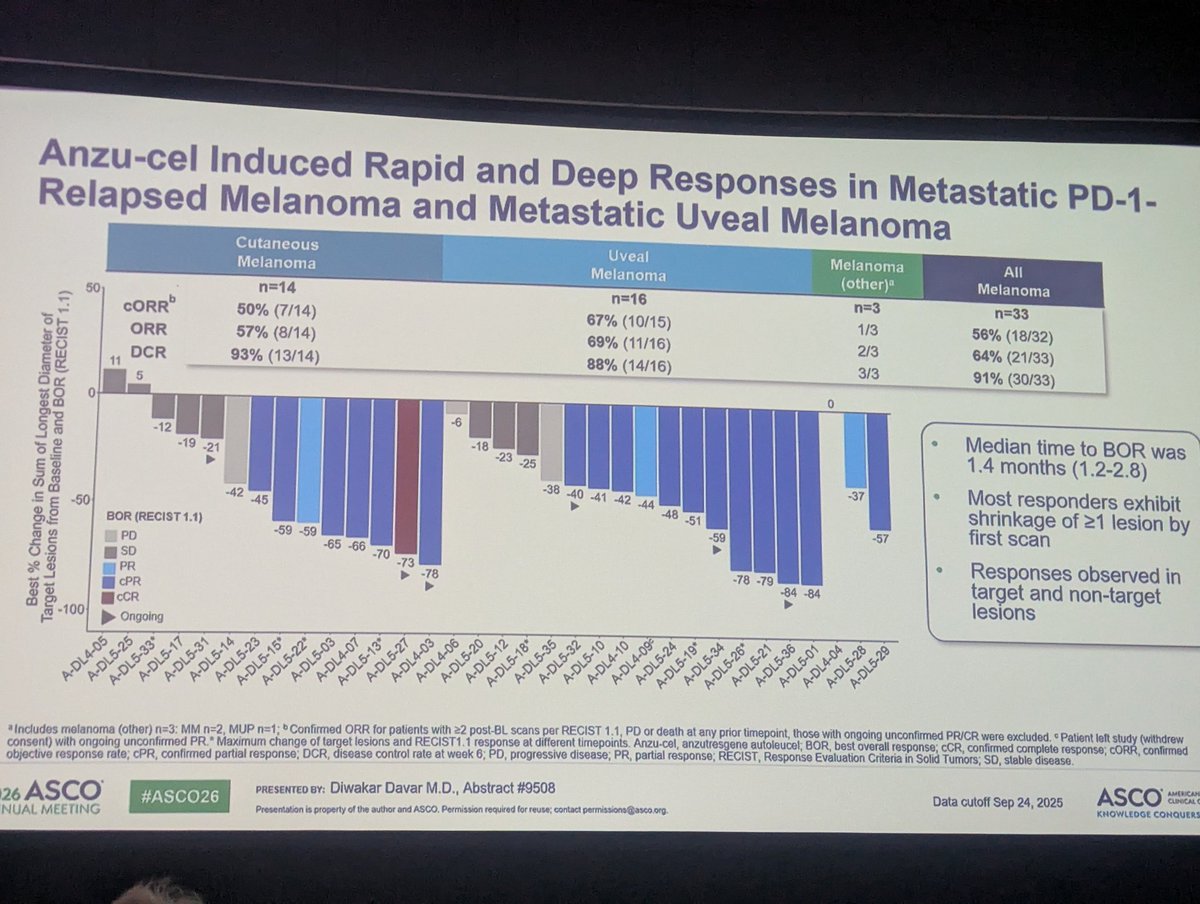
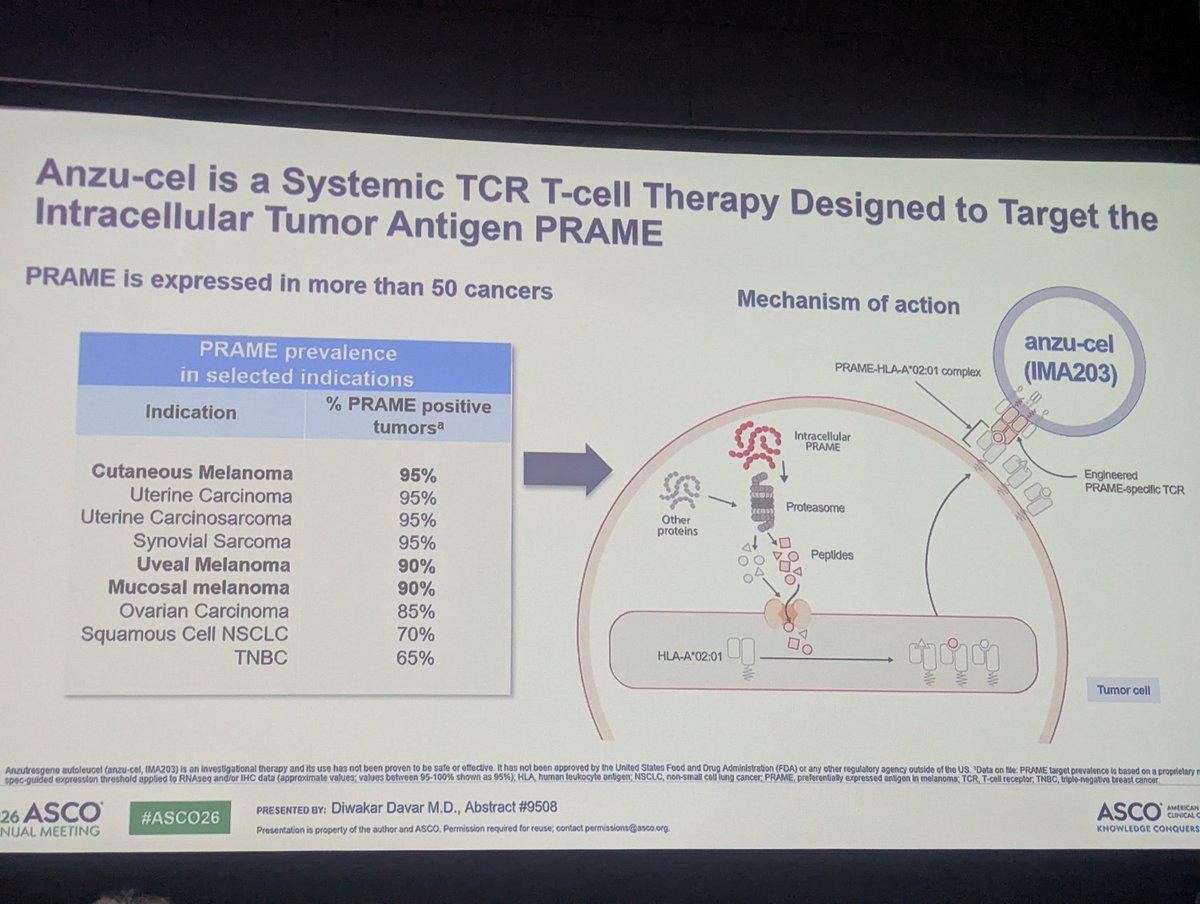
Concluding the excellent melanoma abstract session are the updated results of the IMA203 PRAME TCR T data. Promising durable responses and slower progression kinetics in those who progress. Another promising agent in the making for both CM and UM #ASCO26@diwakardavar@MRFCureOM
Another great presentation about the promising OBX115 TIL therapy by @DrBetofMDPhD, showing that modified TILs can be a viable option for frail patients without the need for toxic IL-2 and with a lower dose of LD chemo. Hoping to see larger cohort data moving this therapy forward
Great news for patients with metastatic uveal melanoma. Another treatment option coming soon with a great early signal with darvo+crizo in the first line setting. Impressive PFS improvement over ipi/nivo and manageable toxicity. #ASCO26@MRFCureOM
A great presentation by @ProfGLongMIA on the feasibility of neoadjuvant nivo/rela for high risk Stage II #melanoma . Promising signal, though significant irreversible endocrinopathies and open questions about the best regimen and duration in this setting #ASCO26
Another great signal to add to our growing arsenal of options in the neoadjuvant setting. Combining nivo/rela with low dose ipi leads to 73% MPR, a great step in the right direction. Still need better predictive biomarkers to stratify dosing intensity in this setting #ASCO26
