Today we publish our paper 'A decade of better MSK health' setting out the change needed to achieve our vision of better MSK health for everyone.
You can read it here; https://t.co/qB1tPYTyQZ
For med twitter and doctors poor at maths and statistics 👇
📊 Relative Risk. Odds Ratio. Hazard Ratio.
Read the Statistic Before You Quote the Result.
To all clinicians interpreting medical literature:
These three numbers are not interchangeable. They answer different questions.
⸻
1️⃣ Relative Risk (Risk Ratio)
Question:
“How much did the overall probability change?”
Example:
30% flare in placebo
15% flare in treatment
Relative Risk = 0.5
Meaning:
The treatment group had half the total risk of flare at 1 year.
It compares final percentages.
It does not consider timing.
Common in:
•Randomized trials
•Cohort studies
⸻
2️⃣ Odds Ratio
Question:
“How do the odds compare?”
Odds is not probability.
If 30% flare:
•30 flare
•70 do not
Odds = 30 / 70
Odds compares event vs non-event.
In a case-control study on smoking and lung cancer:
If smokers are 3 times more common among cancer patients than controls:
Odds Ratio = 3
Meaning:
The odds of smoking are 3 times higher among cancer patients.
It does NOT directly mean risk is 3 times higher.
Why?
Because in case-control studies:
•We artificially choose how many cases exist.
•True incidence cannot be calculated.
Logistic regression also produces Odds Ratios.
Important:
If the outcome is common, Odds Ratio exaggerates the effect compared to Relative Risk.
⸻
3️⃣ Hazard Ratio
Question:
“At any given time, how fast is the event happening?”
Example:
Cancer relapse over 5 years.
Hazard Ratio = 0.6
Meaning:
At any moment during follow-up, relapse is happening 40% less frequently in the treatment group.
It accounts for:
•Timing
•Censoring
•Variable follow-up
Used in survival analysis and Cox regression.
⸻
The Practical Difference
Relative Risk → compares total probability
Odds Ratio → compares event vs non-event odds
Hazard Ratio → compares event rates over time
Same percentage reduction.
Different meaning.
⸻
Before quoting “50% reduction” in a journal club, conference, or clinic:
Ask:
• Is this probability?
• Is this odds from logistic regression?
• Is this time-to-event data?
Interpret the model before interpreting the magnitude.
Statistical literacy is not optional.
It directly affects how we counsel patients and choose therapies.
Read beyond the abstract.
Your patients deserve precision.
'A Duty Forsaken: The Legal and Ethical Abandonment of ME/CFS Patients'
Thanks to Jenny Wilson (@JennyWi04810918) for preparing this summary of a longer document she is working on. I'm going to send a copy to my MP @BeccyCooper4Lab. #MyalgicEncephalomyelitis#MECFS
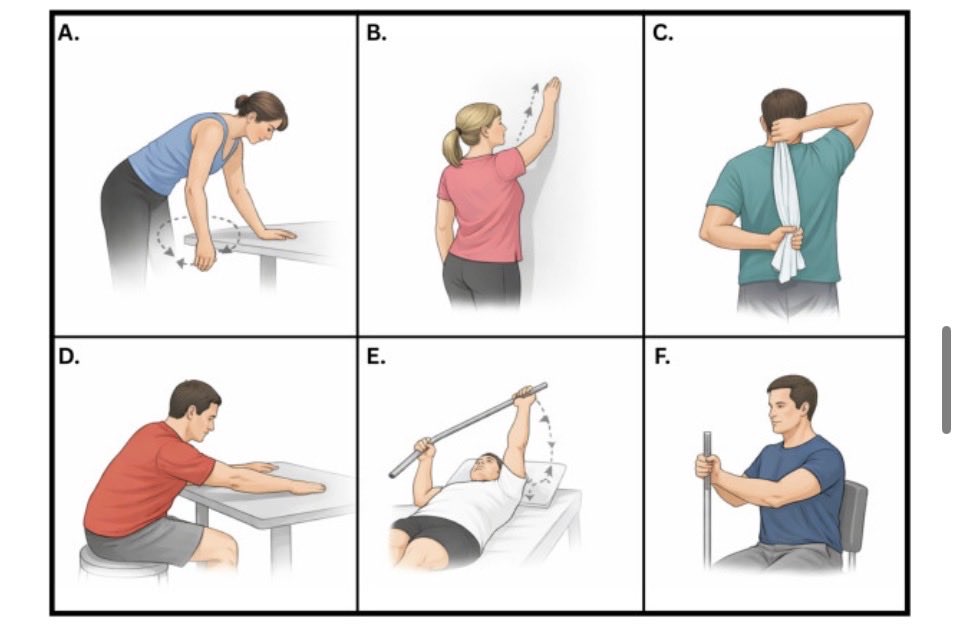
❄️FROZEN SHOULDER❄️
Just published narrative review…
😲Watchful waiting = Physio
💊Low dose steroid = high dose
🔍Ultrasound CSI guided NOT superior to landmark
💥Hydrodistension promising…
Full text: https://t.co/IBP3hhpoW5
More injection CPD here: https://t.co/6D81EaZXAi
Strength is a function of practice. It's self-evident that you will get stronger lifting heavier weights - because that's what you practice doing = the principle of specificity. When given the opportunity to practice lifting heavy often enough, people (quite well trained) will get the same strength gains: https://t.co/zXQ2W5FlR9
IOW: Lift at 80% of 1RM - 20% away from 1RM - voila, you get better at 1RM lifts than someone who trains at 50% of 1RM (50% away from their 1RM). When given an unpracticed task, almost invariably, people get just as 'strong.'
