TRIPLE-NEGATIVE BREAST CANCER #ASCO2026
A clear theme emerged this year:
From immunotherapy-driven gains in early disease to ADC-driven advances in metastatic TNBC.
Key takeaways:
🔹 KEYNOTE-522: Durable 7-year survival benefit
🔹 ASCENT-04: ADC + IO moves into 1L PD-L1+ mTNBC
🔹 ASCENT-03: SG benefit observed across biomarker groups
🔹 TROPION-Breast02: Dato-DXd validates the TROP2 ADC class
🔹 PANKU-BREAST02: Bispecific ADCs represent the next wave of innovation
ASCO 2026 reinforced the transition from conventional chemotherapy toward ADC-based precision therapy in TNBC.
#TNBC #BreastCancer #ASCO #Oncology #ADC #SacituzumabGovitecan #DatoDXd #MVOnco
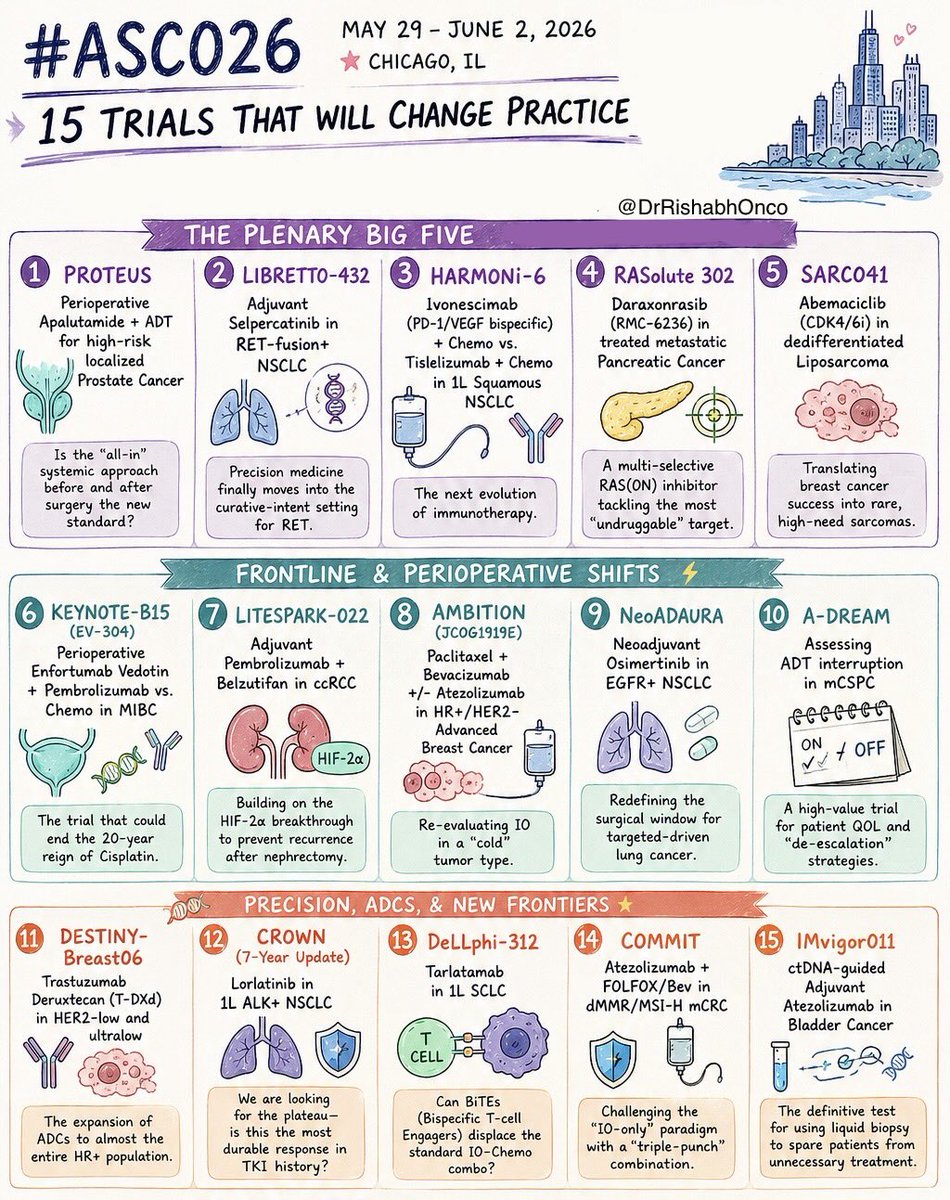
🚨 THE 15 MOST IMPORTANT TRIALS OF #ASCO26
May 29 - June 2 | Chicago
Which trial are you watching most closely?
