (OR 1,28), probablemente por disfunción placentaria.
⤵️La guía internacional 2023 ya recomienda clasificarlo como gestación de “alto riesgo” y cribado con SOG en 1er trimestre.
🔗 https://t.co/yHI6l4gDaz
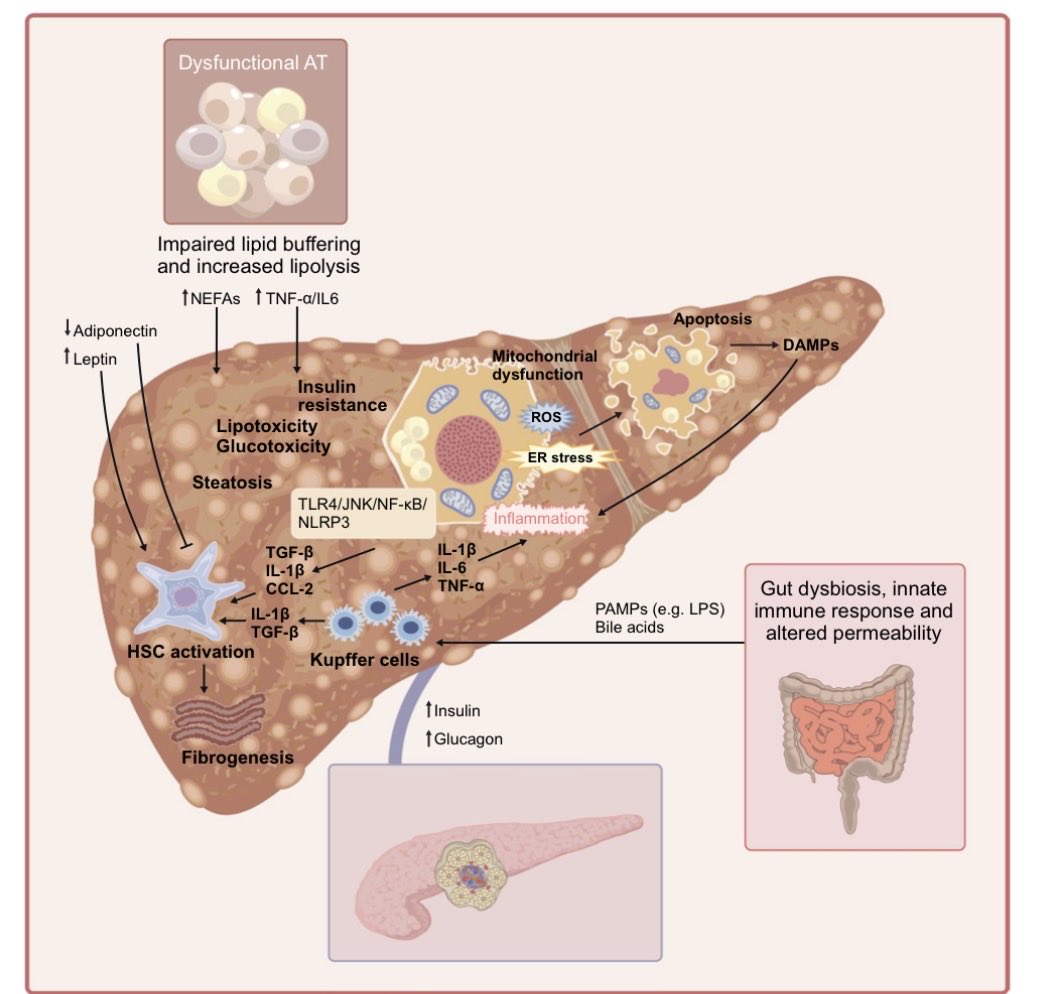
🔬 Nueva revisión en @DiabetologiaJnl ➡️los motores metabólicos de MASLD y MASH ➡️ del desequilibrio hormonal a la fibrosis.
🔹 La disfunción del tejido adiposo y el desequilibrio insulina–glucagón son el eje central
🔹 La fibrosis (no la inflamación) predice el pronóstico… y puede regresar si mejora la disfunción metabólica
🔹 Dianas terapéuticas con base mecanística: resmetirom (THR-β), AR GLP-1, lanifibranor (pan-PPAR), análogos FGF21/19
Medicina de precisión para frenar la progresión hepática 👇
🔗 https://t.co/K1crEXGIF6
The last decade brought extraordinary advances in cardiovascular medicine.
