It's #tractTuesday! Knowing tract directions helps with Wallerian degeneration in the cord. Tracts carrying info FROM the limbs (dorsal columns) degenerate ABOVE the level of injury, and tracts carrying info TO the limbs (lateral corticospinal) degenerate BELOW the injury #spine
Evolution of @TheAJNR with clinically helpful articles like this!
Stepwise Diagnostic Algorithm for Imaging of Mandibular and Maxillary Reconstruction https://t.co/UzLR5Fjnjj
Hip pain X-ray:
Pearl:
Don’t miss faint, amorphous calcification at the greater trochanter - calcific tendinosis (HADD) of the gluteal tendons.
Recognize it as a cause of significant lateral hip pain. It’s often underdiagnosed, yet treatable.
Pitfall:
Sometimes dismissed as an artifact or cortical irregularity.
Wisdom:
Every image holds two stories: the one that is seen, and the one that reveals itself only if you dare to look closer and deeper.
—My reporting list: pearls, pitfalls, and wisdom
Pearl:
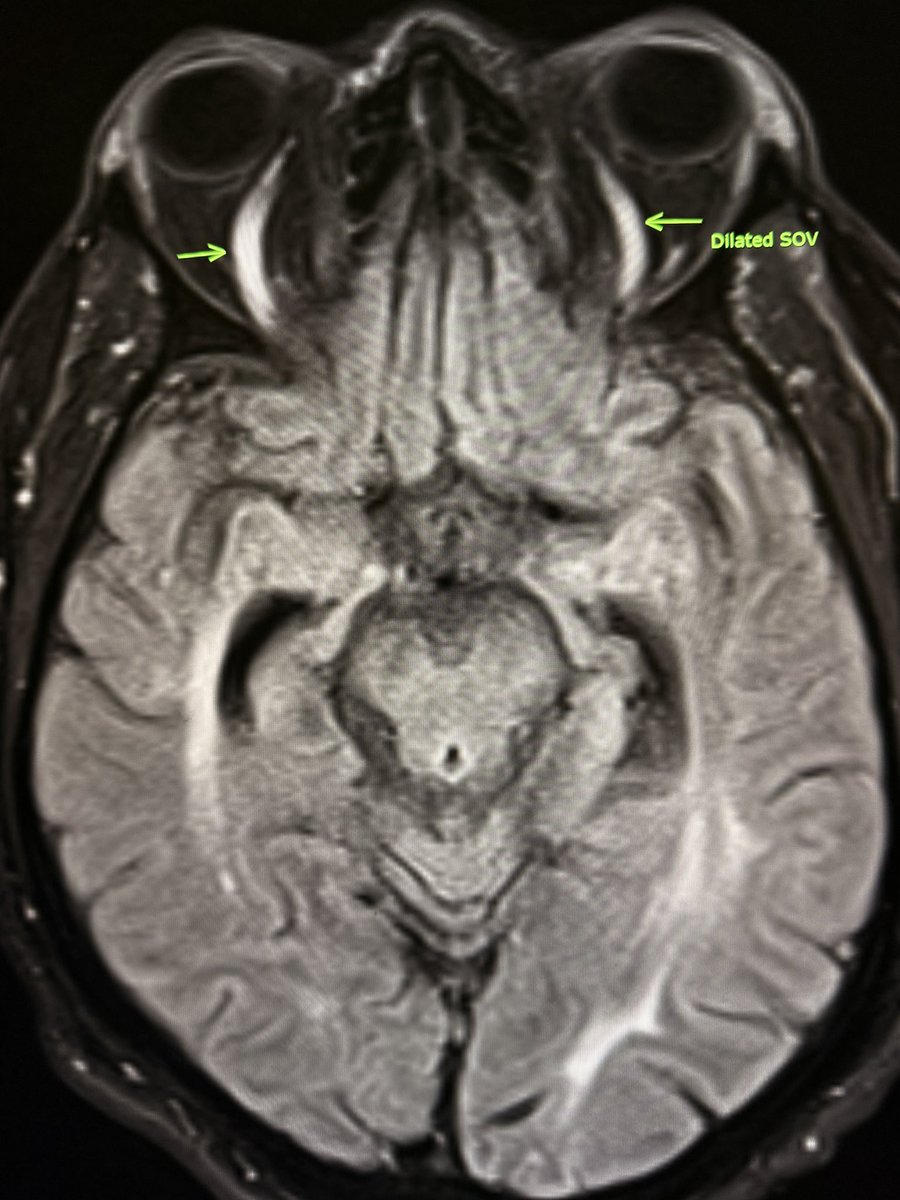
Dilated superior ophthalmic veins can be seen in intubated ICU patients due to raised intrathoracic pressure and venous congestion.