🌟 PLENARY GAME-CHANGERS
1️⃣ PROTEUS
Perioperative apalutamide + ADT in high-risk localized prostate cancer
2️⃣ LIBRETTO-432
Adjuvant selpercatinib in RET+ NSCLC
3️⃣ HARMONi-6
Ivonescimab + chemo vs tislelizumab + chemo in squamous NSCLC
4️⃣ RASolute 302
Daraxonrasib (RMC-6236) in metastatic pancreatic cancer
5️⃣ SARC041
Abemaciclib in dedifferentiated liposarcoma
⚡ FRONTLINE & PERIOPERATIVE SHIFTS
6️⃣ KEYNOTE-B15 / EV-304
EV + pembrolizumab vs chemo in MIBC
7️⃣ LITESPARK-022
Pembrolizumab + belzutifan in adjuvant ccRCC
8️⃣ AMBITION
Paclitaxel/bevacizumab ± atezolizumab in HR+ breast cancer
9️⃣ NeoADAURA
Neoadjuvant osimertinib in EGFR+ NSCLC
🔟 A-DREAM
ADT interruption strategies in mCSPC
🧬 PRECISION, ADCs & NEXT-GEN IMMUNOLOGY
1️⃣1️⃣ DESTINY-Breast06
T-DXd expands into HER2-ultralow disease
1️⃣2️⃣ CROWN (7-year update)
Lorlatinib durability in ALK+ NSCLC
1️⃣3️⃣ DeLLphi-312
Tarlatamab in frontline SCLC
1️⃣4️⃣ COMMIT
Atezolizumab + FOLFOX/Bev in MSI-H mCRC
1️⃣5️⃣ IMvigor011
ctDNA-guided adjuvant atezolizumab in bladder cancer
