If you would like to help me keep my n*wsletter alive, you can take out a paid subscription. I have a couple of months to make it work before I give up and go get a normie job. The EC seems to have twatted my prospects in my field. One of the avenues of legal redress would have involved establishing that, but that seems like it's over now.
Read/share/like/subscribe/support for fresh hot takes on sex, free speech and genderfaff in Europe.
@HSELive@AnneOConnorIRL I want to see why Irish government bodies, overseen by @MichealMartinTD are doubling down rather than looking at the evidence surfacing all over the world [as well as here in Ireland] that telling children they are born in the wrong body is a dangerous lie.
I'm a cardiologist. A 42-year-old mother of two came to my office complaining of jaw pain and crushing fatigue. She ran half-marathons. Her EKG was normal. Another doctor had sent her home with anxiety medication.
When I got her into the cath lab, I found severe microvascular disease — plaque choking the tiniest vessels of her heart, the ones standard angiograms routinely miss.
Her heart had been starving in silence while everyone told her she was stressed.
She is alive today. Too many women like her are not.
Heart disease kills more women than every cancer combined. And medicine is still diagnosing it through a male lens.
84% of cardiologists report having patients in the past year whose heart disease was misdiagnosed by another physician. Women with a STEMI heart attack have a 59% greater chance of being misdiagnosed compared to men. Women with an NSTEMI — 41% greater chance.
The reason is structural. For decades, we screened, tested, and treated women using a template built for men.
Men's heart attacks announce themselves — the crushing chest pain, the clutched fist, the Hollywood collapse. Women's hearts whisper. Crushing fatigue that feels like wearing a lead vest. Jaw pain written off as TMJ. Nausea blamed on a stomach bug. An ache between the shoulder blades blamed on a long week. Shortness of breath blamed on being out of shape.
For years, medicine called these "atypical" symptoms. They are not atypical. They are female-typical. Half of humanity is not a variant.
And the biology runs deeper than symptoms.
Women have smaller hearts and narrower coronary arteries. Plaque doesn't only clog the big highway vessels — it hides in the microvasculature, the tiny branches feeding the heart muscle itself. A woman can have a heart attack with a completely "clean" standard angiogram.
SCAD — spontaneous coronary artery dissection — occurs 90% of the time in women. Often young, fit women with zero traditional risk factors. It's the leading cause of heart attack in women under 50, accounting for roughly one quarter of all cases in that age group. Most doctors have never diagnosed one.
And some of the most dangerous cardiac risk factors are hidden in women's medical histories where no one thinks to look:
Preeclampsia or gestational hypertension doubles to quadruples lifetime heart disease and stroke risk. Pregnancy is the body's first cardiac stress test — and these complications are early warning sirens, not closed chapters.
Autoimmune disease — lupus, rheumatoid arthritis, psoriasis — far more common in women, turbocharges inflammation and plaque formation at any age.
Cardiovascular disease in women aged 20-44 is projected to surge nearly 50% by 2050.
The youngest patients in my practice keep getting younger.
What every woman should ask her doctor — and what every doctor should be asking:
"Given my pregnancy history, autoimmune status, and family history — what is my full cardiovascular risk?" If they don't ask about preeclampsia or gestational diabetes, volunteer it.
"Should I have an Lp(a) test and a coronary calcium score?" Standard cholesterol panels miss too much. Lp(a) is genetic, one-time, and most women have never been tested.
"My tests came back normal but my symptoms haven't stopped — what's next?" Normal stress tests and angiograms can miss microvascular disease, spasm, and SCAD. Persistent symptoms warrant coronary CT angiography or cardiac MRI.
And if something feels wrong — say these exact words to your doctor: "I am concerned this could be my heart."
That single sentence changes the workup. Do not soften it. Do not apologize for it.
80% of heart disease is preventable. But the playbook has to be built for female biology.
Two decades ago, I wrote one of the first books warning that heart disease was the number one killer of women and that medicine was diagnosing it through a male lens. It was recognized by First Lady Laura Bush at the White House during the early years of the national conversation about women's heart health.
I'm haunted by how much of that book I could republish today unchanged.