Changing RT variables helps, but the effects are small:
https://t.co/Gv1eKnquhd https://t.co/SWS2YTzW4H
Endometriosis was once thought to be imagined by mad and ‘hysterical’ women. Some were treated with straightjackets.
Medicine has a long history of assigning blame to our brain (emotions, stress, etc) when the actual cause remains unknown. 🧵 1/
We cannot currently zoom in and determine whether a lumbar nerve root is undergoing irreversible conduction loss, e.g, demyelination, or axonal degeneration. However, this study examining prognostic factors in lumbar radiculopathy related foot drop (a form of profound myotomal weakness) may provide useful guidance until more encompassing data becomes available.
✅️ Time to Surgery: Discectomy within 6 weeks is associated with better outcomes.
✅️ Age: Younger patients (<47 years) show more favourable recovery.
✅️ Pre-operative Strength: Better baseline motor power (≥2/5 on the MRC scale) predicts improved recovery.
✅️ Early Post-operative Improvement: Demonstrating ≥1 MRC grade increase in dorsiflexion strength soon after surgery is a positive sign.
✅️ Symptom Duration: The recovery window becomes less favourable after 6 months of persistent symptoms.
Prognostic factors and surgical outcomes of foot drop secondary to lumbar degenerative disease: A systematic review and individual patient data meta-analysis
SR. 2025.
https://t.co/2hcoiyJlLm
Yesterday, I took part in presenting my research poster on the management of vertebral fractures using hydrotherapy at The University of Salford Celebration, Conference and Co-creation Event to educators and students.
@UoS_Physio@ATACP
