On average, someone in the U.S. dies of a stroke every 3 minutes and 14 seconds. If there is a history of A.Fib, please address the left atrial appendage at the time of cardiac surgery!
The Brockenbrough-Braunwald-Morrow sign.
This sign is characterized by a ⬇️ in arterial pulse pressure after a premature ventricular contraction, accompanied by a significant ⬆️ in peak left ventricular systolic pressure.
Severe constrictive pericarditis. Starting CVP was 25mmHg, CI was 1.77 L/min/m2 and PAP was 51/20. Following near total pericardiectomy CVP dropped to 10 mmHg, CI improved 3.2 L/min/m2, PAP 34/20. @KrithikaRamapr1
@LuisCastroMD@tomcnguyen@JoChikweMD@M_Pompeu_Sa_MD@ovidiogarciav Nice result. In our experience, adequate septal myectomy is usually sufficient to relieve both the dynamic outflow tract obstruction and abolish SAM without the need of mitral valve repair…unless there is an intrinsic mitral valve problem.
It is not uncommon to see a partial or complete LBBB after myectomy. Watch out for a pre-existing RBBB as this carries increased risk of requiring PPM after myectomy.
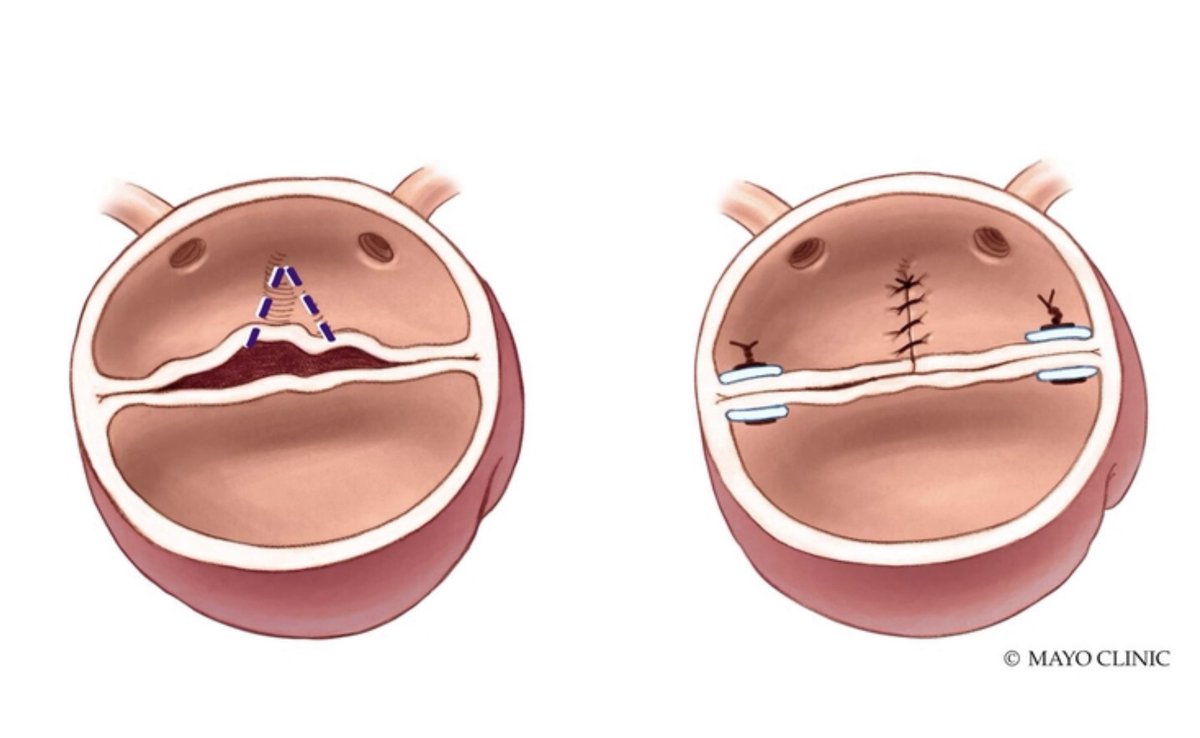
The asterisks indicates the initial site of myectomy (nadir of the RCC…it is then carried CCW to the AMVL).
When should you advise surgical myectomy for HCM?
1. Effort induced symptoms are unresponsive to medical Rx (beta blockers, calcium channel blockers, disopyramide).
2. Patient is intolerant to medicine (meds make them feel worse).
Severe mitral annular calcification.
