Los #CriteriosLight diferencian #EXUDADO🟡de #TRASUDADO💧PLEURAL🫁pero necesita #muestraSanguinea🩸
En #ERJOpenReseach:COMBINACIÓN pleural de 3:
👉🏻Proteínas>3 g/dL
👉🏻LDH>250 UI/L
👉🏻Colesterol>55 mg/dL
Igualó precisión de Light y mejoró la especificidad
🔗🆓https://t.co/FhSB7WN96K
📌 Definiendo la fibrosis pulmonar progresiva: implicaciones para ensayos clínicos, guías y atención al paciente 🫁
Una editorial de:
✍️ Alyson W. Wong
✍️ Christopher J. Ryerson
Consulta el contenido aquí ⬇️
🔗 https://t.co/hCt0vh2FHm
#ArchivosdeBronconeumología#SEPAR
🫁🦠Abordaje y Manejo de la Neumonia Asociada a Ventilación Mecánica
🔰📚Infect Dis Clin
https://t.co/YZCRND2npc
Enlace a Artículo Completo👇🏻🆓✅
https://t.co/xumUMHaxVK
En este artículo científico, publicado en la revista SCIENCE, los autores concluyen que el teletrabajo aumenta de forma significativa el aislamiento social y empeora la salud mental, sobre todo en las personas que viven solas. Estiman que el teletrabajo puede explicar hasta un tercio del aumento global del malestar psicológico -observado en el período estudiado. Y recomiendan que trabajadores, empresas y gobiernos tengan en cuenta estos efectos al diseñar políticas laborales.
El artículo cuestiona la extendida idea, tras la pandemia, de que teletrabajar desde casa es siempre una mejora. Desde luego los datos sugieren que la productividad y la comodidad no agotan el problema. Era evidente que las personas no sólo necesitamos eficiencia; también encuentros cotidianos y formas ordinarias de convivencia. Así que puede que el lugar de trabajo sea al mismo tiempo un espacio de relación humana cuya importancia habíamos subestimado
🫁💥Ajustes Ventilatorios Guiados por la Mecánica Respiratoria en el SDRA
🔰📚Annals of Intensive Care
https://t.co/JVUnZtouWg
Enlace a Artículo Completo👇🏻🆓✅
https://t.co/rPEDXf5xvO
📖✨¡Por fin está aquí!
Después de casi tres años de trabajo colaborativo, hoy se publican las Bases Técnicas del Plan de Aceleración para Detener la Obesidad en México 2025-2030.
Este documento es el resultado de un amplio proceso de construcción colectiva que reunió las voces, experiencia y conocimiento de más de 80 expertos nacionales, así como los aportes generados a través de grupos de discusión, talleres de trabajo y una exhaustiva revisión de la evidencia científica disponible. 🤝🔬
Las Bases Técnicas presentan una hoja de ruta con las prioridades y acciones estratégicas necesarias para avanzar hacia el cumplimiento de las metas de reducción de la prevalencia de obesidad al año 2030. 🎯
📲 Consulta y descarga el libro aquí:
https://t.co/5D47mXEGGj
#Obesidad #SaludPública #PolíticasPúblicas #EntornosSaludables #México #ObesidadSeriamente
🤒Fever is not the rule in sepsis.
And perhaps we have underestimated what the absence of fever actually means.
This important multicentre Australian cohort study analyzed more than 15,000 ICU patients with sepsis and found something striking:
Only 1 in 15 septic ICU patients arrived with a temperature ≥38.3°C.
Most septic patients were either normothermic or hypothermic.
Even more interesting: 21% arrived hypothermic (<36°C), and this group had the highest mortality, vasopressor requirement, mechanical ventilation use, and renal replacement therapy rates.
30 day mortality:
• Fever ≥38.3°C → 14%
• Normothermia 36–37.4°C → 12%
• Hypothermia <36°C → 17%
The paper introduces a fascinating concept: “fever deficit”
Defined as the cumulative degree-hours below 38.3°C during the first 72h of ICU admission.
Patients with hypothermia accumulated massive fever deficits: median 85 degree-hours over 72h.
The physiology behind this may be extremely important.
Fever is not simply a symptom. It is a coordinated host defense response:
• enhanced leukocyte function
• increased cytokine signaling
• improved microbial clearance
• reduced pathogen replication
• potentiation of antibiotic activity
Hypothermia in sepsis may represent:
• immune exhaustion
• failed thermoregulatory response
• depleted physiological reserve
• maladaptive host response
The authors even raise a provocative possibility:
Should we actively warm afebrile septic patients toward high-normal or supranormal temperatures?
Not just “avoid hypothermia”… but therapeutic hyperthermia.
