Adaptive DBS and the future of walking: Proceedings is out from the XIII annual DBS Think Tank. Adaptive DBS refers to a form of deep brain stimulation where the device senses brain signals and automatically adjusts stimulation in real time, instead of delivering constant stimulation. Chance Fleeting and colleagues just dropped a new paper in Frontiers in Human Neuroscience summarizing the 13th Annual DBS Think Tank held at the Fixel Institute for Neurological Diseases at the University of Florida. The meeting gathered engineers, neuroscientists, industry partners and health care providers to discuss the evolving landscape of DBS, including adaptive stimulation for walking and more broad brain network therapies.
Key points on the 'walking work:'
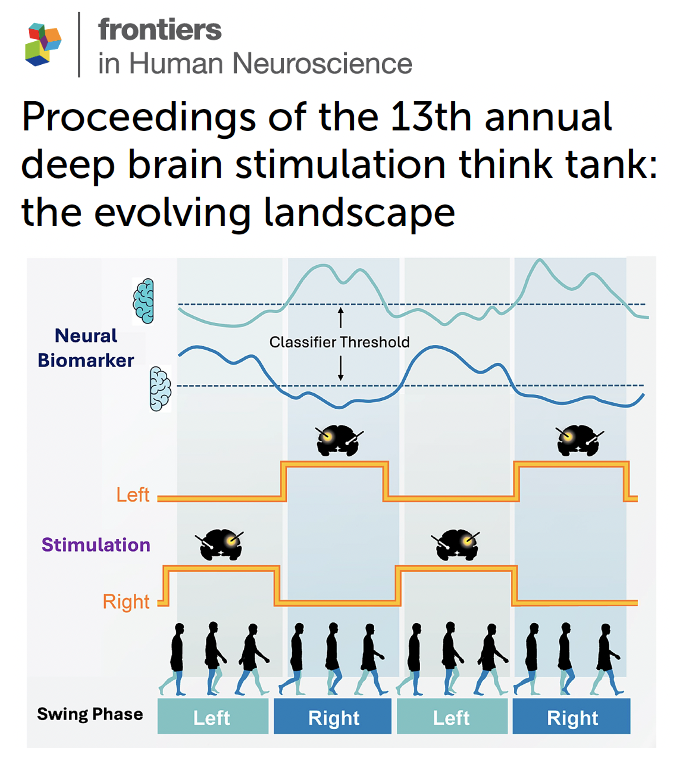
- Adaptive DBS synchronized to the walking cycle (Doris Wang lab at UCSF) can adjust stimulation during specific phases of gait and has shown improvements in symmetry, variability and fall reduction in Parkinson’s disease.
- Neural signals from the subthalamic nucleus and other brain regions can decode mobility states such as sitting, standing and walking, allowing stimulation to switch automatically to gait optimized settings.
- Modern DBS is shifting from targeting a single brain location to targeting distributed brain networks and to using biomarkers to determine where, when and in whom stimulation should occur.
My take: The DBS field is rapidly moving toward smarter stimulation. Instead of delivering the same signal continuously, next generation systems can sense brain activity, recognize behavior and adjust therapy dynamically. This shift toward adaptive and network guided stimulation may one day help to address some of the most stubborn Parkinson’s symptoms such as gait freezing and falls. Please read and decide on your won as I am biased as a co-author and participant in the meeting.
Here are 5 points that resonated w/ me:
1- Walking problems in Parkinson’s frequently persisted even when tremor and stiffness improved, making gait a critical target for next generation DBS strategies.
2- Adaptive DBS can synchronize stimulation to real world behaviors such as stepping, creating therapy that matches the brain’s natural timing.
3- Brain network mapping is revealing that DBS outcomes depend not only on where stimulation occurs, but also on who receives it and when stimulation is delivered.
4- Neural sensing technologies now allow implanted devices to record brain signals continuously, opening the door to automated and personalized therapy adjustments.
5- The future of DBS will likely blend sensing, AI driven decoding and adaptive stimulation so therapy responds dynamically to how folks move and function in daily life.
https://t.co/U4OspsgyNY @DBSThinkTank@ParkinsonDotOrg #parkinson #depression
When motor fluctuations persist despite optimized use of levodopa + MAO‑B + COMT + DA agonists (± amantadine), think Refractory Motor Complications (RMC). Before jumping to DBS/infusions, ensure true best‑medical therapy has been tried. Pearls: maximize dosing frequency, use ER/OD formulations, educate on timing + food interactions. https://t.co/X5X5X4ln5Y
نظرا لكثرة الاستفسارات التي تلقيتها من المرضى وذويهم بعد اعتماد هيئة الدواء والغذاء السعودية مستحضر " لكمبي " #ليكانيماب " كأول علاج لمرض #ألزهايمر في السعودية بعد تقييم فعاليته وسلامته واستيفائه للمعايير المطلوبة أود ان اذكر في سلسلة التغريدات القادمة بعض المعلومات عنه.
•Tenderness over ischiofemoral space
•MRI shows narrowed ischiofemoral + quadratus femoris spaces
🎯 Don’t forget to include IFI in your differential for posterior hip or buttock pain—especially in patients not responding to piriformis-targeted treatments
Unlike piriformis syndrome, IFI involves compression of the quadratus femoris between the ischial tuberosity and lesser trochanter, often due to pelvic morphology or post-op changes.
📌 Clues:
•Deep gluteal pain
•Worse with hip extension/adduction
A new video from Dr. Diana Angelika Olszewska & Prof. Anthony Lang from Toronto demonstrates how to perform a skin punch biopsy in Parkinsonism. Includes a live patient demo. A must-watch for clinicians and researchers alike! https://t.co/9ym5wZDakc
تنظّم الجمعية السعودية لمرضى الباركنسون (المؤتمر العلمي العالمي للمستجدات في مرض باركنسون)، بدعم من صندوق دعم الجمعيات، وبالتعاون مع مستشفى الملك فيصل التخصصي، يومي 29-30 نوفمبر (الجاري) في فندق كراون بلازا بالرياض.
@saudi_neurology@saudimovdis@asfgovsa@KFSHRC
There is no room for therapeutic nihilism in ICH. It is imperative to uphold “Time is Brain” in ICH as much as in Acute ischemic stroke. Timely, multidisciplinary interventions can save millions of neurons. Code ICH can be the difference between life & death for these patients; can be the difference between a good vs poor functional outcome.
🧠ABC
🧠Time to CT/CTA
🧠Time to BP control
🧠Time to Coagulopathy reversal
🧠Time to get our neurosurgery friends involved for EVD; ENRICH/SCUBA…Go minimally invasive surgical evacuation (MIS)🙌
🧠 Time to get multidisciplinary teams involved from triage to recovery
@caseyalbin@stephanamayer@aartisarwal@neurocritical@CuringComa #CuringComa #CHEST2024 bookmark this manuscript
بيان الشعبة السعودية لطب أعصاب #الإدراك و #السلوك بخصوص تصريح هيئة الغذاء و الدواء الأمريكية باستخدام دواء #كيسونلا و ما يعنيه ذلك بالنسبة للعلاجات المناعية لمرض #ألزهايمر.
رزقكم الله جميعا #الصحة و العافية.
@saudi_neurology