Pitfall:
Don’t overcall it cavernous sinus thrombosis. Bilateral, symmetric dilation without orbital congestion is usually benign.
Wisdom:
Machines breathe, but veins still tell stories. In critical care imaging, veins often reflect physiology. Always read the patient, not just the pixels.
—Pearls, pitfalls and wisdom from my reporting list
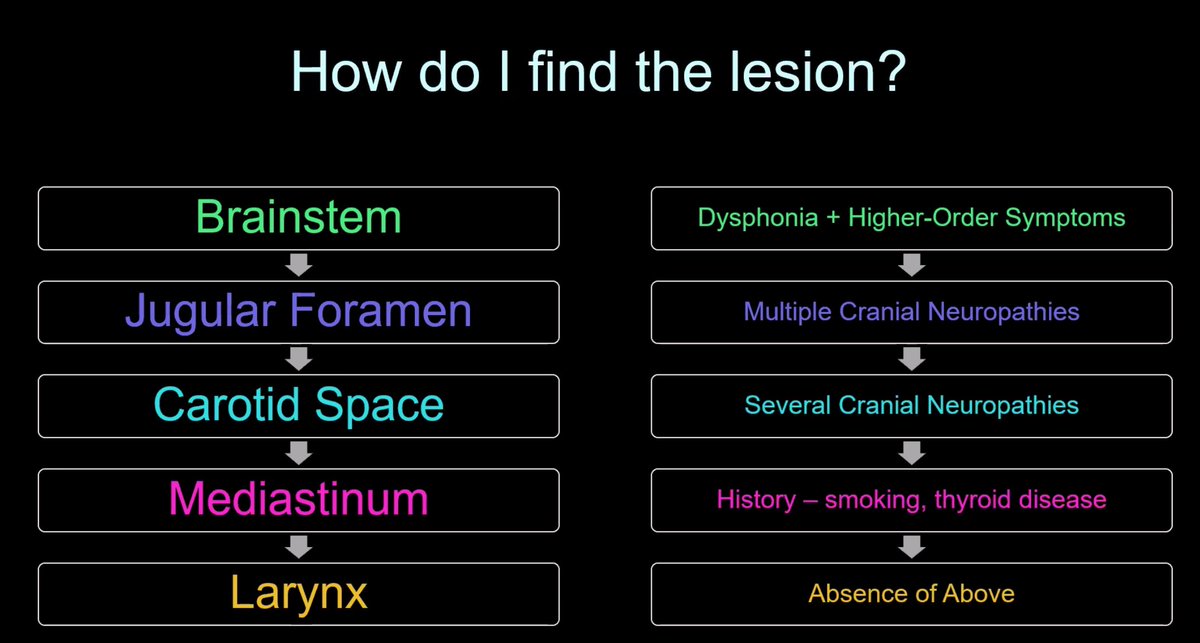
Snapshots from today’s ESHNR webinar — “Imaging Approach to Dysphonia” by @Alok_A_Bhatt moderated by @SalmanQureshiDr
Sharing key takeaways below ⤵️
🎥Recording available for ESHNR members. 🔒
Apply/renew membership: https://t.co/xjXkNlGIMa 🔗
The vast majority of the alphabet-soup instability lesions are located at the anterior-inferior aspect of the GHJ & are associated with anterior instability and/or sequela of anterior dislocation. Lesions such as : Hill-Sachs, Bankart, Perthes, HAGL, Bony HAGL , ALPSA.
🫁 Answer: Pulmonary hamartoma
📌 A common benign lung tumor — and a classic boards + real-world pearl.