The science has advanced. The awareness has grown. But the gap between what we know and what happens in the exam room is still costing women their lives.
Share this with every woman you love — and every doctor who treats them. READ MORE: https://t.co/4LRugiY8q2
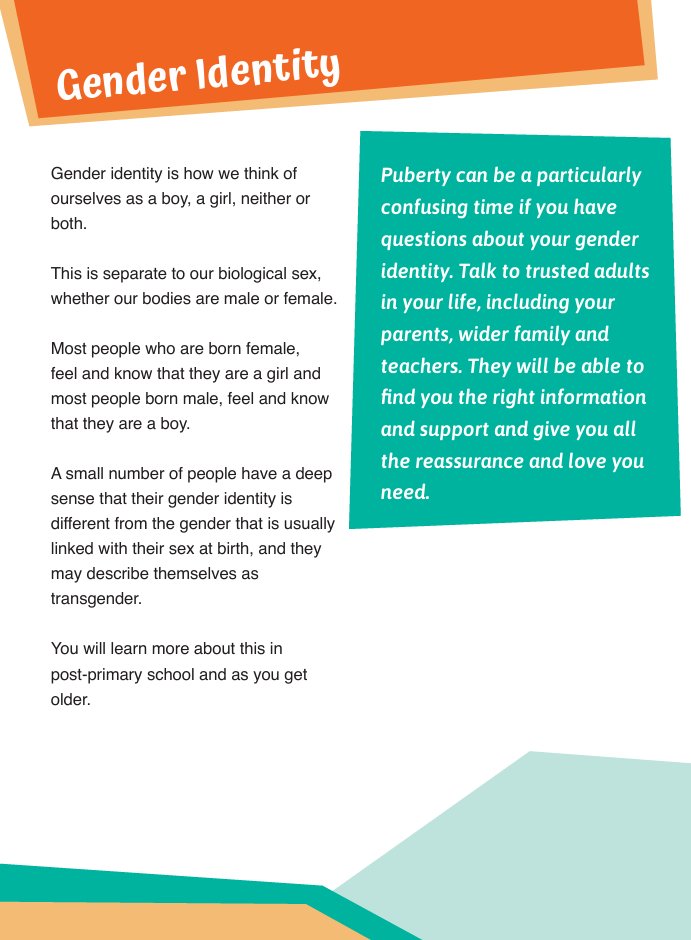
I have found yet ANOTHER copy of the busy bodies guide for primary schools
It seems @HSELive have iterated the gender identity page of busy bodies 3 times, 2020, 2023, 2026
3 versions below, the reason it keeps changing is they are making this nonsense up @AnneOConnorIRL
I’m going to share the proof that state funded activists belongto have infiltrated @HSELive puberty guide ‘busy bodies’ which is shared with every primary school in the country and filled it with transgender ideology
@AnneOConnorIRL the new CEO has to intervene
Thread
I’ve had enough of this. They think we’re not watching, the mission to erase women and girls continues
The @HSELive under @BernardGloster has removed ‘girls’ from the busy bodies guide in favour of ‘people’ I will share more before and after samples in a thread.
the CEO of Childrens books Ireland knows exactly what she is doing, this is her committing to exclude inappropriate books in the reading list in 2023 @rte@griptmedia
but she continues. The focus needs to shift now onto @KidsBooksIrel They are still pushing trans at toddlers
Seeing as there is a lot of focus on @NormaFoleyTD1 I would like to highlight that I have been emailing & ringing her office about what is happening in Irish schools in regards to inappropriate content targeting children on her watch for 5 years.
Never a response.
Montenegro, and all the other Balkan states, are being blackmailed: replace sex with "inner gender identity", or you cannot join the EU.
In other words: betray women and girls (and reality)
I was extremely disappointed by the @PresidentIRL choosing to endorse the medical transition of children and I wrote this for the @IrishCathNews in the hope that it might convince her advisers to research this issue- they’ll reconsider this decision very swiftly if they do
Those who say the sex and gender debate is about “a tiny minority” are looking through the wrong end of the telescope.
It’s about a concerted attempt by activists, backed by governments, institutions, and NGOs, to deny that humans - like all other mammals - are either male or female. It’s about an attack on reality.