Yet our recent study in the JACC found that only 1 in 2 with CKM who need treatment for hypertension or hyperlipidemia are receiving it.
The therapies are here. Now we need to get them to patients.
👉OVER A CENTURY OF SCIENCE. ONE CONSISTENT MESSAGE.
☝️In medicine, few hypotheses have been tested as rigorously as the relationship between LDL cholesterol and atherosclerotic cardiovascular disease.
🐇 1913 – Nikolai Anitschkow demonstrated that cholesterol-rich diets induce atherosclerosis in experimental models.
❤️ 1948 – The Framingham Heart Study established the association between cholesterol levels and cardiovascular risk.
🏆 1964 Nobel Prize – Konrad Bloch and Feodor Lynen elucidated the biosynthesis and metabolism of cholesterol.
🏆 1985 Nobel Prize – Michael Brown and Joseph Goldstein discovered the LDL receptor, transforming our understanding of cholesterol regulation and familial hypercholesterolemia.
💊 1994 (4S Trial) – Lowering LDL-C with statins reduced cardiovascular events and mortality.
💊+ 💊2015 (IMPROVE-IT) – Further LDL-C reduction with ezetimibe translated into additional cardiovascular benefit.
💉2017–2018 (FOURIER & ODYSSEY Outcomes) – PCSK9 inhibitors demonstrated that achieving very low LDL-C levels produces further risk reduction.
🧬👫🏻🔬🩻Today – Genetics, epidemiology, pathology, imaging, Mendelian randomization studies, and randomized clinical trials continue to converge on the same conclusion.
More than a century of basic science and clinical research has consistently pointed in one direction:
👉LDL cholesterol is causal.
☝️Lower is better.
☝️Earlier is better.
☝️Longer is better.
When a scientific concept is supported by experimental biology, human genetics, epidemiology, randomized clinical trials, and two Nobel Prizes in Medicine, it is no longer merely a hypothesis.
🙌 It is biology.
@society_eas@nationallipid
🧠🫀¿Y si la grasa corporal fuera un órgano de comunicación?
Revisión en Nature 2026 redefine al tejido adiposo como centro neuroendocrino que conversa con cerebro, corazón, hígado y sistema inmune mediante adipocinas, lípidos bioactivos, vesículas y señales neuronales.
Role of Physical Activity in Obesity Treatment and Cardiometabolic Health: A Scientific Statement From the American Heart Association
👉Obesity rates have reached all-time highs, with obesity affecting 42% of adults in the United States.
👉An overview of evidence-based strategies for targeted weight loss counseling and for leveraging digital technology, particularly to engage patients and achieve realistic physical activity goals."
https://t.co/QJbVSeoZdK?
El día que fallece un ser querido significativo para ti, tienes 21 veces más riesgo de sufrir un infarto agudo al miocardio 💔 que cualquier otro día de tu vida
#EAPM
🧠 El tejido adiposo no es un simple almacén de grasa. Es un hub endocrino-neuronal que regula el metabolismo de todo el cuerpo.
Nueva revisión en @NatureRevEndo : adipoquinas + circuitos simpáticos/sensoriales coordinan lipólisis, termogénesis y sensibilidad a la insulina.
🔗 https://t.co/Oda9s3MC2c
How fast do SGLT2 inhibitors work in heart failure? Faster than you think.
📊 Time to first clinical benefit:
• EMPEROR-Reduced (Empagliflozin): Day 12
• DELIVER (Dapagliflozin): Day 13
• EMPEROR-Preserved: Day 18
• EMPULSE (acute HF): Day 15
• DAPA-HF: Day 28
Los GLP-1RA reducen las lipoproteínas remanentes postprandiales (apoB48↓, apoCIII↓) de forma independiente del peso.
Y ese remanente postprandial predice MACE mejor que el LDL en ayunas.
Review imprescindible en Circ Res 2026. 📄
https://t.co/CaWEOpNDb0
La ventana terapéutica temprana importa.