NotebookLM is (probably) the best reading assistant for research papers.
It's free and you can use it to:
• Summarize papers
• Ask question about papers
• Prepare study guides
• Create mind maps
• Generate podcasts based on papers
And it's very easy to use:
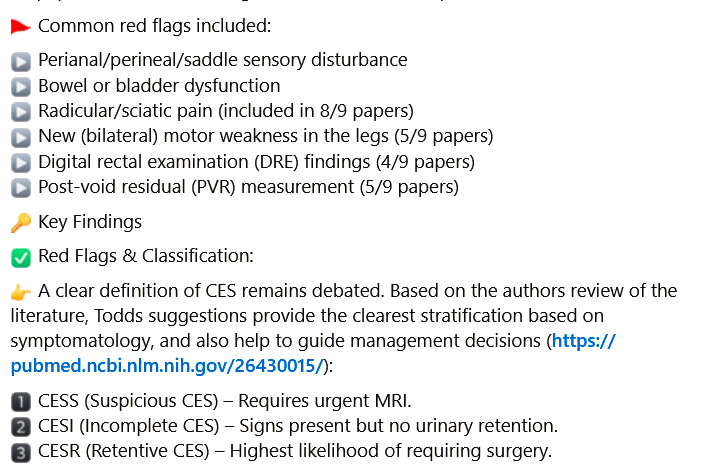
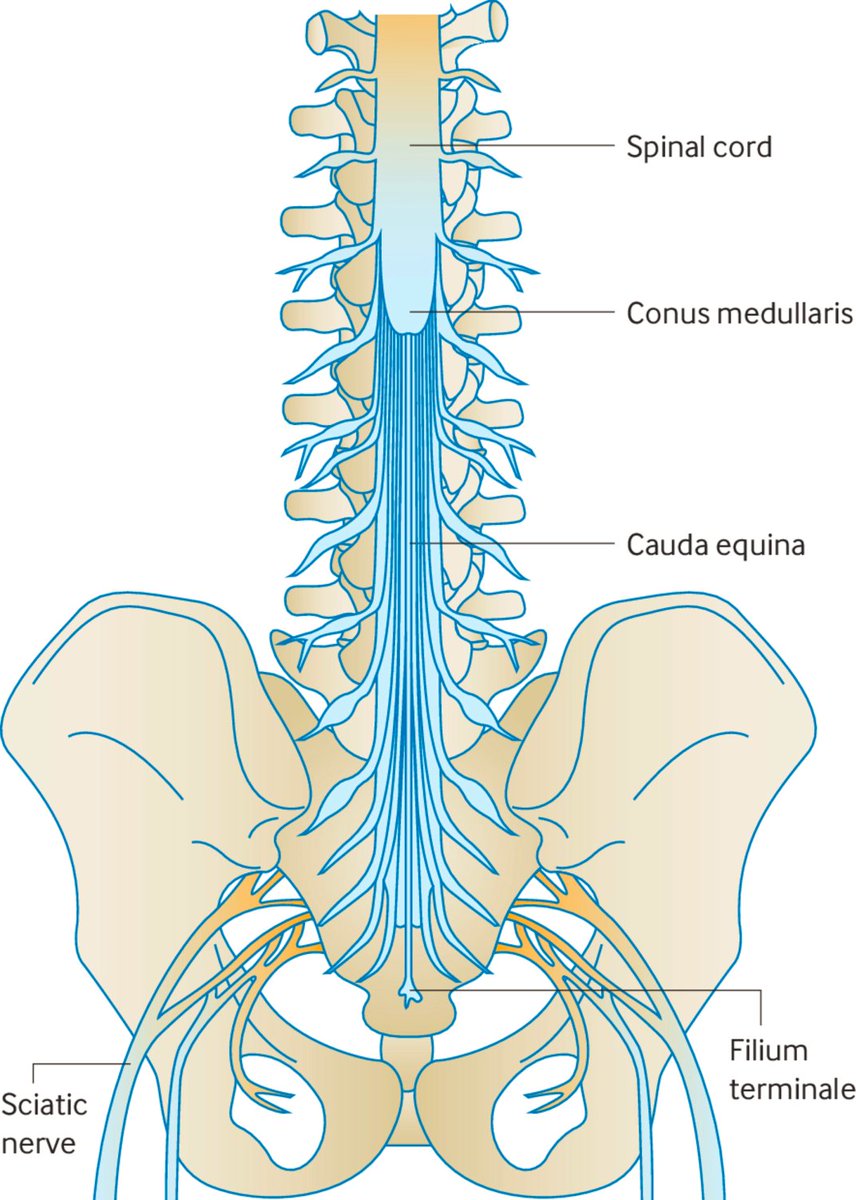
Just published 🔥
Assessment and Early Investigation of Cauda Equina Syndrome – A Systematic Review of Existing International Guidelines and Summary of the Current Evidence
👇👇👇
https://t.co/IC9Wpq2xE1
📷https://t.co/YU7UDCMHM7
Agree with @RogerKerry1 that it's impossible to draw firm conclusions from this sample. See also an extensive review from @RikKranenburg et al., 2017 (https://t.co/nLmArkmb21).
From the @IFOMPT Cervical Framework: The current hypothesis is, that patients presenting with neck pain and headache who go on to develop a serious adverse event, such as a dissection, have an underlying pathology which is subsequently aggravated by treatment (https://t.co/CcVDrSlY2C). I do agree that, based on the limited available evidence, that it's unlikely that a healthly vessel will be dissected by treatment of the cervical spine.
Re the conclusion that practitioners should exclude cervical spine pathology before performing cervical spine manipulation I largey agree. See also @AussieLouie et al, 2012 (https://t.co/HXrAUkcGwX). So this is important, however, difficult. Moreover we need to take into account the incidence arterial dissections is 1.0–3.0 per 100,000 people). Also, it's not feasible nor appropriate to use X-ray examination or other diagnostic tests in all patients.
