Surgeons — using Netter on your slides or social posts? That's a copyright violation.
Here are 6 FREE sources you can actually use legally:
🔵 Open-i (NLM) — 3.7M images, 2,000+ ortho illustrations
🟢 USC Ortho Collection — 1,900+ dissection photos (CC licence)
🟡 HEAL / Utah — 22,000 health ed materials
🟣 BioRender — publication-quality figures (free tier)
🟠 NIH BioArt — 2,000+ vectors, public domain
🟩 InjuryMap — anatomy diagrams for posts & blogs
Bookmark this. Share it with a colleague who needs it.
#Orthopaedics #MedTwitter #SurgicalEducation #TheArmDoc
👨🏼⚕️ El doctor Roberto Sánchez Rosales explica en este vídeo cómo realiza una sutura intratendinosa. Y es que, las lesiones en los tendones flexores pueden ser las que más se complican en cirugía de la mano.
No te pierdas la lección completa aquí: https://t.co/530cpBZPXK
ohhh hell yeahhh !!
In final prototype testing phase on https://t.co/1WvAMhHtn0
Not for public use yet, but im pretty sure you'll find this as cool as I do!
post a random sketch and ill test run it, and we'll see how it goes !!
#orthotwitter#medtwitter
@JMGardnerMD Intriguing case, @JMGardnerMD! The expansile intramedullary bone lesion you've shared could be associated with several syndromes. One possibility is Jaffe-Campanacci syndrome, linked to mutations in the BRAF gene.
"Treatment of Proximal Trans-ulnar Fracture-Dislocations Based on a Step-By-Step Coronoid-Centric Surgical Technique" by Blonna et al.
Read online at https://t.co/lu2zs8YYRr
Most shoulder X-ray misses happen before interpretation even starts.
Know your landmarks:
Humeral head centered on glenoid
Acromiohumeral interval: 7-12mm
AC distance: under 8mm
CC distance: under 13mm
AP view. Scapular Y view. Trace every cortex. Review the lung apex.
The systematic approach is everything.
#ShoulderSurgery #Orthopedics #MedEd
A quick look on posterior glenohumeral joint injection technique.
To access full video, start your 14-day free trial at https://t.co/HzbdPPtCGu
#orthopaedics#ShoulderjointInjection#meded
Supplementation with Vitamin D or calcium, or both does not help prevent fractures or falls. From a new systematic review of 69 randomized trials and >150,000 participants
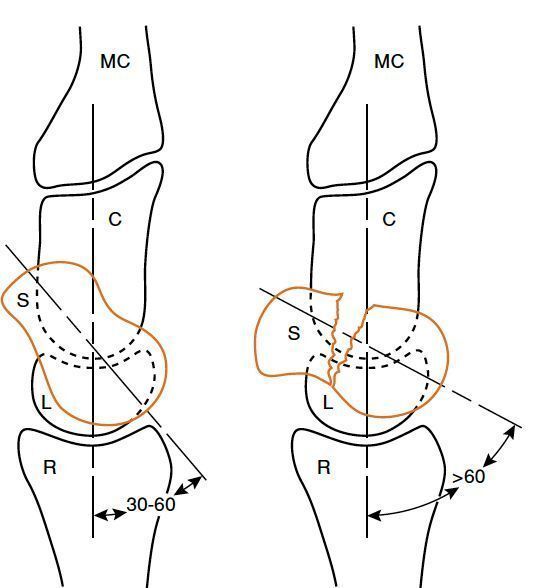
A, Normal scapholunate angle (SL) is 30 to 60 degrees. A normal capitolunate angle (CL) is (0±15) degrees. B, Displaced scaphoid fracture leads to dorsal intercalated segmental
instability (SL angle >60 degrees) through internal angulation and humpback deformity. C, Capitate; MC, metacarpal; L, lunate; R, radius; S, scaphoid.