#OncoTwitter #MedTwitter #ASCO26 #CancerResearch @OncoAlert@ASCO@JCOPO_ASCO@OncBrothers
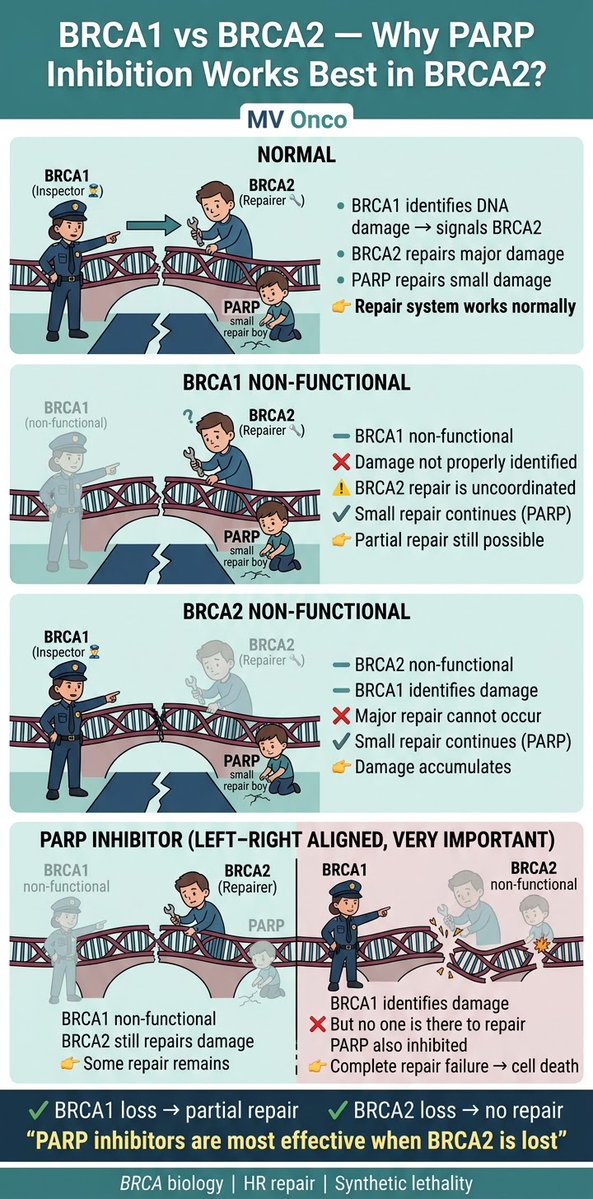
If you remember only one thing from BRCA biology, remember this👇
• BRCA1 → detects DNA damage
• BRCA2 → repairs DNA
• PARP → fixes small damage
Block PARP + lose BRCA2 → no repair left → cell dies
👉 That’s why PARP works best in BRCA2
#MVOnco#Oncology#MedOnc
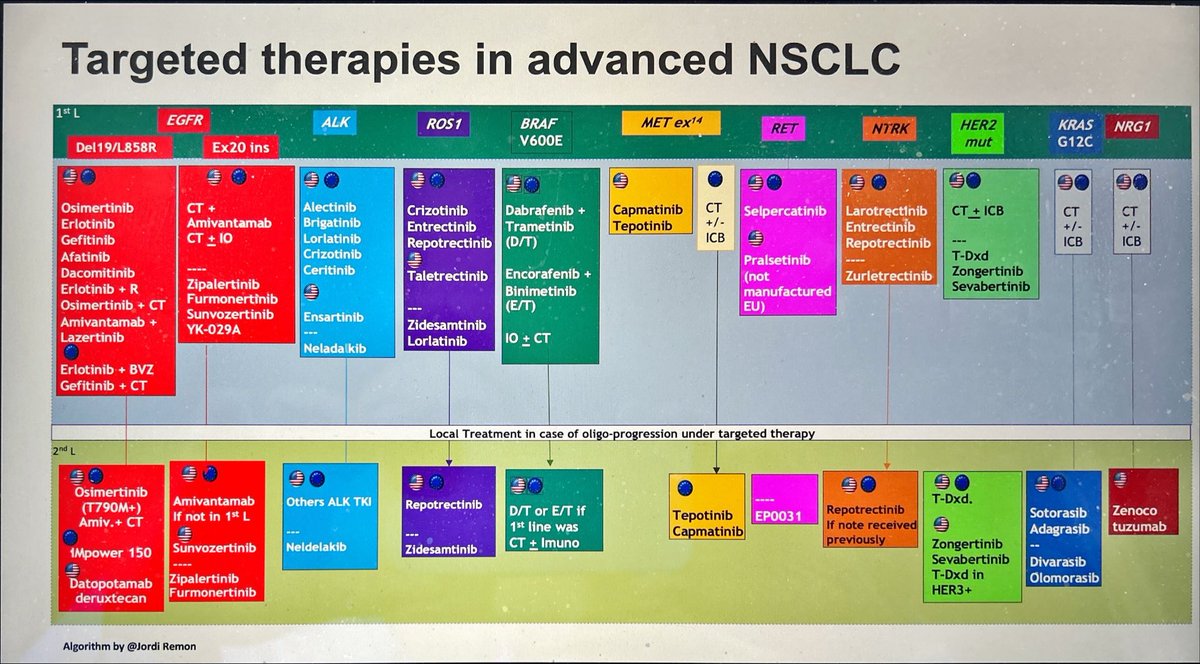
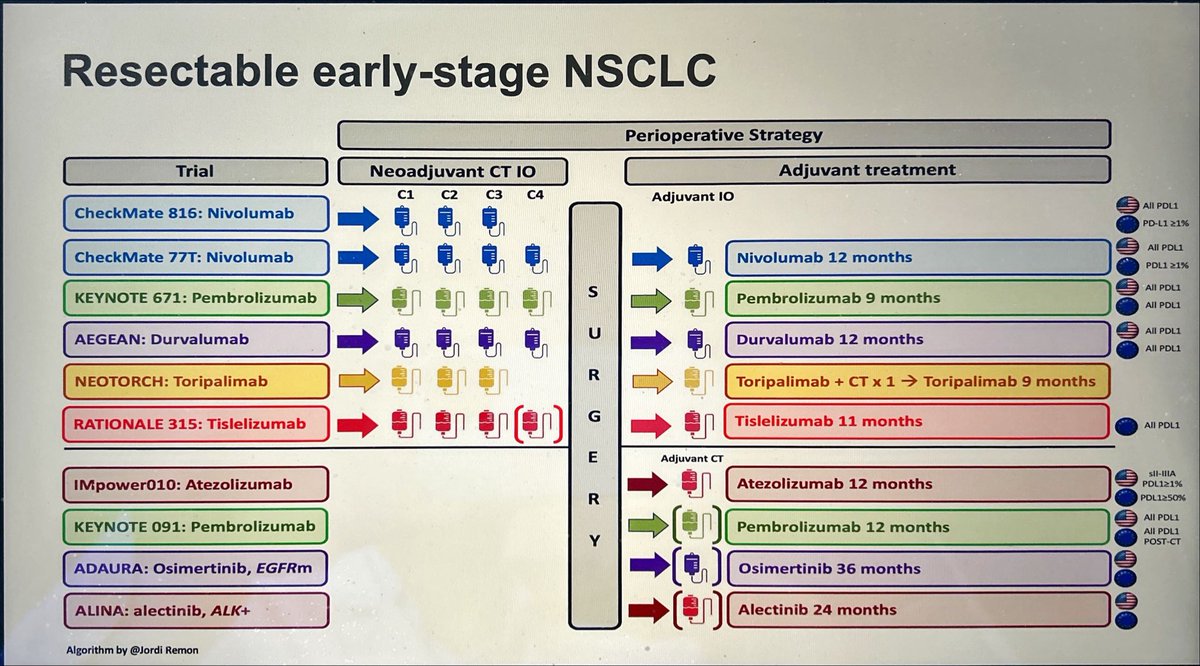
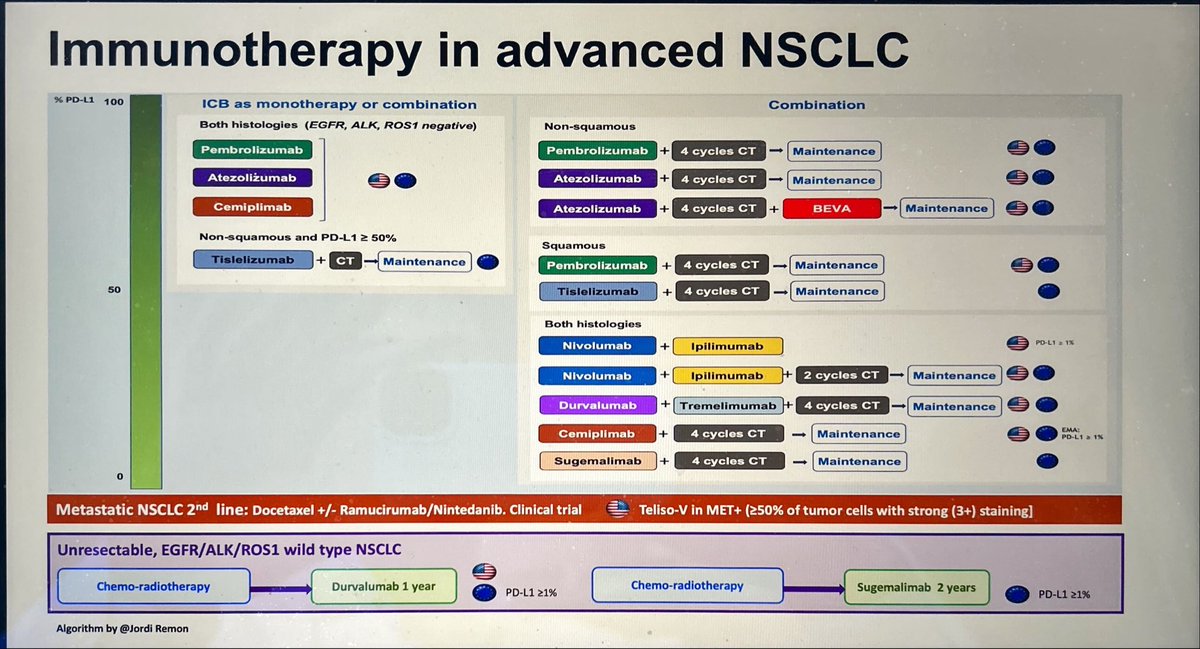
2025: Summary of Ttx for NSCLC in 3 slides
➕: IO is SoC in early stage
➖: multiple « me too » agents but cost of drugs is ⬆️ and access is ⬇️ worldwide
✏️: optimal Ttx duration with IO or TT
✏️: access to TT for rare 🧬altertions
✏️: role of ADCs?
We need more Academic trials!
☢️New meta-analysis in JAMA Network Open:
🎯Stereotactic body radiotherapy (SBRT) alone for oligometastatic cancer achieved 70% systemic therapy-free survival at 1-2 years, highest in renal (87%) and prostate cancer (78%).