If you can get someone to believe a man can be a woman, you can get them to believe anything.
If people are threatened. fired, taken to court and convicted for pointing out that a man is a man, or that it is impossible to change sex, freedom of speech is lost and you are living under a tyrannical dystopia.
It’s not about “a tiny minority.”
It’s about all of us.
1./ My latest article explores the truth behind an incredible scandal. 3 days ago the UK government announced it will host a huge jamboree for the LGBTQ+ lobby next year. As if that's not bad enough it will also hand over £21M to insane LGBTQ+ organisations. What's going on? 👉
The WHO trans healthcare guidelines are coming and they will be bad
One of the objectives of trans activism has been to get trans-ness depathologised. Meaning, to have it taken out of the official category of mental illness.
There’s a problem, however: how can you ask the state to pay for your healthcare (breast implants or amputations, for example) for something that is not a disease or a mental illness? The solution that the drafters of the World Health Organisation’s almanac, the ICD, was to reclassify wrong-bodyism as “conditions related to sexual health”.
But reclassifying something means you also need new guidelines to go along with it. How should this very-much-not-a-mental-illness be treated by doctors and shrinks? How do we justify the coverage of cures for people who definitely-do-not-need-to-be-cured-of -anything? What a conundrum.
The task of drawing up the new WHO guidelines got underway in 2023ish, and when the names of the people who would draft it went public, TERFs went bananas because all the people in the Guideline Development Group seemed to be ideologues. They are not just on the trans train, they’re driving it. They’re in the engine room shovelling buckets of black coal into its furnace.
Anyway, one of the external experts was a very pervy Canadian autogynephile called Florence Ashley. He quit the group after the uproar, and in the months that followed, various gender critical/evidence-based medicine and TERFy type groups made statements about the crazies who were still in it. Nothing has been announced publicly since then.
This systematic review from May 2025 seems to claim that the group has decided on 15 “outcomes of interest”, with the help of WHO technical experts.
The outcomes are based on “patient importance” so I think we can safely predict where all this is going. Later last year, someone from ILGA-Europe reportedly said that clinics don’t have to wait for the guidelines to get busy transitioning their patients. Indeed, as I wrote for Genspect, trans ‘affirming’ care is a blossoming industry; the real value of the WHO guide, whenever it gets here, will be comms that will help feed lobbyists arguing for public reimbursement of medical transition.
The WHO has cachet, so you can imagine the headlines to come. This is the trans activists’ version of the Cass Report.
See the recent list of drafters in the WHO trans guideline group, link below
Hi @PresidentIRL, below is an article I wrote about BelongTo and my first hand experience after spending almost two years there as a vulnerable and confused teenager.
If you value LGB young people, you simply will not endorse this organisation.
I wish our @PresidentIRL didn’t support the sterilisation of gender non conforming children. But here we are…
State funded, state ordained social experiments and scandal. Children are the guinea pigs
This is the new Wellbeing Curriculum for primary school children. It is being rolled out between now and 2030.
