7-year PFS of 55% with lorlatinib is truly remarkable—arguably a new benchmark for targeted therapy in solid tumors.
Other solid-tumor benchmarks across modalities include:
Cytotoxic chemotherapy: BEP in testicular cancer — 5-year PFS ~90% in good-risk and 40~50% in poor-risk disease
ADC: Trastuzumab deruxtecan in HER2+ breast cancer — 2L median PFS ~29 months
Immunotherapy: Nivolumab + ipilimumab in dMMR/MSI-H mCRC — 4-year PFS ~65%
Together, these examples remind us that with precise patient selection and continued optimization of existing drug modalities, transformative long-term disease control is still achievable in solid tumors.
#ASCO26 @ASCO@OncoAlert@oncodaily
Newest #ASCO26 example: NEXUS-01.
Post-EV urothelial carcinoma treated with LY4052031 — anti–Nectin-4 ADC, TOP1i payload — showed encouraging activity, ORR ~33%.
Another signal for the ADC sequencing rule:
Same target, different payload → opportunity
Different target, same payload → limited help
Payload resistance may be the key.
By the same logic, given the current dominance of TROP2–TOP1i ADCs, emerging TROP2–MMAE strategies such as LCB84 (NCT05941507) may be worth watching.
@ASCO@OncoAlert@oncodaily #ADC
ADC sequencing is entering a new phase.
At ESMO BC 2026, two prospective datasets raised an important caution:
1️⃣ SATEEN: trastuzumab + sacituzumab govitecan after prior T-DXd in HER2+ MBC
ORR: 3.7% — only 1/27 confirmed response
2️⃣ HER3-DXd after prior TOP1-ADC exposure, including T-DXd, Dato-DXd and/or SG
ORR: ~5% in both HR+/HER2– breast cancer and TNBC cohorts
Different targets, similar TOP1 payload backbone — and very limited activity.
These data strongly suggest that in many patients, ADC resistance may be driven more by payload-associated resistance than by antigen selection alone.
This also fits the opposite clinical observation: when the payload changes, activity can still be meaningful — for example, T-DXd after T-DM1, or FRα-TOP1 ADC strategies after mirvetuximab soravtansine in ovarian cancer.
The ADC field is still heavily concentrated around two payload classes:
• TOP1 inhibitors
• anti-microtubule agents
Soon, many chemo-sensitive cancers may have one TOP1-based ADC and one microtubule-based ADC, often with the earlier-line ADC combined with anti-PD-1/PD-L1.
That may already improve survival substantially.
But to unlock the next level of benefit, we need more diversified ADC payloads — especially payloads that induce immunogenic cell death or other mechanisms that synergize with immunotherapy.
@myESMO@oncodaily@OncoAlert
A warmup before ASCO: The rapid pace of oncology innovation is completely outstripping trial design.
With the major NEJM publication of the HERIZON-GEA-01 trial, a new Standard of Care (SOC) emerges: Zanidatamab + tislelizumab + chemo wins in the ITT population, regardless of PD-L1 status.https://t.co/ihKvD3BbM4
But this creates a fascinating clinical & regulatory bottleneck:
🔹 ToGA (Trastuzumab + Chemo) was the benchmark for a decade.
🔹 KEYNOTE-811 advanced the needle but primarily for the PD-L1+ subgroup.
🔹 HERIZON-GEA-01 splits the 1L landscape wide open.
Now, ongoing trials like ARTEMIDE-Gastric01 and DESTINY-Gastric05 are using KEYNOTE-811 as their control arms. How will we cross-compare them to a Zanidatamab-based triplet? And what about future branches from HERIZON-GEA-01?
As our "treatment tree" (figure generated by GEMINI) sprouts new branches at an unprecedented speed, selecting the right 1L SOC (and subsequent 2L sequence) becomes highly fragmented. This same phenomenon is playing out in EGFRm NSCLC (MARIPOSA vs. FLAURA-2).
Advancing the field? Absolutely. Navigating it? It's going to take collective wisdom from investigators, pharma, and regulatory agencies.