🎯Low toxicity rates suggest SBRT may safely defer chemotherapy in selected patients.
10.1001/jamanetworkopen.2025.49685
@OncoAlert@DrYukselUrun #MedX #Cancer #Oncology @JAMANetworkOpen
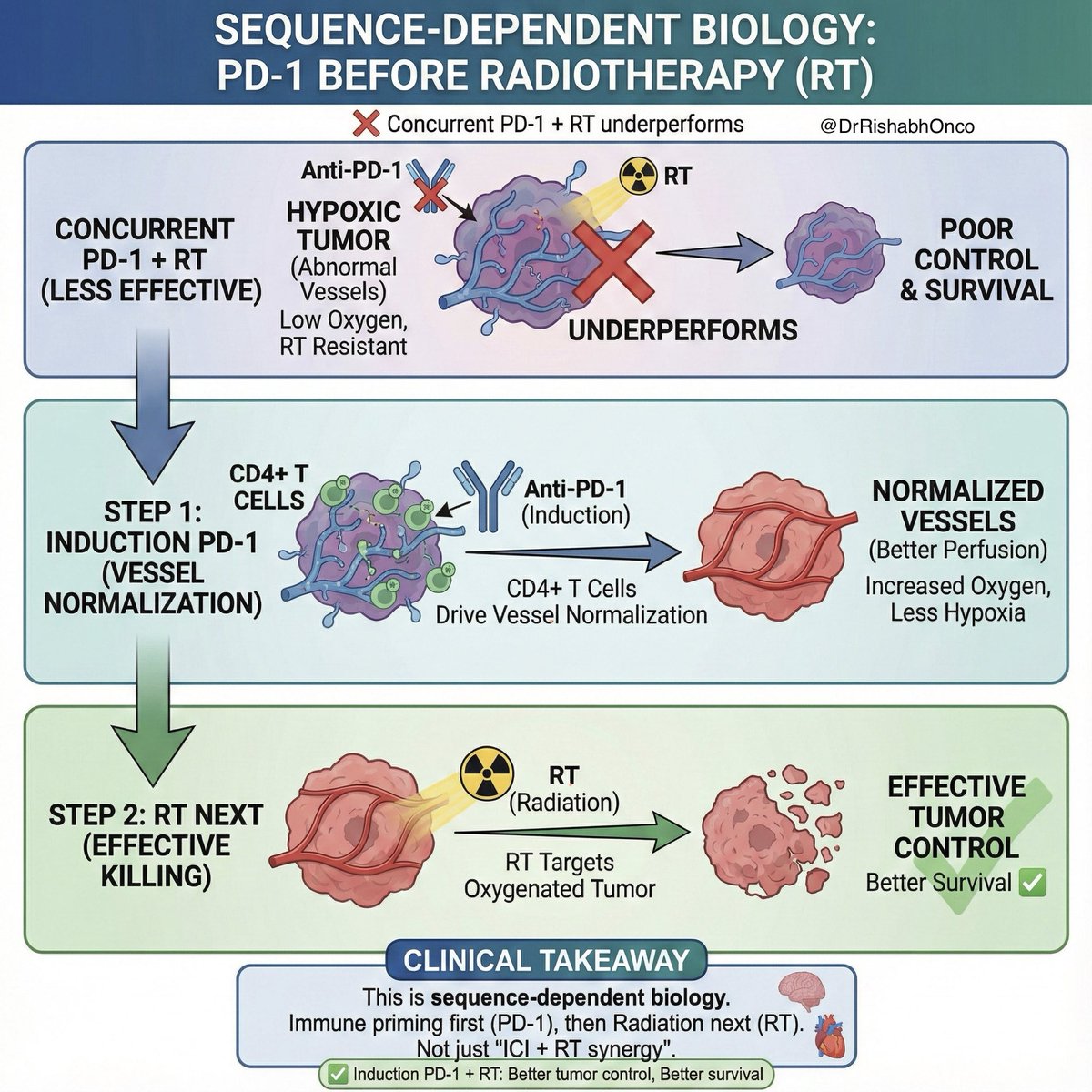
Why does PD-1 before radiotherapy work better than giving both together?
This paper explains it beautifully 👇
🧠 Tumors fail RT mainly because of hypoxia
🩸 Hypoxia exists because tumor vessels are abnormal
🧬 Anti–PD-1 given before RT fixes this problem
🔍 What happens biologically
🩺 PD-1 blockade normalizes tumor vessels
🫁 Better perfusion → less hypoxia → RT works better
🧠 This effect is driven by CD4+ T cells, not CD8+
📊 Key finding
Induction PD-1 + RT
✅ Better tumor control
✅ Better survival
❌ Concurrent PD-1 + RT underperforms
🎯 Clinical takeaway
This is not just “ICI + RT synergy”
This is sequence-dependent biology
Immune priming first
Radiation next
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #RadiationOncology #Immunotherapy
@OncoAlert@ASCO@myESMO@ESMO_Open
NCCN Breast Cancer Guidelines 2025 (v5) #update focuses on localized therapy:
• Less extensive axillary surgery—SLN biopsy may replace ALND in select pts.
• Hypofractionated post-mastectomy RT safe with reconstruction.
• Partial breast irradiation recommended for low-risk pts ≥40.
#BreastCancer #NCCN @Larvol@OncLive@ONCOLife_HP@OncoAlert
💥 Boost or Not to Boost? That’s the Cervical Question 🩸
In FIGO IIIC cervical cancer with radiologically positive LNs - does an external beam RT boost really help?
📊 Study Design
Retrospective (n = 231, 2012–2019)
All had node-positive disease
Compared: RT Boost vs No Boost
🎯 Key Outcomes
🕒 Median OS: 107 mo (Boost) vs 91 mo (No-boost) — p = 0.01 ✅
📏 No OS benefit if:
• LN > 2 cm → 105 vs 99 mo (p = 0.048)
• > 4 positive nodes → 91 vs 73 mo (p = 0.04) ❌
💊 Concurrent chemo improved survival + 22 mo (p = 0.023)
⏱️ Median DFS = 93 mo | Median OS = 84 mo overall
🧩 Best Outcomes Observed When
✅ LN < 2 cm
✅ < 4 nodes
✅ Concurrent chemo given
🧠 Take-Home Message
External RT boost 💪 improves survival in selected Stage IIIC cases-
but nodal size & burden matter more than dose.
