@LisaBritton I'm going to take the positive approach. Millennial /young genx parents are a lot more involved and empathetic with their kids than previous generations? this may be helpful?
WHY OUR HOSPITAL CRISIS IS REALLY A SENIORS CARE CRISIS
Richard, you raise a very important point and have sparked the policy geek in me.
There once was a balance between for-profit, non-profit, and public care for seniors, and that balance needs to be restored.
A few realities about long-term care, assisted living, and seniors care are worth considering.
Cost + profit = higher price.
1. For-profit providers must cover infrastructure, equipment, staffing, and profit, which raises the cost of care.
Many therefore focus on lower-needs residents, since higher-needs, lower-income seniors are harder to support in a profit model.
2. Staffing pressures can arise when operators reduce costs using fewer, lower-paid, or less-skilled staff while charging residents additional fees.
3. A phenomenon sometimes called “Eviction by 911.”
When residents’ needs increase, they are transferred to hospital by ambulance. In some cases the facility continues to hold the publicly funded bed while the patient becomes an Alternate Level of Care (ALC) patient occupying an acute care bed.
4. This contributes to hospital congestion and can mean taxpayers are effectively paying twice.
Government should audit every ALC patient in acute care to determine if this is occurring.
5. Policy balance matters. For-profit providers have a role for lower-needs, higher-income residents, but PUBLIC and NON-PROFIT care must remain the BACKBONE for seniors with higher medical needs.
6. Funding incentives are misaligned. Long-term care is funded per occupied bed, while hospitals absorb the cost of all admitted patients, including ALC patients.
7. When residents are transferred but their LTC bed remains funded, pressure shifts to acute care, contributing to surgery cancellations and the ER/EMS crisis we see today.
8. Premier @ABDanielleSmith and others often criticize AHS, but government sets these policies and AHS does not control hospital inflow or outflow.
9. Regulatory barriers also play a role. Many assisted living and LTC facilities cannot provide higher-acuity services such as IV antibiotics, oxygen therapy, or complex monitoring, even when these could safely be delivered outside hospital.
10. For example, a long-term care resident with osteomyelitis (bone infection) may require 4–6 weeks in hospital simply because the facility cannot administer IV antibiotics.
11. We should enable higher levels of care in assisted living, LTC and home care, including:
– 24/7 RN coverage
– Nurse practitioners on call
– Integration with family physicians and primary care network multi-disciplinary teams
– Mobile lab, x-ray and low acuity EMS support services
***This simple and inexpensive policy change can make a very big difference in the ER crisis we face today, reduce suffering AND save money***
12. Sending frail seniors to acute hospitals for relatively low-acuity problems makes little sense. Hospitals are the most expensive and often the least appropriate setting for these patients.
13. The old auxiliary hospital model addressed this gap better than our current system.
14. Intermediate and convalescent facilities (transition, subacute, rehab) once cared for patients needing more support than home but not full acute hospital care.
15. Seniors care now increasingly includes for-profit home care and private seniors housing. These services can play a role, but when profit incentives dominate system design, access and care levels can become uneven, especially for seniors with complex needs.
16. Many jurisdictions are moving toward a HOME FIRST MODEL, supporting seniors to remain safely at home with adequate home care and caregiver support before institutional care. Denmark does this well.
17. Properly funded home care is far less expensive than hospital or institutional care and often better for patients and families. When home care is inadequate, families are forced to rely on emergency departments and hospitals.
These low-cost initiatives improve system flow.
When seniors who no longer require hospital care remain in acute beds, admissions are blocked, emergency departments congest, and the ER/EMS crisis worsens.
My ICU doctor friends are discharging patients to their living rooms from the ICU as the step-down beds are occupied by ALC patients!
profit incentives → LTC transfers → ALC beds → ER crisis
FIX SENIORS CARE & HOME CARE , and you fix a large part of the hospital crisis.
Minister @JasonNixonAB , please address these issues (specifically #11 above) and Minister @MattJonesYYC can run our hospitals safely without resorting to the TLP disaster protocol.