🔑 High-yield imaging clues:
• Well-circumscribed, solitary pulmonary nodule
• “Popcorn” calcifications are common 🍿 (pathognomonic)
• Intralesional fat on CT = huge clue
• Slow or no growth over time
🧠 Why it matters:
Recognizing this saves patients from unnecessary biopsies, anxiety, and follow-up scans.
👀 Pearl: Not every lung nodule needs a panic spiral — some just need pattern recognition and aggressive windowing/leveling.
#Radiology #RadTwitter #MedTwitter #Radres
🎙️ Join the ESHNR Webinar!
📅 Jan 27 | ⏰ 18:00 CET
Imaging Approach to Dysphonia
👨⚕️ Speaker: @Alok_A_Bhatt
🎓 Moderator: @SalmanQureshiDr
🔗 Register: https://t.co/9kVZA8qj42
📖 Related reading: https://t.co/6W1QTr4iLW Insights into Imaging
👀 A sneak preview of the talk
🔵 Diffusion-weighted Imaging Distortion in Prostate MRI: A Cross-sectional Study Comparing Supine and Prone Positioning
https://t.co/b5X4mGfF3E
👍Congratulations to @Tristan_Radiol and his Team for this very nice publication
#prostateMRI#prostatecancer#CancerResearch #TeamScience
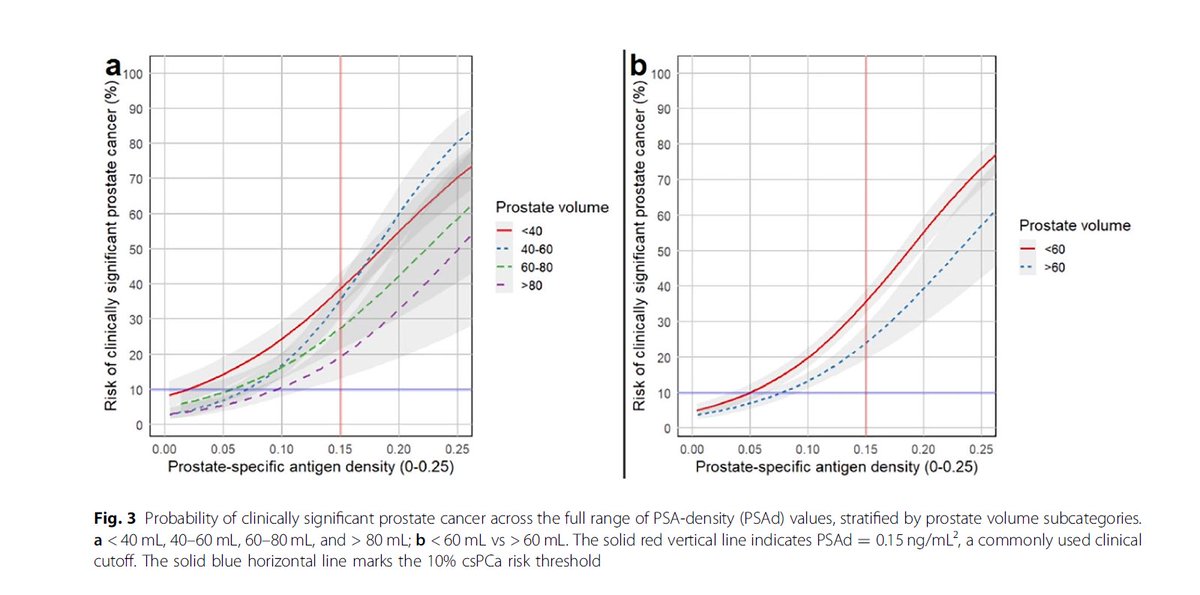
The effects of prostate volume and PI-RADS category on optimal PSA-density thresholds for biopsy decision-making
https://t.co/Bq6vfxhmZy
🔵PSA-density cut-offs of 0.20ng/mL² (PI-RADS 1–2) and 0.12ng/mL² (PI-RADS 3) can guide biopsy decisions
🟡 In PI-RADS 1–3 patients with large prostate (≥ 60 mL), PSA-density becomes significantly less predictive, and low values may not reliably exclude clinically significant prostate cancer
👍Congratulations to @Tristan_Radiol and his team for this important work
#prostatecancer #prostateMRI #Radiology
Extraforaminal disc herniation; a relatively rare cause of radiculopathy that is easy to miss on MRI.