Even more important, we need to acknowledge that a recent trauma and vascular anomalies are the most important risk factors for dissection vascular events. So, clinicians should pay attention to a previous trauma in the patient interview. However, anomalies are not identifiable in the patient interview and are largely unknown in the patients treated by clinicians.
It's also very important to pay attention to (early) clinical features (signs and sympotoms) of an underlying dissection (or more broadly: vascular flow limitation).
Re the case: in all my workshops I mention that we can't rule out the possibility that cervical spine manipulation itself, in extremely rare cases, may cause a dissection. Case 10 presented in the article might be such a case in which a vascular serious adverse event occured, potentially cause by a transdiscal fracture at C5-C6, resulting in critical stenosis and compressive myelopathy.
We don't know of the manipulation in this case was performed appropriately (I have some doubt about that), however, detailed information is lacking. Moreover, during her last session of spinal manipulation, she mentioned new-onset paresthesia beginning on the upper limbs and progressing to the lower limbs. Her complaint was disregarded, and the session continued, at the end of which she was unable to stand. Retrospectively (which is always easy), for me this emphasizes the importance of proper clinical reasoning and decision making, not only in the first session but also in follow-up treatments. Moreover, it endorses the hypothesis that the treating clinician might have been insufficiently aware and might have had insufficient contemporary knowledge about the potential incidence of serious adverse events.
Further reading (biased as I'm involved in these @MSKPhysioJnl@JOSPT@BrazJPhysTher publications):
Vascular flow limitations affecting the cervico-cranial region: Understanding ischaemia: https://t.co/sxwQbhUYEx
What to Look Out for, What to Do, and When: 3 Key Messages for Safely Treating Neck Pain, Headache, and/or Orofacial Symptoms in Musculoskeletal Rehabilitation Settings: https://t.co/sunWcw8SdZ
A guide to cranial nerve testing for musculoskeletal clinicians: https://t.co/Qg5AnXEXrA
Assessing Vascular Function in Patients With Neck Pain, Headache, and/or Orofacial Pain: Part of the Job Description of All Physical Therapists: https://t.co/ahOToADqhc
Yes, we should abandon pre-treatment positional testing of the cervical spine: https://t.co/vxQNcuY4ab