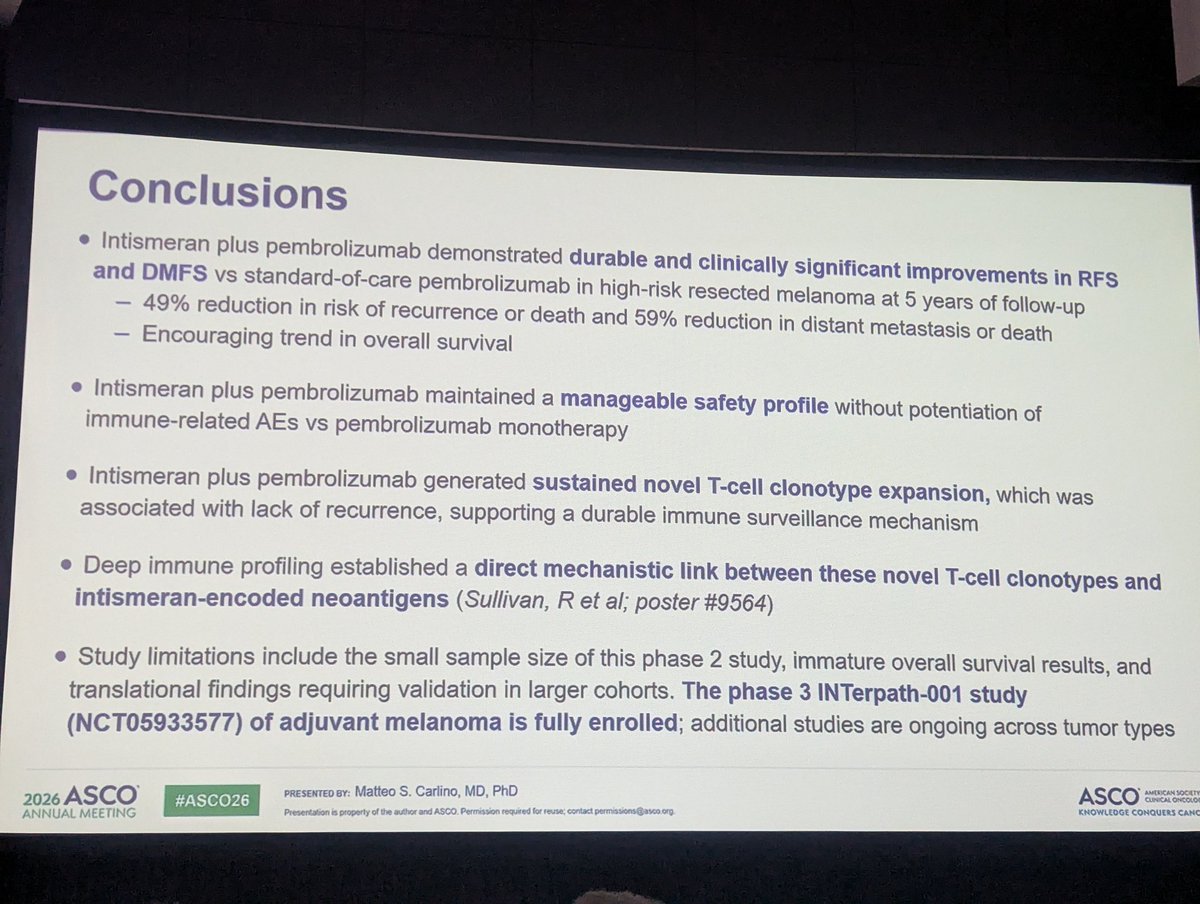
Great start to the #melanoma abstract session with the 5 year updated results of the adjuvant pembro + personalized mRNA vaccine. Nice TCR recruitment data, though still no OS signal as seen in all adjuvant trials to date. Waiting for the phase 3 results. #ASCO2026
Come and check out our data on the immune correlatives of patients treated with neoadjuvant combination of immunotherapy and targeted therapy for resectable Stage III #melanoma poster #289 at the melanoma poster session today 9:00-12:00. #ASCO26@TJH0828@MayoCancerCare
#ASCO 26 here we go! Great start to the morning with data on TIL efficacy in metastatic uveal melanoma with a possible predictive biomarker that could be used to select the optimal harvest site. A step in the right way to offer more therapies for this rare disease @MRFCureOM
Out now! Our new publication on the use of an in-house fast turnover ddPCR Liquid Biopsy for BRAF V600 Mutated Melanoma. A promising liquid biopsy assay that correlates with disease extent and PET-CT radiometabolic metrics. @YaldaNikanpour@MayoCancerCare https://t.co/xQGVmhB5b6
Out now, our new publication on the role of ctDNA as a predictive marker in
Stage III #melanoma patients treated with neoadjuvant combination of immunotherapy + targeted therapy in the NeoACTIVATE study. more to come soon on TCR and RNA seq @TJH0828@SU2C https://t.co/qjm5JcNikJ