Arrowhead shows nerve root. https://t.co/UvAWkCctEd
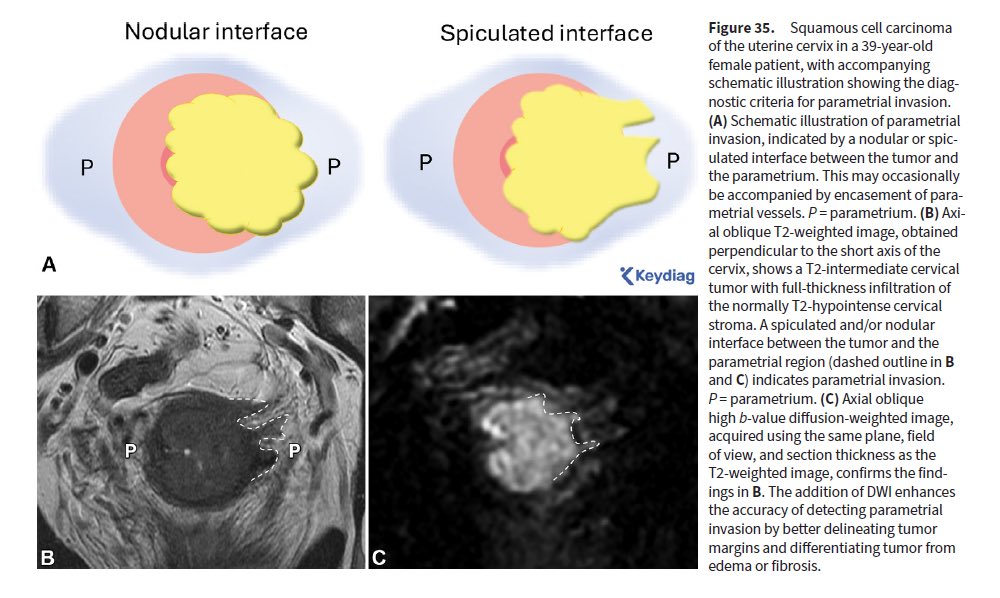
📣 Excellent article in RadioGraphics: “Reference Handbook of Gynecologic Pelvic MRI”
https://t.co/EQjugs2Cce
✅Tailored protocols
✅Normal pelvic anatomy with excellent illustrations and MR images
✅Step-by-step lesion characterization ✅Structured reporting for adnexal masses, endometriosis, cancer staging and more!
🥇Super helpful for radiologists! 🙏
👍 Congratulations to all Authors for this fantastic practical guide! 📚🩻
#Radiology #GynOnc #MRI
Case 172: Right Adrenal Gland Biopsy with an Ipsilateral Up Decubitus Approach Using Hydrodissection
66-years old treated for Ca lung had a right adrenal nodule
The video explains why prone and ipsilateral down (the two common approaches) didn't work but surprisingly an ipsilateral up approach did.
An approach to adrenal gland lesions can generally be found by trying out different positions from prone to ipsilateral down to ipsilateral up decubitus. Hydrodissection helps
Video
https://t.co/VVd0udTchZ
#ctbiopsy #adrenal #carcinoma #metastasis #hydrodissection
Cortical Infarcts Spectrum:
Patient with acute neuro deficits. MRI DWI shows:
•Tiny punctate foci in right insular cortex → acute cortical microinfarcts (≤5 mm)
•Slightly larger cortically confined lesion in right parieto-occipital cortex ( → small cortical infarct (>5 mm)
Pearls:
•Microinfarcts: sharply cortically confined, ≤5 mm, often embolic or amyloid angiopathy related.
•Small cortical infarcts: >5 mm but not territorial; often embolic or hypoperfusion related.
Pitfalls:
•Don’t mislabel as “lacunar” (those are deep, subcortical, small vessel disease).
•Easy to miss on DWI if punctate—always correlate with ADC.
Wisdom:
•Micro + small cortical infarcts in the same patient often = embolic shower or diffuse vascular vulnerability.
•Small dots can carry big meaning—always prompt a search for embolic source, AF, carotid, cardiac, amyloid.
—Pearls, pitfalls and wisdom from my reporting list