We’re excited to welcome you this Friday, May 15, from 12PM–6PM for the 2026 Mount Sinai Fuster Heart Research Forum, where faculty and trainees from across the institution will showcase their outstanding scientific work!
@DLBHATTMD@SwirskiLab@MountSinaiHeart@IcahnMountSinai
Valentin Fuster, MD, PhD, has been honored with the Glorney-Raisbeck Award from the New York Academy of Medicine in recognition of his exceptional contributions to cardiovascular medicine.
Join him on Monday, June 1, for his Glorney-Raisbeck Lecture, “Evolving New Imaging for Primary and Primordial Prevention – PESA, PRECAD, REACT, PESA-Brain & SHE Studies,” as he shares insights shaping the future of prevention and cardiovascular care.
Register now: https://t.co/HTCsHROZt2
@MountSinaiHeart
Mount Sinai was proud to support the ACC Cardiology Hour at #ACC26. Led by Valentin Fuster, MD, PhD, MACC, a multidisciplinary panel of experts explored the most practice-relevant science from ACC 2026 and its impact on real-world patient care, highlighting key clinical decisions cardiologists face every day. Watch the episode here: https://t.co/wdODgs3h2H
@ACCinTouch@MountSinaiHeart #CardioX #Cardiology
When I became CEO of DocGo, I set a simple expectation: trust has to sit at the center of everything we do—from the care our clinicians deliver to how we safeguard the sensitive information our partners and patients share with us.
Today, I’m proud to share that DocGo has been recognized as one of the 2026 World’s Most Ethical Companies® by Ethisphere. It’s our first time receiving this honor, and it’s a meaningful validation of the standards our team has built—and the culture they live every day.
Ethics isn’t a statement on a wall. It’s governance, accountability, and the willingness to speak up, especially when it’s hard. I’m grateful to our teams across the company—and to our compliance and risk leaders—for helping ensure that integrity is the easiest path forward.
As we continue to bring technology-enabled healthcare to people where and when they need it, we’ll keep holding ourselves to the highest bar—because in healthcare, trust isn’t optional. It’s everything.
Read more on the press release on our website: https://t.co/cnlca8xprp
#DocGo #WorldsMostEthicalCompanies #Ethisphere #Ethics #Compliance #Governance #Healthcare #Nasdaq #Marketsite
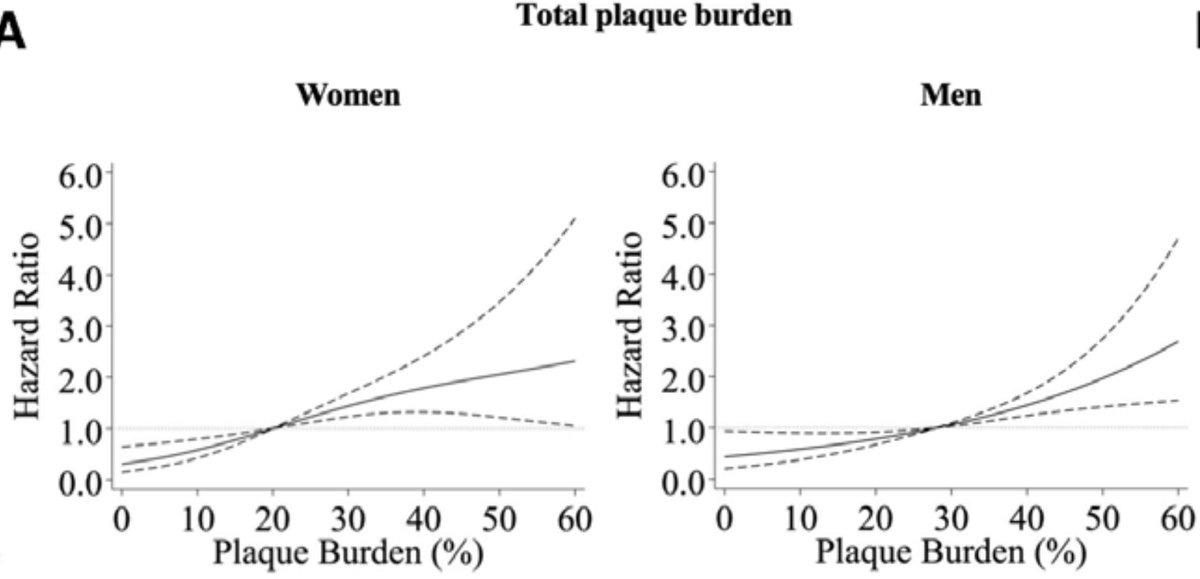
⚠️Women may not need as much coronary plaque as men to get into trouble.
🫀New @CircAHA analysis quantified total plaque burden (plaque volume/vessel volume) in 4267 patients with CP undergoing #CCTA.
Women had less plaque and lower plaque volumes, but risk “turned on” earlier:
Are BVS ready for a rematch with metallic DES in coronary space?
In this review, we walk through the rise, fall, and potential rebirth of BVS—highlighting where early trials failed, why late outcomes matter, and what next gen scaffolds must prove before this rematch.
Outstanding lecture by Dr. Camaj on cardiogenic shock, with a great breakdown of MCS modalities and landmark trials. Highly informative!