Effects of Head and Neck Positions on Blood Flow in the Vertebral, Internal Carotid, and Intracranial Arteries: A Systematic Review: https://t.co/31ZFzLGsOt
Considerations to improve the safety of cervical spine manual therapy: https://t.co/lqs9V2OldX
"The report, ‘Recipe for health: a plan to fix our broken food system’, finds that #Obesity and diet-related disease are a public health emergency..."
From @UKHouseofLords Food, Diet & Obesity Committee.
https://t.co/XLf3oNDEYW.
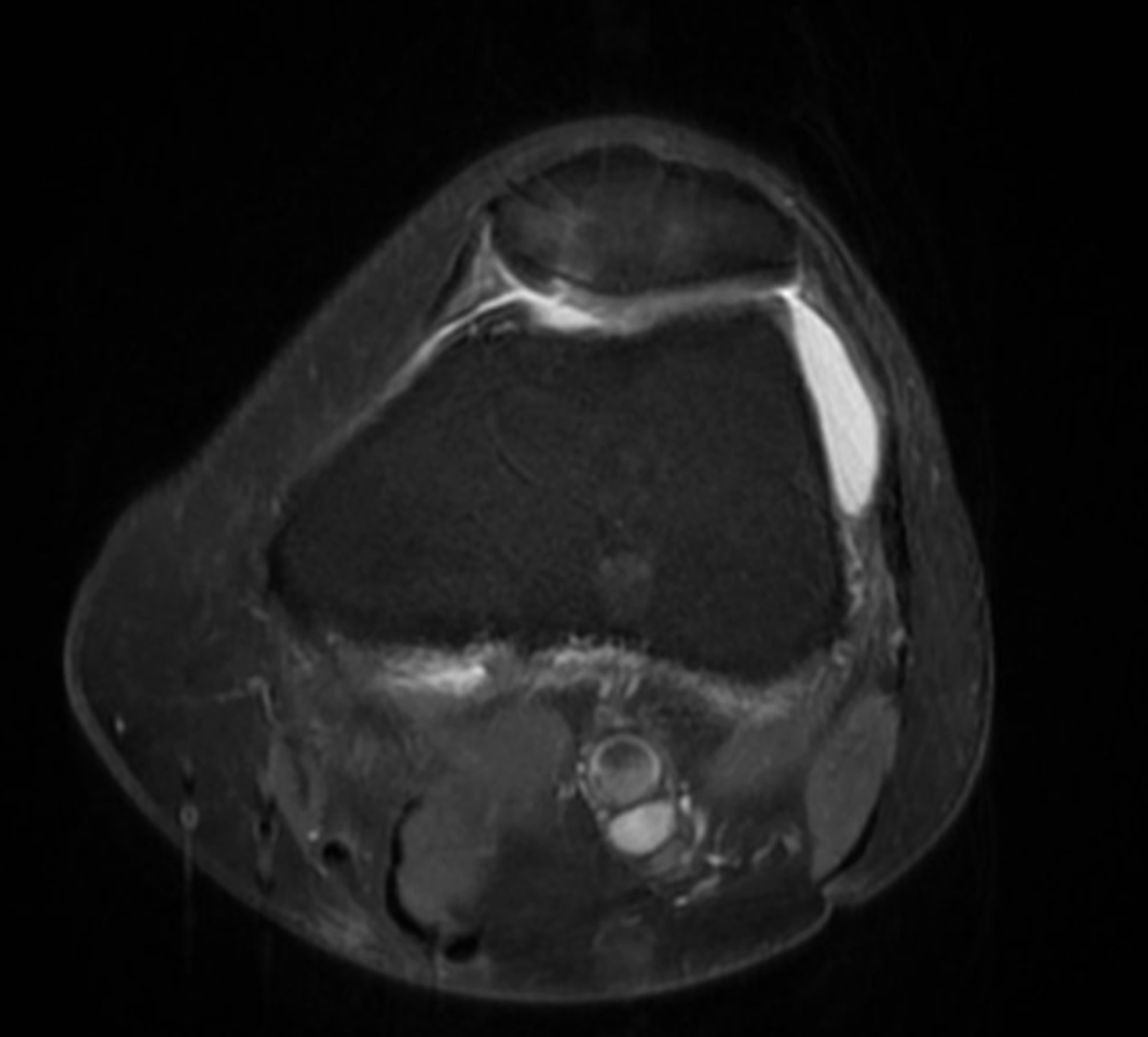
Case study: A sordid little story of anterior knee pain, manual therapy and K-tape..with consent.
60yo patient presents with 6 months of worsening anterior knee pain and swelling. Pain at rest. Worse with with stairs and rising from chairs. Unable to jog or play singles tennis (which is central to her social life). Had been told her weak glutes were the cause; had been given glute strengthening; she felt it was making things worse.
MRI: Chondral fissuring of medial facet, Full thickness cartilage loss inferior patella, superolateral fat pad inflammation, effusion...aka anterior knee pain/PFPS/PFJ OA.
After >4 years, Covid delays, 3 linked manuscripts, & several rounds of revisions, our Best Practice Guide is finally online first in @BJSM_BMJ.
Thanks to @simonthephysio, @iamclarebart, & @DrDylanM for their perseverance!
Check it out ⬇️⬇️
https://t.co/ZCWOB5axNv
'Tackling health inequalities: seven priorities for the #NHS' @TheKingsFund
https://t.co/qOoa6EZHck
#HealthInequalities are "avoidable, unfair and systematic differences in health experiences and outcomes"
We are pleased to announce the publication of a BOA Standard (BOASt) on Mobilisation and weightbearing after orthopaedic surgery / musculoskeletal injury. This BOASt was jointly produced by BOA and several stakeholder contributors. Please read and share: https://t.co/h85KueLjtN
Discover what is necessary for effective dental record keeping, to ensure you’re putting your patients’ interests first, in our latest blog post by Shamir B. Mehta, Senior Clinical Dental Adviser at the GDC.
https://t.co/5IlcQPqQfO
#Dentistry#DentalRecords
It's nice to be honoured in the Pro Bono Recognition List of England & Wales 2024 & it was lovely to receive a congratulatory email from The Lady Chief Justice. There are many lawyers on the list "following the long tradition of the legal profession in volunteering their time to provide free legal assistance to individuals & charities". Well done everyone! I do feel it's an absolute privilege to have a skill which can be put to good use for the benefit of others.
https://t.co/B3GuzNI4f4