That idea sounds radical at first glance, yet several observations support it:
• hypothermic sepsis consistently carries worse outcomes
• microbial growth increases at lower temperatures
• antibiotic efficacy may decrease in hypothermia
• febrile patients often survive more frequently than afebrile patients
One particularly important finding: temperatures normalized rapidly during the first 12-24h in ICU, but patients rarely became febrile afterward.
Meaning: our current ICU practice may unintentionally suppress or fail to restore a potentially protective physiological response.
This paper opens an important discussion in critical care:
In selected septic patients, should temperature become a therapeutic target similar to MAP, oxygenation, or perfusion?
Excellent paper challenging one of the oldest assumptions in ICU medicine, that fever in sepsis is primarily harmful.
Reference 📚
White KC et al. Sepsis in the absence of fever: Determining the criteria for and feasibility of future therapeutic temperature management trials. Critical Care and Resuscitation. 2025;27:100135. https://t.co/U7GJKjbWqT
📊 JAMA Clinical Guidelines Synopsis: The 2025 guideline for #ACS management recommends dual antiplatelet therapy with aspirin and a P2Y12 inhibitor, high-intensity statins, invasive revascularization, and radial access for angiography.
https://t.co/OnEihazgow
Las nuevas Guías Latinoamericanas de Pancreatitis Aguda (2026). Puntos importantes:
🟢 Cambio en el paradigma (gracias a WATERFALL Trial y otros): reanimación hídrica moderada a 1.5 ml/kg/h, con bolo SOLO en caso de haber hipovolemia franca.
🟢 No uses antibióticos profilácticos, solo en caso de necrosis pancreática infectada.
🟢 La CPRE es urgente (<24 horas) solo si hay colangitis aguda, sino no.
🟢 Menos es más; intenta diferir por lo menos 4 semanas la intervención de colecciones pancreáticas. Y si se necesita, idealmente endoscópico transluminal guiado por ultrasonido.
🟢 La hipertrigliceridemia es una causa (sobre todo si >500-1,000 mg/dL). El tratamiento: insulina en infusión.
Las voy a leer a fondo para actualizar las apps (https://t.co/FZoAsLTFc2).
🦠 El #Ébola sigue recordándonos que una zoonosis puede convertirse rápidamente en una emergencia global. Su alta letalidad y transmisión por fluidos exigen diagnóstico precoz, aislamiento, bioseguridad y vigilancia estricta. 🚨👩⚕️
💉 Vacunas como Ervebo y Zabdeno/Mvabea han transformado la respuesta, pero persisten desafíos: acceso equitativo, cadenas de frío, confianza pública, vigilancia genómica y protección del personal sanitario.
🌍 El reto es actuar antes de que el brote cruce fronteras: investigar, vacunar y responder con enfoque #OneHealth para salvar vidas.
#SaludGlobal #EbolaVirus #SaludPública #Infectología #Prevención@josemillanonate
Aztreonam-Avibactam for Carbapenem-Resistant Gram-Negative Infections: Mechanisms, Clinical Efficacy, the Challenge of Resistance and Susceptibility Testing | International Journal of Antimicrobial Agents
(https://t.co/AWOP03O3FJ)
🩸Anticoagulation in the ICU is not one protocol. It is a daily balance between thrombosis, bleeding, renal clearance, procedure timing, and the reason for anticoagulation.
Recent PubMed indexed guidance reinforces that critically ill patients need systematic VTE prophylaxis unless bleeding risk is prohibitive (Bounes et al., 2024; Arabi & Mehta, 2025).
But dose is context.
Standard ICU prophylaxis is often enoxaparin 40 mg once daily or UFH 5000 IU every 8 to 12 hours. In obesity, fixed low dosing may underdose patients, reflecting the need for higher or weight adjusted prophylaxis in selected patients (Arcelus et al., 2024). In AKI or severe CKD, UFH is often safer than LMWH because accumulation is less problematic and reversal is easier.
Therapeutic anticoagulation is a different question.
AF in the ICU requires stroke risk, bleeding risk, rhythm duration, procedures, renal function, and enteral absorption assessment. The 2023 ACC/AHA/ACCP/HRS AF guideline supports DOACs over warfarin for most non valvular AF, but not for mechanical valves or moderate to severe rheumatic mitral stenosis (Joglar et al., 2023).
PE in shock is not “just anticoagulation.” It is anticoagulation plus reperfusion assessment. The 2026 AHA/ACC multisociety PE guideline focuses on risk stratification, anticoagulation, catheter based therapy, thrombolysis, surgical embolectomy, and IVC filters when anticoagulation is impossible (AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM Writing Committee, 2026).
