@iceman_ex Agreed and its not helped by lack of robust regulation for professions/departments.
I'll speak for physiology, buts it a profession that should be highly regulated given how easily an echo can be misreported/a CIED van be reprogrammed incorrectly yet our register is voluntary.
Cardiac arrest isn’t a diagnosis in the same way as headache isn’t a diagnosis, jaundice isn’t a diagnosis, chest pain isn’t a diagnosis, abdo pain isn’t a diagnosis. If we keep trying to find magic bullets that treat the presenting complaint, we’re relying on luck to innovate.
The European Resuscitation Council Guidelines 2025 are out now in Resuscitation!
🔗 Read the Executive Summary: https://t.co/QWoGv3nVgd
🧵 Explore all the chapters in this thread
#Resuscitation#RESUS25#ERCGuidelines#Guidelines2025
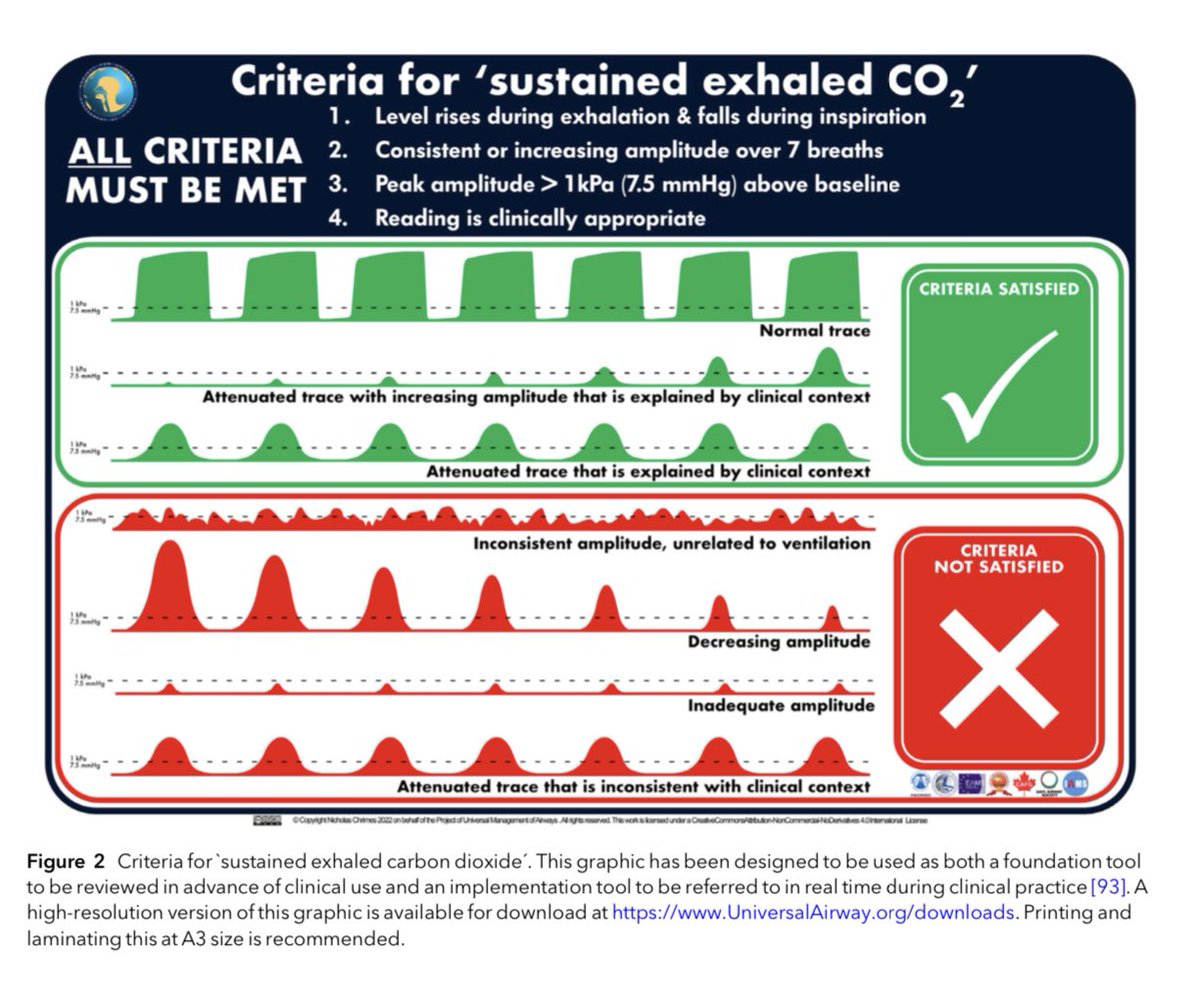
Avoiding unrecognised oesophageal intubation
The @RCoA & @dasairway have agreed to drop ‘no trace wrong place’
The message now is that we need to exclude oesophageal intubation by identifying SUSTAINED EXHALED CO2
This requires 4 elements
-CO2 rises & falls with respiration
-sustained (non-fading, >7 cycles)
-amplitude >1 KPa
-clinically appropriate
It replaces ‘no trace wrong place’ which is insufficient & therefore inadequate
See these two updated webpages
Sustained exhaled CO2
https://t.co/ZAdO23sHil
Prevention of future deaths
https://t.co/goxZZEcCzu
@AAGBI@AndyHiggsGAA@NicholasChrimes
@samdharrison@stjohn_wa You'll be missed in London. Thank you Sam for all your wisdom and jokes over the years!
You've defo provided me with peace on jobs when I heard/saw you were my allocated backup.