#OncoTwitter @OncoDailyGI@oncodaily #GIonc #DrugDevelopment
I have been so impressed by the recent Daraxonrasib data that I forgot the 25 year anniversary of the precision medicine OG - STI571 (Gleevec). What a triumph of modern medicine. And congratulations to @MelDMann - still going strong all these years later!
https://t.co/Infk3Ov7Pn
ADC sequencing is entering a new phase.
At ESMO BC 2026, two prospective datasets raised an important caution:
1️⃣ SATEEN: trastuzumab + sacituzumab govitecan after prior T-DXd in HER2+ MBC
ORR: 3.7% — only 1/27 confirmed response
2️⃣ HER3-DXd after prior TOP1-ADC exposure, including T-DXd, Dato-DXd and/or SG
ORR: ~5% in both HR+/HER2– breast cancer and TNBC cohorts
Different targets, similar TOP1 payload backbone — and very limited activity.
These data strongly suggest that in many patients, ADC resistance may be driven more by payload-associated resistance than by antigen selection alone.
This also fits the opposite clinical observation: when the payload changes, activity can still be meaningful — for example, T-DXd after T-DM1, or FRα-TOP1 ADC strategies after mirvetuximab soravtansine in ovarian cancer.
The ADC field is still heavily concentrated around two payload classes:
• TOP1 inhibitors
• anti-microtubule agents
Soon, many chemo-sensitive cancers may have one TOP1-based ADC and one microtubule-based ADC, often with the earlier-line ADC combined with anti-PD-1/PD-L1.