Mechanical valves remain warfarin territory. DOACs are not substitutes. Bridging decisions must consider valve type, position, prior stroke, AF, LV dysfunction, and bleeding risk.
Liver failure is not “auto anticoagulated.” Cirrhosis creates rebalanced but fragile hemostasis. Hospitalized cirrhotic patients can thrombose and may still need prophylaxis or treatment when bleeding risk is controlled (Roark et al., 2024).
Recent stroke, major surgery, ACS, elderly frailty, thrombocytopenia, and renal dysfunction all change the equation. Mechanical prophylaxis may be useful when pharmacological prophylaxis is temporarily unsafe, and a 2024 meta analysis supports intermittent pneumatic compression as an option in surgical patients, especially when bleeding risk limits anticoagulants (Kim et al., 2024).
References📚
*AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM Writing Committee. Circulation. https://t.co/EGd3n1NDUW
*Arabi, Y. M. Intensive Care Medicine, 51, 1508–1510. https://t.co/LylFk2NVlr
*Arcelus, J. I., Eur J Anaesthesiol. 2024 Aug 1;41(8):607-611. doi: 10.1097/EJA.0000000000002000.
*Bounes, F., European Journal of Anaesthesiology, 41(8), 582–588. https://t.co/4EtIe75hh9
*Joglar, J. A., Circulation, 149(1), e1–e156. https://t.co/wlIzj89iJS
*Kim, N. Y. PLOS ONE, 19(7), e0307602. https://t.co/UnND9Cv59L
*Roark, R., Clin Liver Dis (Hoboken). 2024 Jun 19;23(1):e0186. doi: 10.1097/CLD.0000000000000186.
🚨🚨 IMPORTANTE ! #HONGOS
¿Cómo ha cambiado el #DIAGNÓSTICO de las infecciones fúngicas graves? 🍄🏥
La British Society for Medical Mycology actualiza sus recomendaciones de buenas prácticas: el diagnóstico ya no puede depender solo del cultivo y la microscopía, sino que debe integrar PCR, antígenos, anticuerpos, 1,3-β-D-glucano y monitorización terapéutica cuando proceda.
Puntos clave de la actualización 2025:↙️
✅ Uso reforzado de PCR para Pneumocystis
✅ Pruebas específicas para candidiasis invasiva y aspergilosis
✅ Elección de muestras y test según síndrome clínico y riesgo del paciente
✅ Tiempos de respuesta definidos para acelerar decisiones clínicas
✅ Integración con programas de uso racional de antifúngicos
La guía recuerda algo esencial: diagnosticar antes no solo depende de más tecnología, sino de circuitos clínico-microbiológicos rápidos, experiencia de laboratorio y criterios comunes de calidad.
En entornos con menos recursos, la microscopía directa bien realizada sigue siendo una herramienta de alto valor, especialmente si se integra con derivación y confirmación cuando sea posible.
🔗↘️↘️↘️
https://t.co/fzvMF0dnpU
#Medicina #Micología #Microbiología #InfeccionesFúngicas #Diagnóstico #SaludPública #Antifúngicos #LancetInfectiousDiseases @AEMMicologia@SEIMC_@FINBAsturias@HUCA_Asturias@SEMicrobiologia
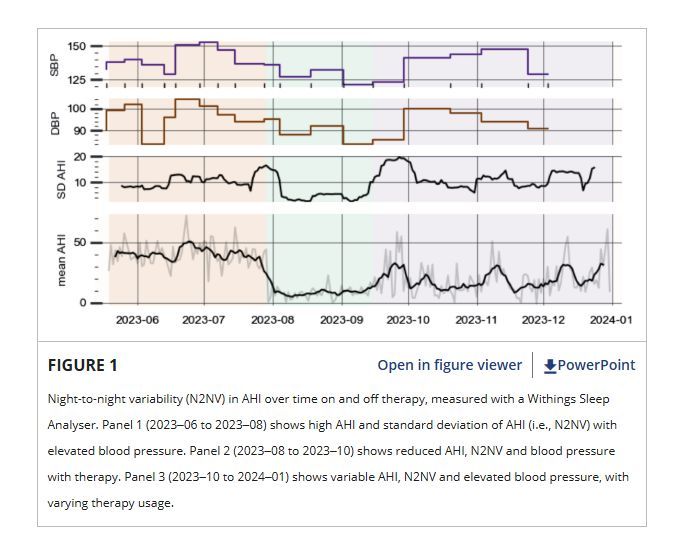
🗨️ COMMENTARY: New Obstructive Sleep Apnoea Multi-Night Diagnostic Devices. Is a Single Night of Measurement Now Considered Enough?
https://t.co/Nv5cWTlXv3