📖 Rishi KS et al., IJGC Oct 2025
🔗 https://t.co/4COPqefmtH
#CervicalCancer #GynOnc #RadOnc #OncoTwitter
@ASCO@ESGO_society@myESMO@ESMO_Open@OncoAlert
“Can surgery still matter in metastatic prostate cancer?” 🩺
💥 RAMPP trial says maybe yes - even in low-volume mHSPC.
🧪 Design:
De novo low-volume mHSPC (≤5 bone mets ± nodes)
👥 Fit for RP + systemic therapy (ADT ± ARPI)
🆚 Radical prostatectomy (RP) + BST vs BST alone
🎯 Primary: Cancer-specific mortality (CSM)
📊 Results (~5 yrs):
•🩸 CSM: 13% vs 23% → HR 0.39, p=0.045 ✅
•🧭 Progression: 59% vs 60% (NS)
•💀 OS: 81% vs 74% (p=0.13)
•⚙️ Complications ≥ G3: 14%, no peri-op deaths
💬 Takeaway:
RP added to BST reduced CSM in low-volume mHSPC — mirroring the STAMPEDE RT signal 🔁
But OS gain unproven → discuss in MDT before adopting.
📖 Graefen et al. European Urology 2025.
🔗DOI: https://t.co/XMhMFVLHPW
#OncoTwitter #ProstateCancer #mHSPC #UroOnc
@OncoAlert@myESMO@ESMO_Open@ASCO@EuropeanUrology@EUplatinum@Uroweb
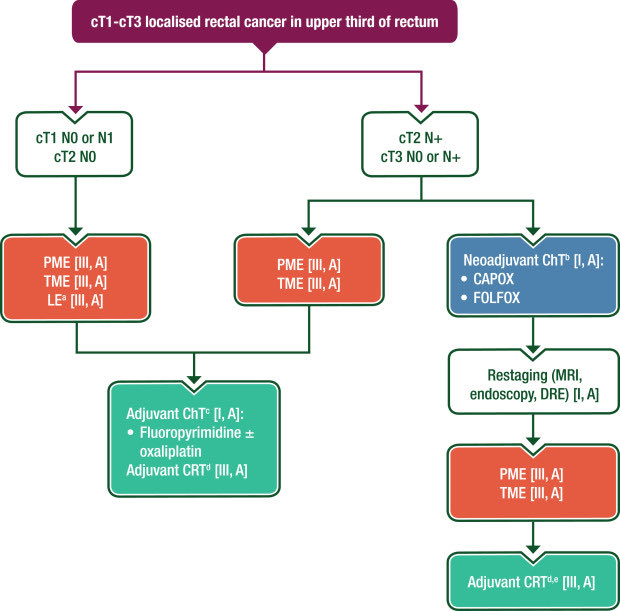
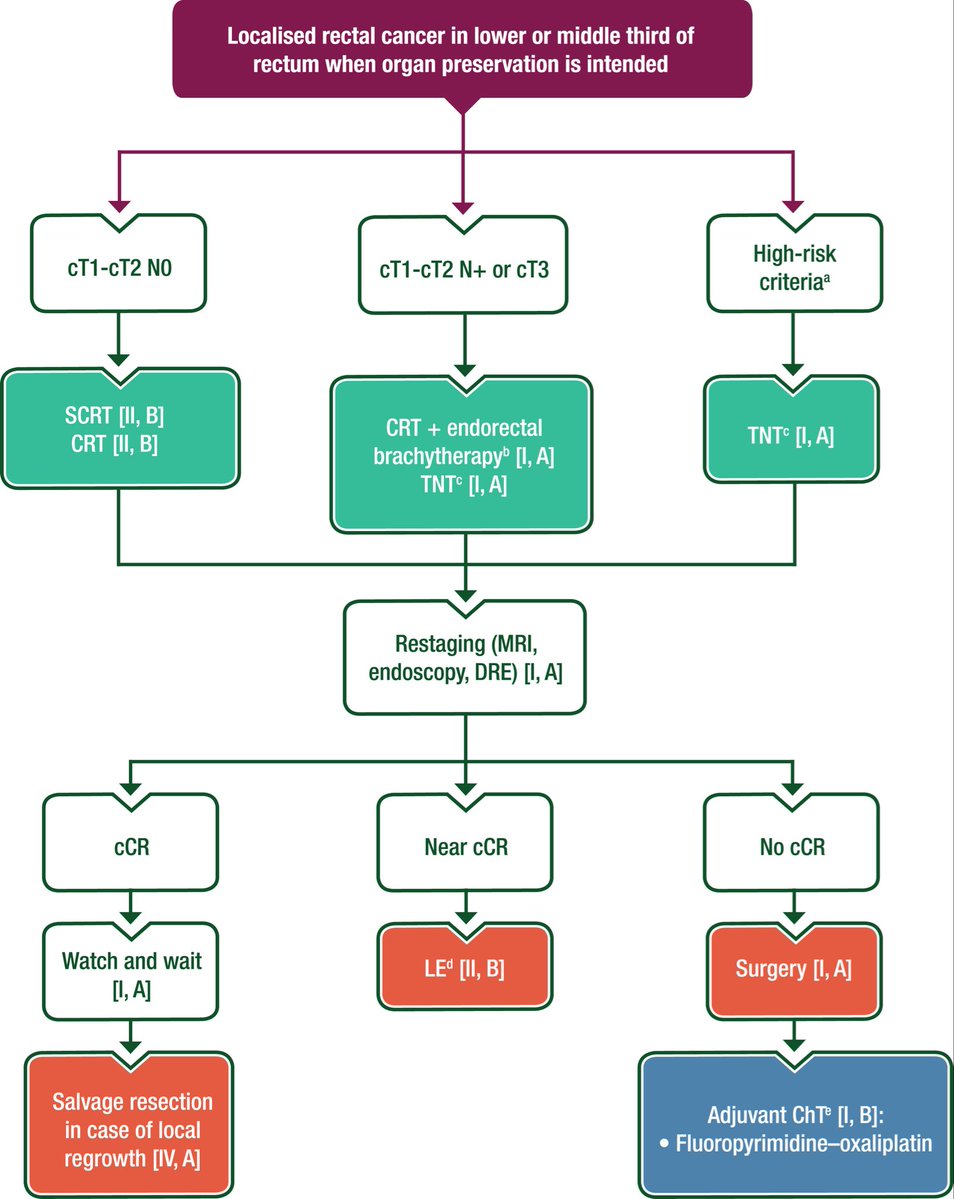
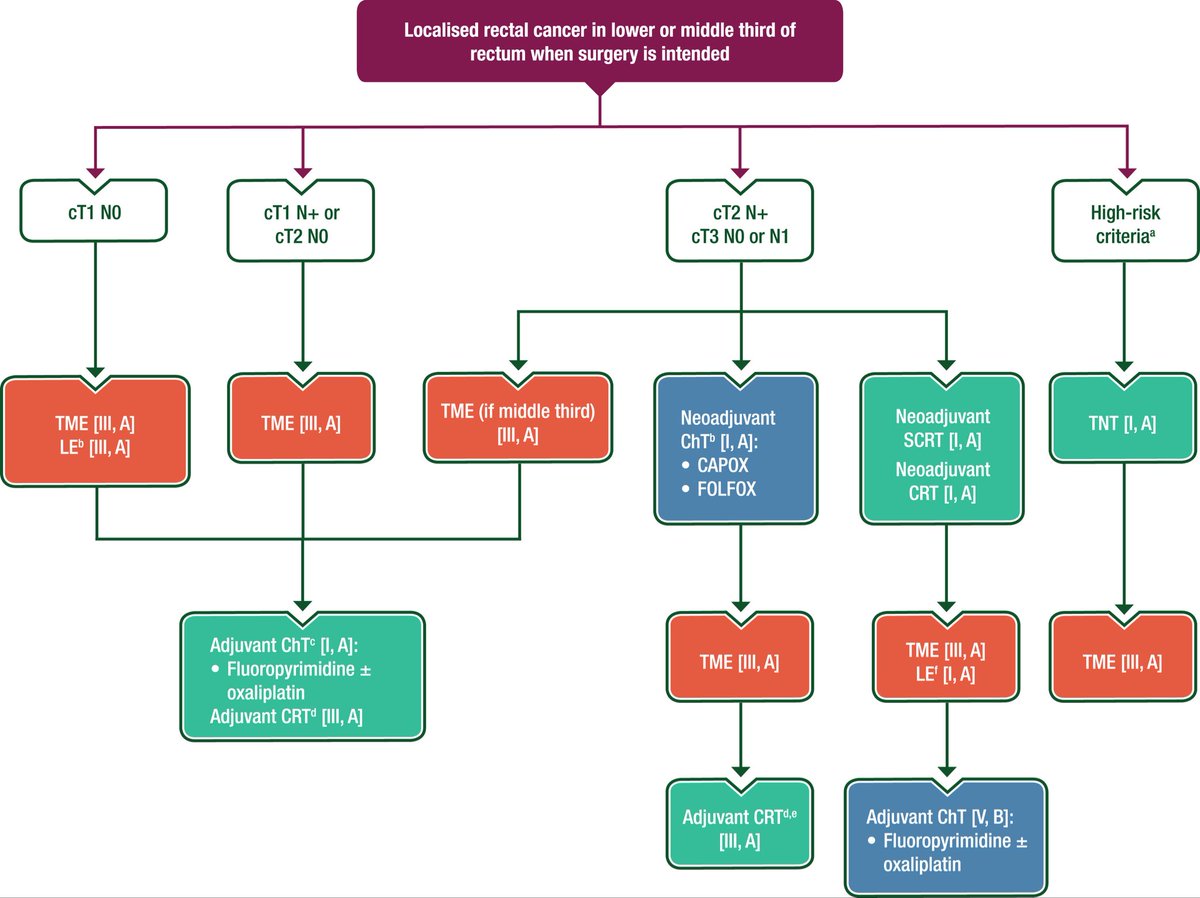
💥 It’s here! The new ESMO Clinical Practice Guidelines for localized rectal cancer (@Annals_Oncology)
🔗 https://t.co/cdCezBb6G7
📌 Covers:
•Imaging & diagnosis
•Staging & risk assessment
•Treatment & follow-up
•Algorithms for local & LA disease
When it comes to rectal cancer, guidance just got…straight to the point 🎯
@OncoAlert #OncoAlertAF @OncoReporte@myESMO@seom@GrupoTTD