How do you manage this when performing MVR?
Debridement with or without patch? Suture around the calcium bar? Suture into the leaflet? Suture to left atrium?
Whatever you can to get a good valve in with no perileak.
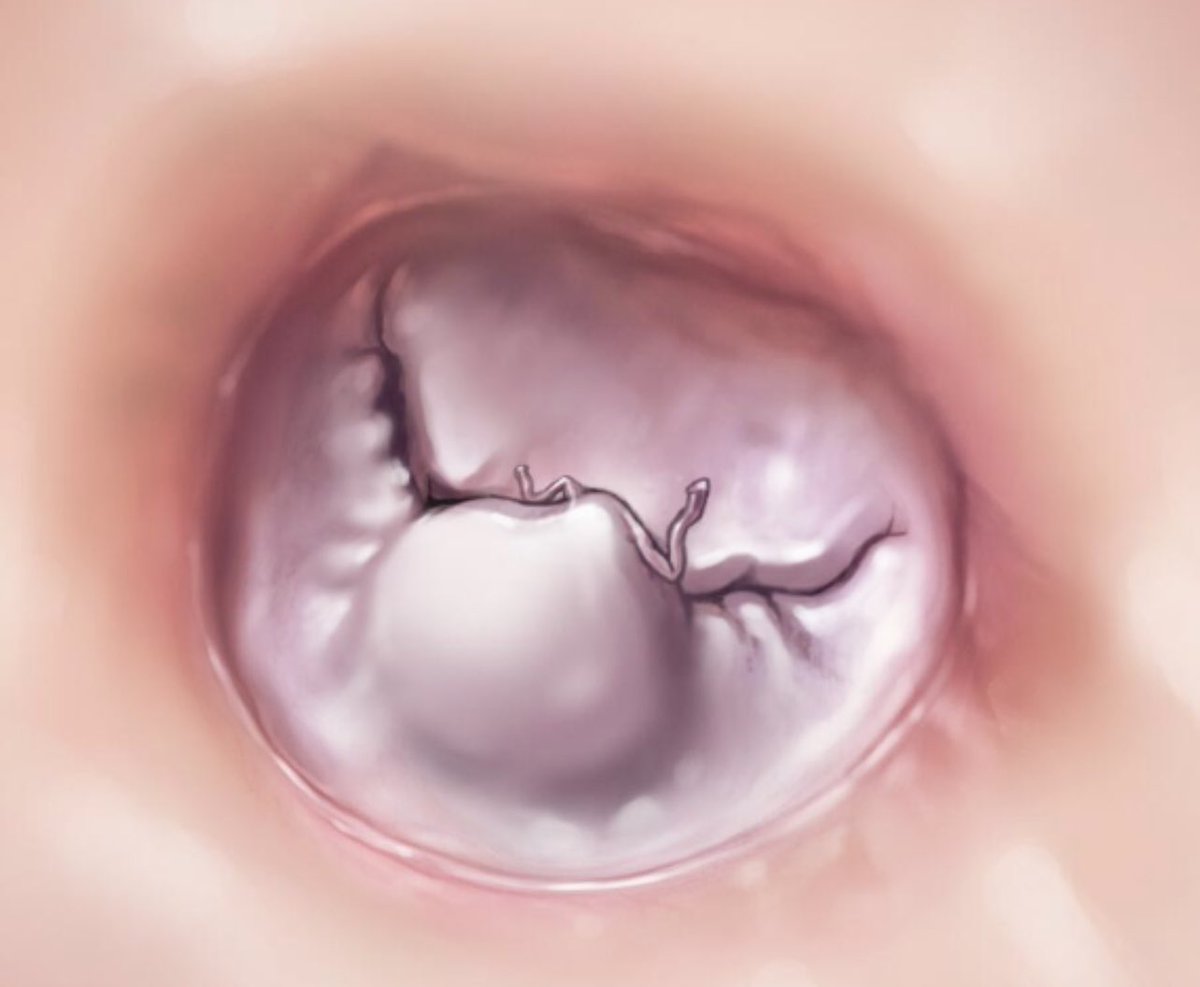
Aortic valve regurgitation repair in a Bicuspid valve.
Plicate (or limited resection) to eliminate conjoined cusp redundancy, close the sub-commissural triangles (5 0 Ethibond with Teflon pledgets) and resuspend the commissures.