@ABDanielleSmith@nenshi@AdrianaLaGrange@JMeddings@PfParks@NightShiftMD@TheBreakdownAB@cspotweet@ryanjespersen@UCPCaucus@Alberta_UCP@albertaNDP@Albertadoctors@BillKaufmannjrn
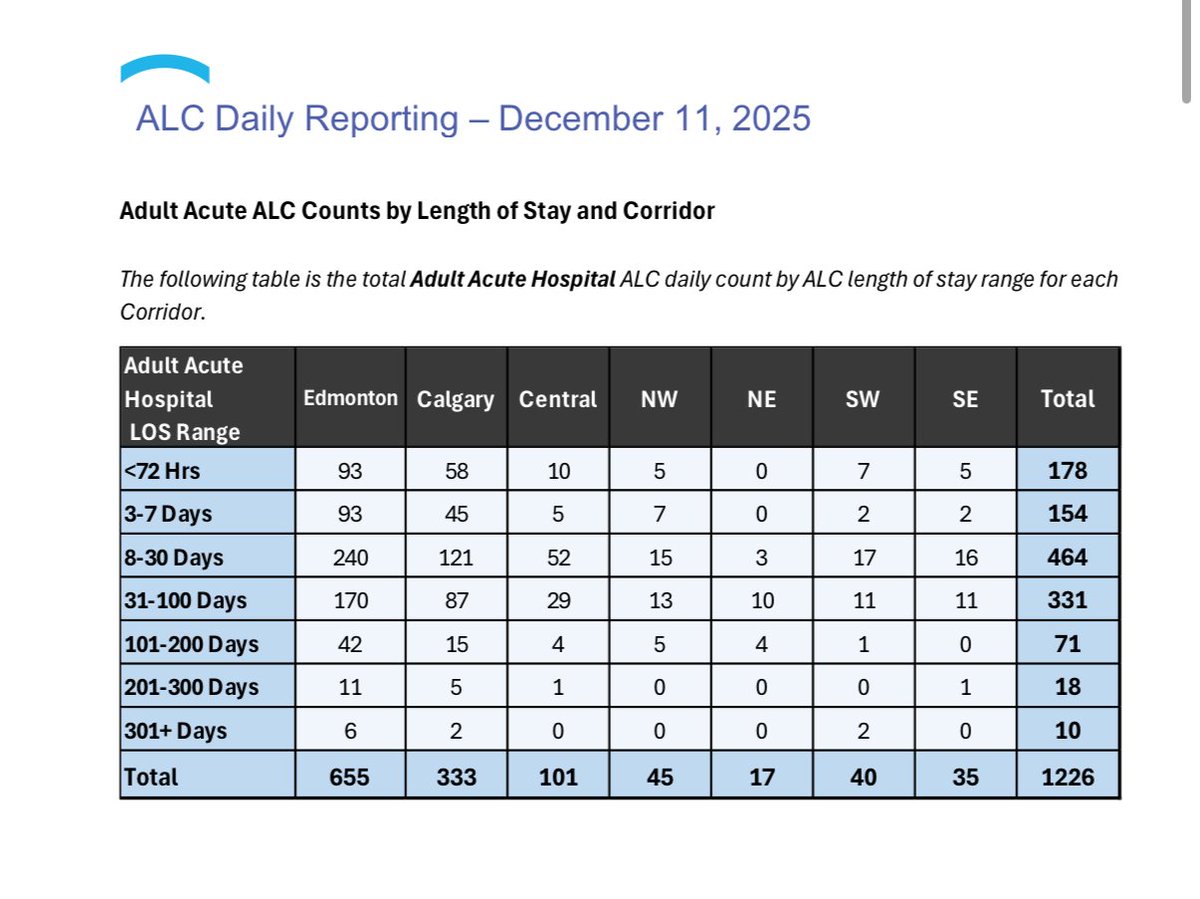
Below is data from August/25 on the left and Dec 11/25 on the right. Note ALC absolute numbers and days in hospital.
@leamaric I'm generally quite understanding with people if it's a once or twice kind of thing. If it becomes a habitual behavioral trait then I start to set more firm boundaries. Obviously if it's a dangerous situation this may change.