Fyi - think they read the ECGs upside down in Australia 😜
1/
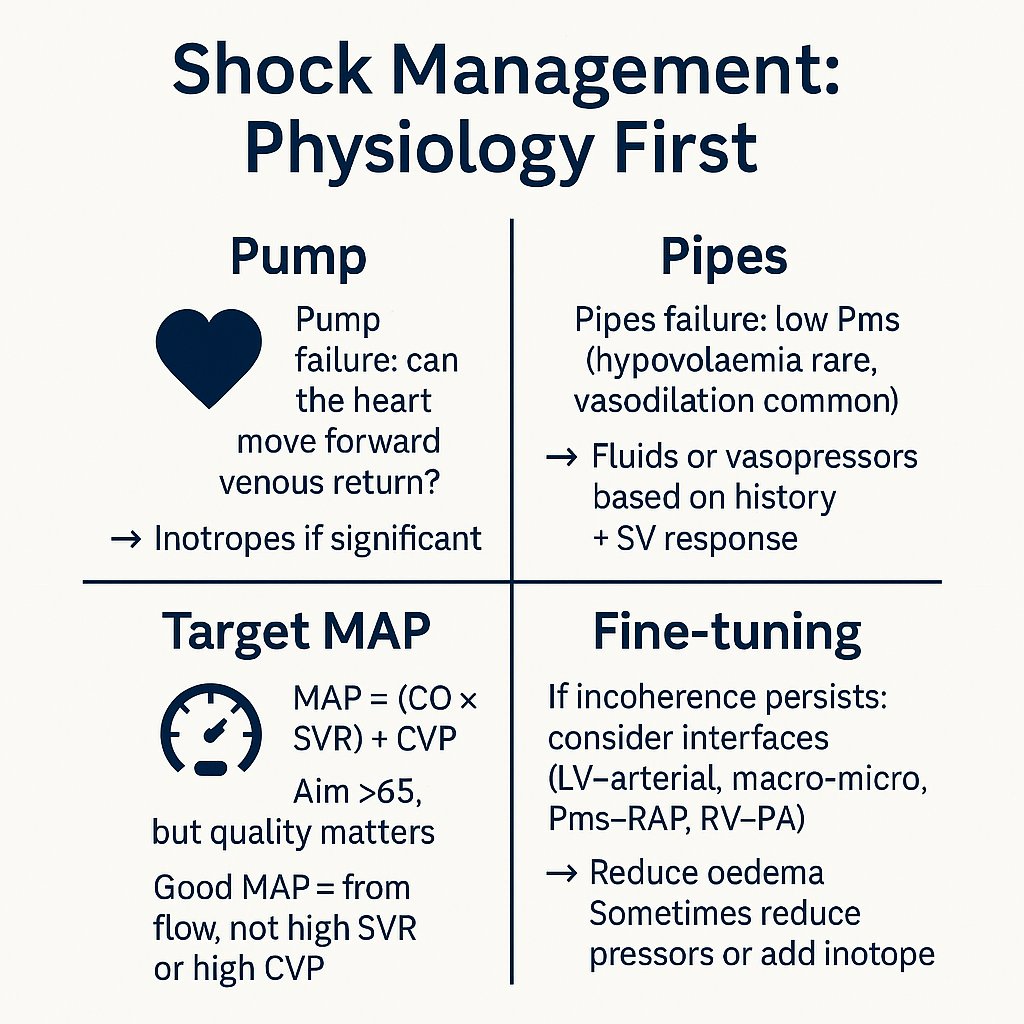
Shock isn’t “give fluids, then pressors, then inotropes.”
That recipe misses the physiology.
Here’s how to manage shock properly: 🧵
#MedX#haemodynamics
(0/x) How do I approach the first 2 minutes of meeting a new critically ill pt?
My approach has been forged from my learnings as a paramedic.
Here's my approach as an ICU doc 🧵
Fresh from the edit - our podcast on #SPEAR and advanced resuscitation . @TheResusRoom have done a brilliant job assembling this - concept, delivery & insights from our OHCA programme at @EastAngliAirAmb and beyond… https://t.co/4Qe9GcYKkW @BartsIntervGrp@NHSBartsHealth
Many see pre-procedural checklists solely as a tool for checking equipment
In EMRS we monitored the heart rate of clinicians during our pre-anaesthetic checklist. 100% of clinicians experienced a fall in heart rate
Here's why....
https://t.co/NTkBbI2OoO
🧵Why does low protein intake cause hyponatraemia?
Most people find this confusing.
But the underlying physiology is beautifully simple.
Let’s walk through it 👇
#Hyponatraemia#FluidBalance#MedTwitter#FOAMed
Half of the places for the AHP Annual Conference have already been taken! Don’t miss your chance to attend one of the UK’s biggest events for cath lab professionals.
🗓️ 7–8 July | 📍 Park Plaza, Leeds
🎓 Two learning streams – Core & Advanced
🛠️ Hands-on sessions, expert speakers & team-focused learning
💼 Free for BCIS members – bursaries available for accommodation
🔗https://t.co/Cjbonxw2RJ
@bcis_ahp
@wmcareteam RIP Charlie, you were an inspiration and welcoming face to so many. So many young people were inspired by you. You were a great clinician and we were so proud of you when you became a Dr! Never forgotten, you'll always be remembered
Use of transoesophageal echocardiography in the pre-hospital setting to determine compression position in out of hospital cardiac arrest - Resuscitation https://t.co/viI6xBa8uc
And some supporting papers, for some extra reading! https://t.co/oWaZq7jl3P and https://t.co/a3b3y1m27W and https://t.co/nGJmFZDt7I @EAAARAID@BartsIntervGrp