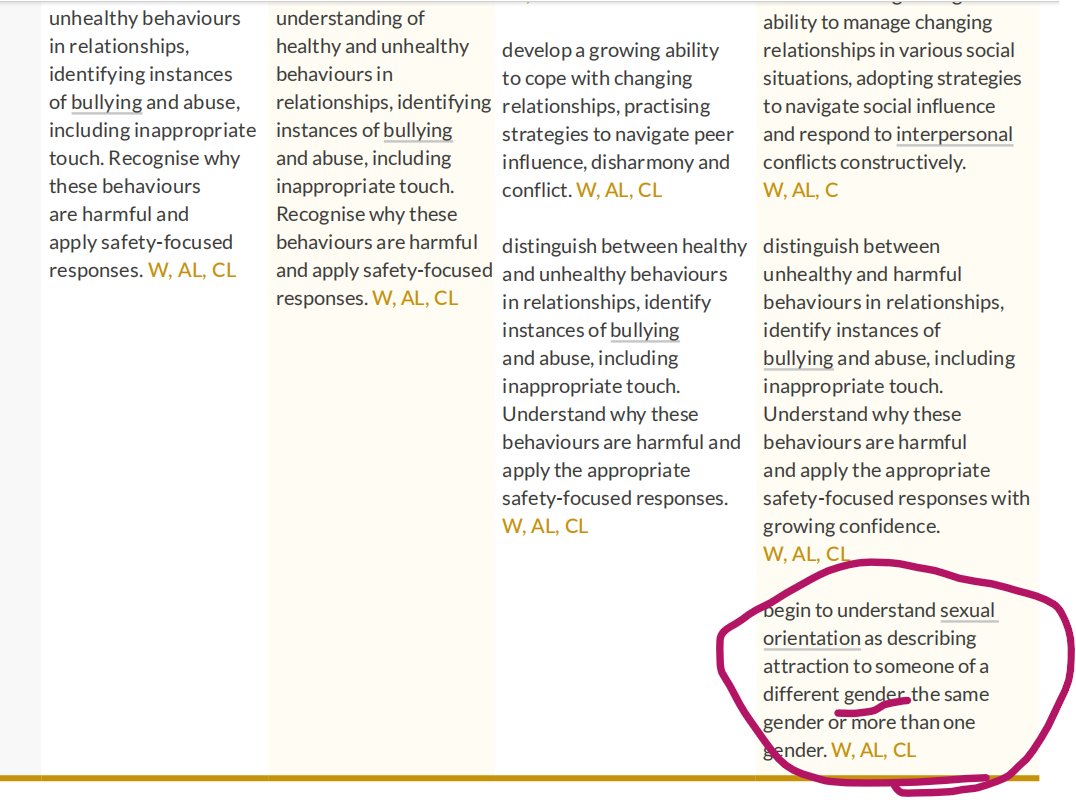
On page 8 they claim they are providing "accurate...information" about sexuality, yet on page 24 they tell children that sexual orientation is "attraction to someone of a different GENDER, the same GENDER or more than one GENDER".
This is gender ideology, not education.
There is nothing accurate about lying to children.
@Education_Ire you ought to be ashamed of yourselves!
Incredibly disappointing to see this. It is galactically inappropriate for the President of Ireland to act as a patron to Belong To, a very well funded lobby group for the medicalisation of children’s identities.
We know these procedures cause harm. Children can’t consent to the loss of sexual functioning and infertility because they don’t understand the consequences of this. This is an unfolding medical scandal.
Mo náire thú, a Uachtaráin
Today, the European Commission adopted a Communication responding to the European Citizens' Initiative (ECI) ‘Ban on conversion practices in the European Union'.
We were relieved that the Commission stopped short of pursuing an EU-wide ban and will not seek to add conversion practices to the list of EU crimes under Article 83(1) TFEU. However, it plans to issue a non-binding recommendation next year urging states to introduce bans on so-called conversion practices, while continuing to mobilise its enormous resources and soft-power machinery to pressure governments into adopting such legislation.
Gender identity has thoroughly captured the EU. The range of actions announced today is aimed at consolidating far-reaching regimes in some Member States, nudging reluctant ones off the fence, and laying the groundwork for the next political turn in resistant states and EU candidate countries.
Broad opposition is growing across Europe, led by feminists, lesbian and gay rights organisations, parent groups, and an increasing number of clinicians and therapists raising concerns about the risks involved. Yet these voices are systematically excluded from the EU’s internal discussions.
Bans on so-called “conversion practices” are deceptively framed. They invoke the brutal abuse once inflicted on lesbians and gay men, while applying that historical imagery to something fundamentally different. Framed around gender identity and expression, these bans risk harming the very people they claim to protect - particularly gender non-conforming children who may simply grow up to be lesbian, gay, or bisexual.
Such bans entrench the unscientific belief that some children are “born in the wrong body” and should be placed on a path toward irreversible medicalisation. In practice, they make affirmation of a child’s self-declared gender identity a legal requirement not only for therapists, but for teachers, doctors, and even families.
Making affirmation the only permissible approach to a child’s self declared gender identity is not protection. Young people struggling with their sex require open, exploratory and therapeutic support; their families deserve evidence-based care; and society needs honesty and clarity.