Lograr ≥15% de pérdida de peso en los 2 primeros años tras el diagnóstico de DM2 se asoció a:
🔻14% menos eventos macrovasculares
🔻10% menos microvasculares
✅ mejor control glucémico y de TA… con MENOS fármacos
n=72.480, datos reales (CPRD, UK). Estudio observacional: asociación, no causalidad. @DiabetesCareADA
🔗 https://t.co/O9b3KBscaf
En Palacio Nacional, recibí al presidente de la FIFA, Gianni Infantino, así como a representantes de federaciones y confederaciones, para darles la más cordial bienvenida a este gran país. Estamos en la víspera de la inauguración en México de la Copa Mundial de Fútbol 2026.
👉This new Mendelian randomization study, including more than 425,000 participants from the UK Biobank, provides important insights into the specific causal effects of Lp(a) and its implications for future Lp(a)-lowering therapies.
☝️Top 5 Take-Home Messages
1️⃣ Lp(a) exerts a direct causal effect on coronary artery disease (CAD), independent of LDL-C. This reinforces that Lp(a) is not simply another LDL particle, but an independent driver of atherosclerosis.
2️⃣ Among 1,456 phenotypes analyzed, only CAD and HbA1c showed direct causal effects of Lp(a). Most other associations appear to be indirect or mediated through other pathways, highlighting the remarkable specificity of Lp(a).
3️⃣ Very low genetically determined Lp(a) levels were not associated with a higher risk of type 2 diabetes. These findings provide reassuring evidence for the long-term safety of profound Lp(a)-lowering therapies currently under development.
4️⃣ The optimal Lp(a) threshold for myocardial infarction risk discrimination was ~86 nmol/L in Europeans and ~93 nmol/L in Africans, suggesting that clinically relevant risk may begin at lower levels than the current 125 nmol/L cutoffs adopted by many guidelines.
5️⃣ The study supports treating LDL-C and Lp(a) as complementary but distinct cardiovascular risk factors. Even with optimal LDL-C control, elevated Lp(a) remains a causal contributor to coronary disease, emphasizing the need for dedicated Lp(a)-lowering strategies.
☝️Bottom line: Lp(a) appears to have a highly specific causal role in coronary atherosclerosis, independent of LDL-C, while concerns about diabetes risk from very low Lp(a) levels are not supported by this large Mendelian randomization analysis.
🔓🔗 https://t.co/hR9dfiOzrJ
@society_eas@nationallipid@JACCJournals
Ha salido la nueva guía 2026 del síndrome cardiovascular-renal-metabólico (CKM) y trae cosas interesantes. Os dejo lo que me parece más destacable, lo bueno y lo que no me cuadra tanto 🧵 @AHAScience@ACCinTouch@AmDiabetesAssn@ASNKidney
Corazón, el riñón y el metabolismo no van por separado. Y es bueno ponerlo también sobre el papel.
Lo que más me gusta:
→ Se estadifica el CKM (0 a 4), también en niños, para frenarlo a tiempo y hasta hacerlo retroceder.
→ La obesidad se trata como la raíz, no como un factor más de la lista. POR FIN.
→ iSGLT2 y GLP-1 como modificadores de enfermedad
→ Mirar siempre el riñón con FGe + cociente albúmina/creatinina.
→ Y meten los determinantes sociales en la ecuación.
Sigo 👇
📖 Ya no podemos seguir viendo a nuestros pacientes como “el que vive con diabetes”, “el que tiene hipertensión” o “el que cursa con MASLD”.
Se acaba de publicar en @TheLancet una serie sobre condiciones cardiometabólicas múltiples (MLTC) que cambia cómo entendemos la fisiopatología.
🧵👇
📌 DOI: https://t.co/YIjVuLCVYZ
How should we manage obesity in CKM Syndrome Stages 1–3? The 2026 AHA/ACC guidelines give us a clear roadmap
Obesity management in CKM is stepped, personalized, and evidence-driven. No judgment, just action.
In today's @TheLancet there are 3 papers on cardiometabolic disease: biology, epidemiology, prevention/treatment.
The sobering and all to common story from womb to tomb conveyed in this graphic
https://t.co/rVs2Yz97NC
https://t.co/OpuJTia0bC
https://t.co/i714onXoCG