Thank you! @acamajmd
I recently had the pleasure of joining Michael Spector on Nasdaq’s Amplify Issuer Spotlight series to discuss how DocGo is leading the proactive healthcare revolution with technology-enabled mobile health services and expanding access to high-quality care to all. Here's a clip from the interview!
Visit Proactive Care Now to watch the full interview and learn about how are team drives real change across the industry. https://t.co/gGEW9Z02hl
🫀📊 Quantitative Coronary Plaque Analysis (QCPA): where do we really stand?
The 2025 ACC Scientific Statement provides the most balanced and pragmatic framework to date on how AI-enabled quantitative coronary plaque analysis (QCPA) should—and should not—be used in clinical practice .
🚀 Why QCPA matters
Advances in coronary CTA, AI segmentation, and detector technology now allow objective, volumetric quantification of plaque burden (total, calcified, non-calcified). Beyond stenosis severity, plaque burden—especially non-calcified and low-attenuation plaque—has strong prognostic relevance, particularly in patients without obstructive CAD. QCPA offers the promise of more personalized preventive care.
⚠️ But reality check
The statement is refreshingly cautious. While correlations with invasive imaging are strong for total plaque volume, accuracy drops for smaller plaque components, and inter-vendor variability remains substantial. Overcalling subvisual plaque is a real risk, especially in low-risk patients, potentially leading to anxiety and overtreatment. Importantly, there is still no definitive evidence that QCPA improves hard clinical outcomes.
📌 Key clinical takeaways
✅ QCPA may be useful only when plaque is visually present on coronary CTA, to refine risk stratification and guide preventive therapy intensity.
❌ QCPA should not be reported in isolation or when visual plaque is absent (CAD-RADS 0).
👩⚕️ Human oversight is mandatory: physicians must review raw images and AI outputs.
📄 Reports must be standardized (TPV, NCPV, CPV, segments analyzed, comparison with prior scans).
🔁 Serial imaging? Use with restraint
Routine serial QCPA is not recommended. If performed, it should be in select cases, with long intervals (≥2–5 years), identical protocols, and cautious interpretation of progression thresholds.
🔮 The road ahead
Standardization, cross-vendor validation, outcome-anchored thresholds, and integration into trials are essential. QCPA is a powerful tool—but only when used expertly, selectively, and responsibly.
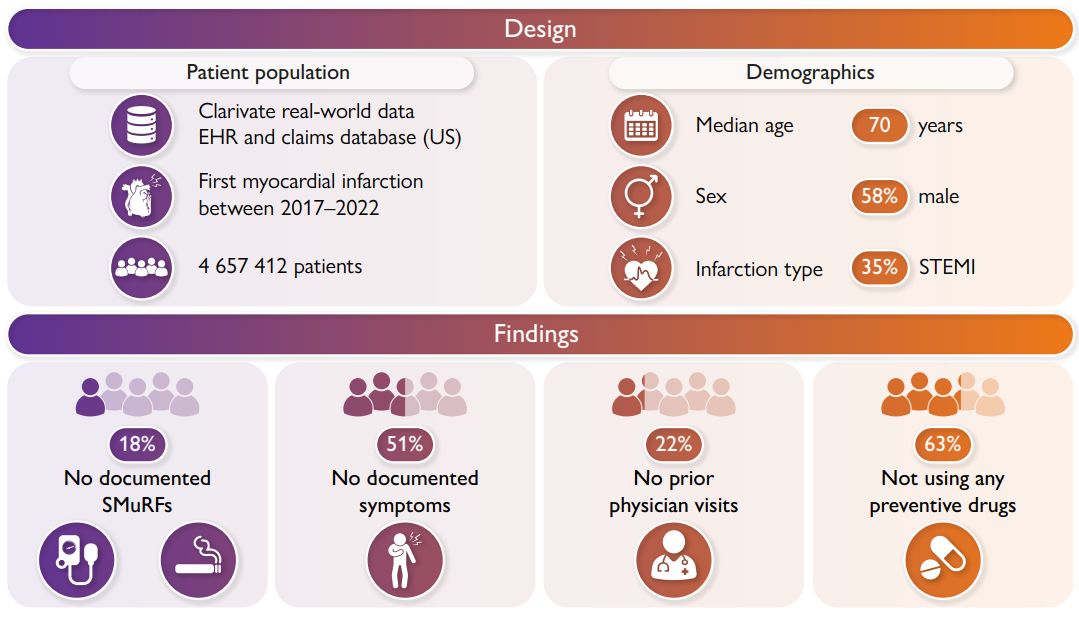
🚨 Preventing first heart attacks may need a rethink.
🔬 In this massive study of 4.6 million people with their first heart attack:
--18% had no standard modifiable risk factors
--51% had no warning symptoms beforehand
--63% weren't on preventive meds (only 22% on statin)
🌟🌟Coronary artery disease: a BIG movement to change from reactive end-stage treatment to early detection and treatment: https://t.co/xyqwuEDHFR
Kudos to the The Lancet Commission for actively studying the global health benefits of this paradigm shift from "ischemic" heart disease to atherosclerosis!🌟🌟