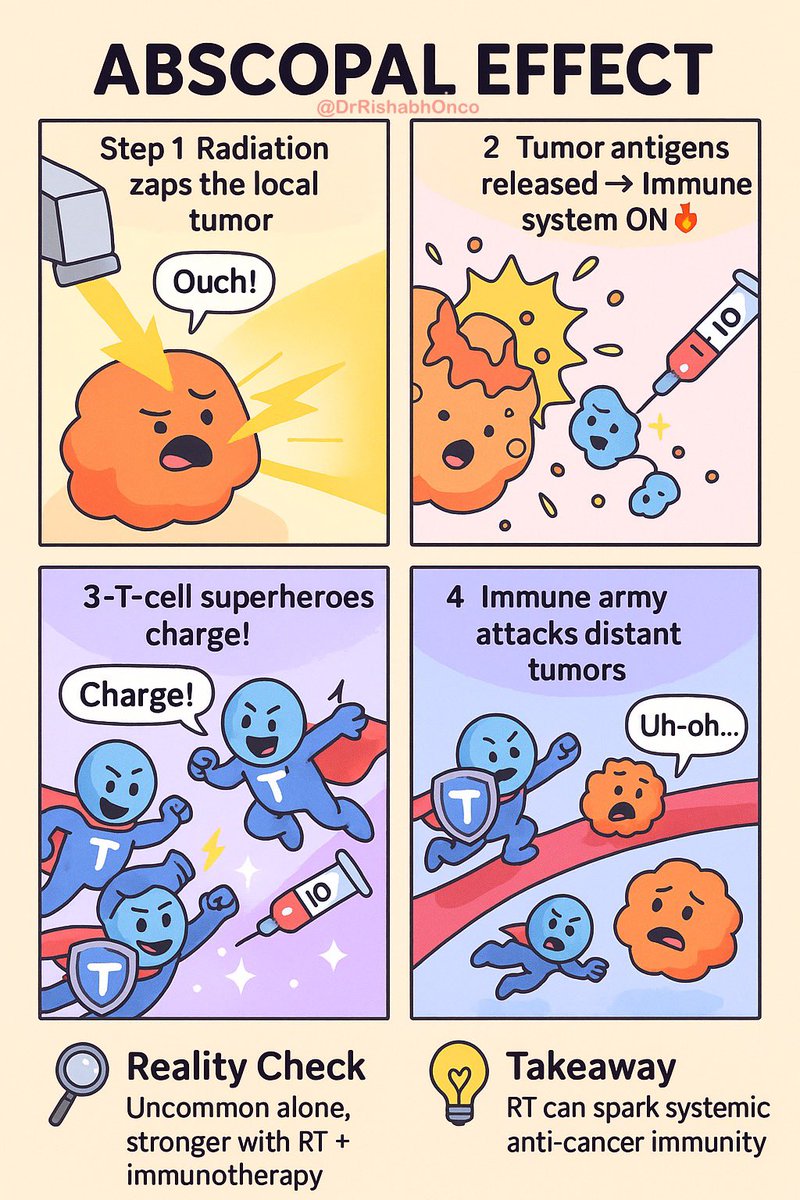
🌟 The Abscopal Effect : When local radiation has systemic impact ✨
👥 What is it?
Radiation to a single tumor site → unexpected regression of distant, non-irradiated tumors.
⚙️ How does it work?
• 🔥 Radiation kills cancer cells → releases tumor antigens
• 🛡️ Immune system gets activated → T-cells attack metastases elsewhere
• 💉 Often boosted with immunotherapy (RT + ICI combos)
📊 Reality check
Rare in clinic, but growing evidence with IO combinations.
💡 Takeaway
Radiation = not just local control… it can spark systemic anti-tumor immunity.
👉 Turning the body into its own “vaccine factory.”
#OncoTwitter #RadOnc #medtwitter #ImmunoOncology
@OncoAlert@astro@asco@myesmo