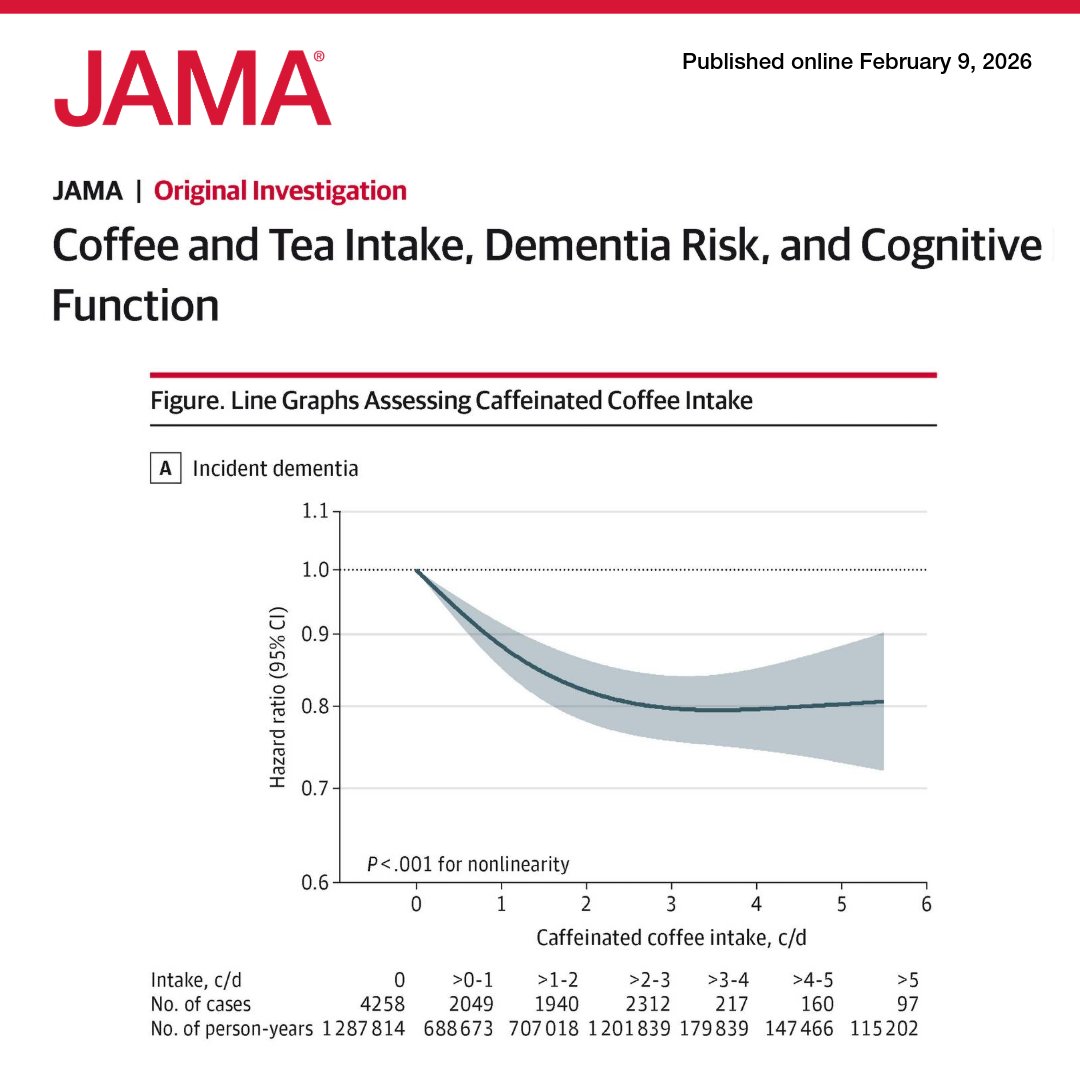
Moderate consumption of caffeinated coffee or tea was linked to reduced #dementia risk and modest improvements in cognitive outcomes; no benefit was seen for decaffeinated coffee in an observational study of US adults.
https://t.co/jlPgjAuosa
@thomaschattwill I think anybody who's ever seen the Station nightclub fire video would immediately run out of there the moment they saw those flames. Or maybe I expect too much of humanity. Insanity
Callie, that is an understatement,
Please tell me where I am wrong, but I’m thinking that holding ALC seniors on acute wards for weeks or months isn’t just unethical, it’s INHUMANE and COSTLY.
We do it only because the system has failed to provide alternatives. What actually happens to ALC seniors in hospital:
-Rapid physical and cognitive de-conditioning
-Loss of mobility, continence, swallowing, and nutrition
-Sedation/antipsychotics -> delirium
-Falls, fractures, head injuries
-Blood thinners -> major bleeding
-Pressure ulcers (often to bone; About $60,000 per wound)
-Hospital-acquired & drug-resistant infections
-Sleep deprivation, sensory deprivation, depression
-Acute deterioration -> ICU admission
-Loss of independence -> permanent institutionalization
-Family/spousal collapse (depression, illness, burnout)
-Unnecessary suffering and death
-Massive cost to taxpayers
Then there are the Downstream system effects:
-ALC bed block cancels surgeries
-ER overcrowding (caused by EIP's) and ambulance off-load delays
-Staff moral injury, burnout, and turnover
-Longer waits for everyone, including acute patients
Higher overall healthcare spending for worse outcomes
This is system-induced harm, delivered in the most expensive and least therapeutic setting possible.
So the real question is: Why do governments try to balance budgets on the backs of the most vulnerable, only to drive healthcare costs up and access to care down?
ALC is a medical, ethical, and fiscal emergency. We need safe, humane, rapid alternatives, now, not more reports.
@UnitedNurses@DanielleLarivee@poliadamyyc@thatABnurse@NatePike
@alandrummond2@nationalpost I'm a family doctor who also does emergency shifts in our local hospital. I see this situation at least once a month. Usually I can find some way to make sure they get appropriate follow-up but it is not a replacement for a comprehensive family doctor. That is what is needed.