I think it's clear that we are overtreating stage III (and probably stage IIB/C) with adjuvant immunotherapy. We need better predictive markers, hopefully ctDNA will be the one. Until then shared decision making with an honest discussion on irAEs is warranted
Original Article: Nivolumab for Resected Stage III or IV Melanoma at 9 Years (phase 3 CheckMate 238 trial) https://t.co/3i2wS5LFM1
Editorial: Changing Role of Adjuvant Therapy in Stage III Melanoma https://t.co/EZFvLvdd64
#Oncology
Our reflections on the use of PET/CT to assess treatment response following neoadjuvant treatment for Stage III melanoma. A short communication reflecting on past, present and future on the field. Still much to be explored @TJH0828
https://t.co/7bqkopqIrG
Is PET-CT a good predictor of the pathological response post neoadjuvant treatment in Stage III melanoma? We report on a cohort of real-world patients treated with immunotherapy alone or in combination with targeted therapy. @AnnSurgOncol@TJH0828 https://t.co/tNmh14Kecy
@EdWilli63968626@TJH0828@SU2C@MayoClinic Hard to compare across trials, as each has its own design and unique patient population features. I think the main theme is trying to find the optimal agents& duration while minimizing toxicity. Biomarkers are needed, perhaps a combination of ctDNA, imaging and immune signatures.
Great presentation by @TJH0828 on the promising results of the NEOACTIVATE arm C trial of anti TIGIT + anti PDL1 for clinical stage III melanoma. Correlative studies to follow in hope of identifying predictive biomarkers for better treatment tailoring. #ASCO25@SU2C@MayoClinic
Ending the melanoma session with data on treatment for BRAFm melanoma: the final DREAMseq data still showing that upfront ipi/nivo is superior to targeted therapy. For symptomatic brain mets, IO+TT combo improves PFS but not OS, maybe we should try quadruple therapy next #ASCO25
More neoadjuvant data, hard to choose from all these great options: anti TIM and TLR9 agonists could both enhance the pCR rate for stage III melanoma. TLR9 has higher response rates, yet harder to use with IT injections and 25% of patients not competing treatment course.#ASCO25
Neoadjuvant-adjuvant pembro for stage IIB/C melanoma is feasible and safe, yet RFS and DMFS are exactly the same as KN716. Interesting signal with decreased SLN positivity in clinical stage IIC patients, possible worth further exploration. #ASCO25
Unfortunately the study of adjuvant targeted therapy for stage IIB/C was terminated early, and only descriptive data on 110 patients is available. Numerically there is a difference, still not enough to act on for patients who aren't candidates for adjuvant immunotherapy. #ASCO25
Starting the closing melanoma session with the 098 study results - adding rela to nivo does not improve RFS or DMFS. Still need to better refine our patient selection for adjuvant therapy in stage III melanoma. #ASCO25@ProfGLongMIA