That may already improve survival substantially.
But to unlock the next level of benefit, we need more diversified ADC payloads — especially payloads that induce immunogenic cell death or other mechanisms that synergize with immunotherapy.
@myESMO@oncodaily@OncoAlert
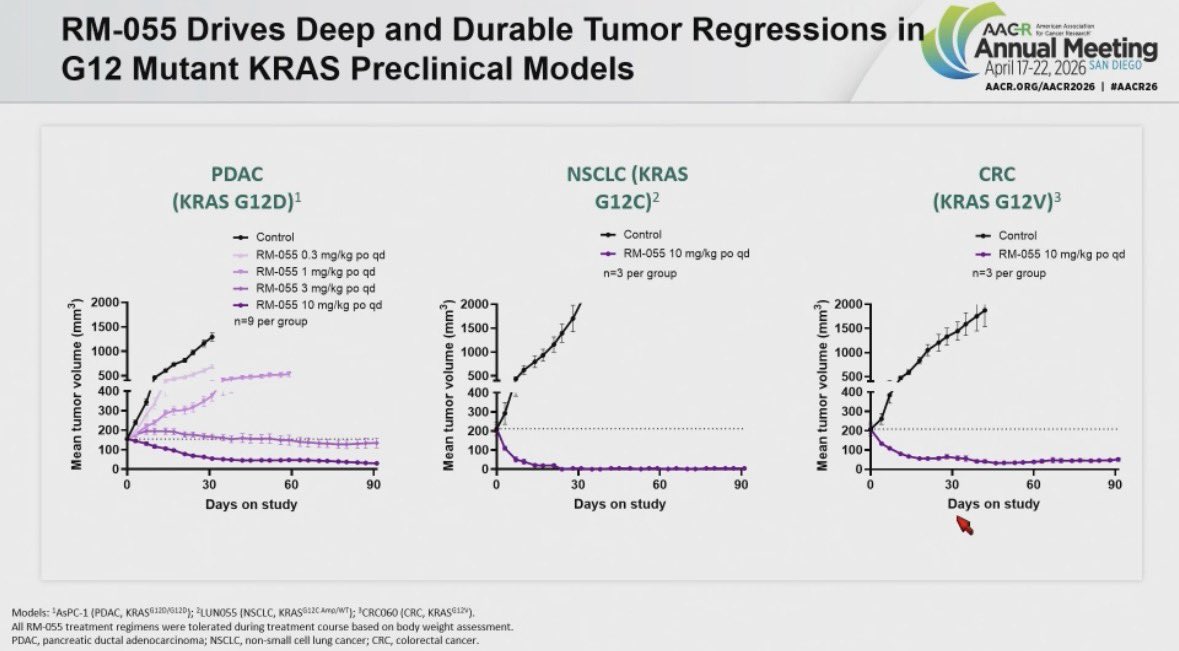
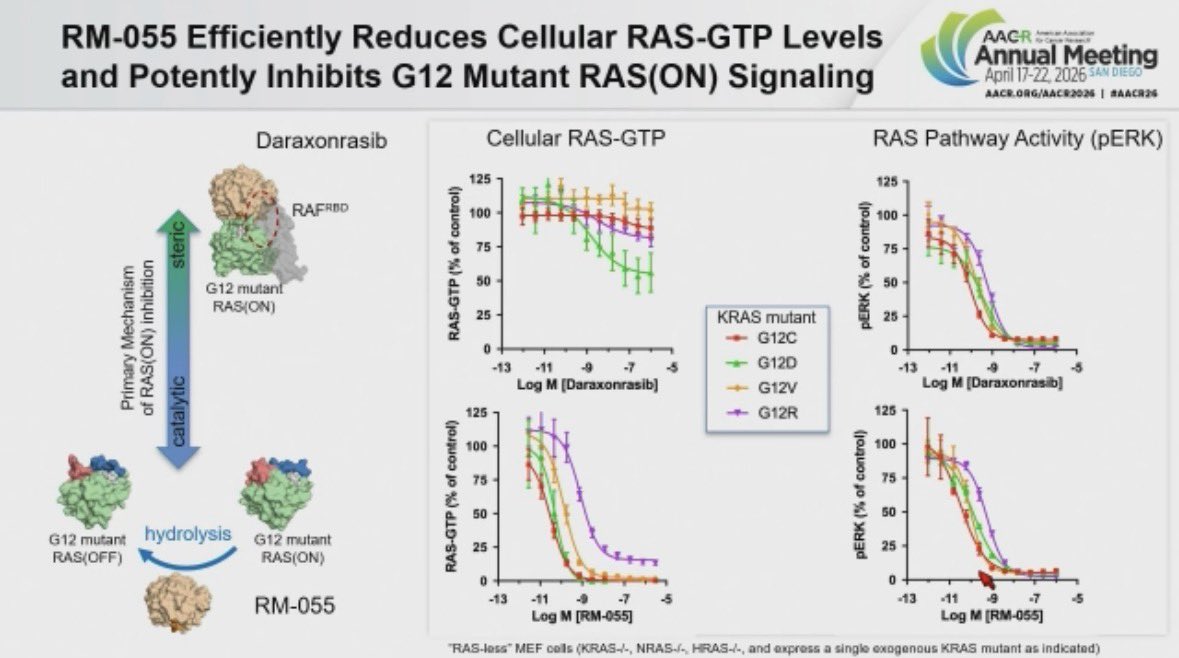
Promising next-generation CYPA-complex RAS inhibitor RM-055 is coming. It appears to overcome daraxonrasib resistance while showing better selectivity over WT RAS. But it also seems G12X-specific, raising an important question: will secondary non-G12X RAS mutations emerge as a resistance mechanism, and will combination with a pan-RAS inhibitor be needed to prevent or delay this? #AACR26 @RevMedicines@KRASKickers
New compound from @RevMedicines RM-055 disclosed at #AACR26
They took a subtle finding 👉🏽Daraxonrasib-CYPA complex modestly increasing RAS GTP hydrolysis 👉🏽 to build a RAS GAP on steroids. RM-055 flattens Daraxonrasib resistant tumors including RAS amplified cases across models.
An interesting proposal. However, IMHO, it may be challenging to omit the immune checkpoint inhibitor component in the 1L and perioperative settings, given that KRAS-mutant NSCLC is relatively sensitive to ICIs and that a subset of patients can achieve durable disease control. Notably, essentially all ongoing phase 3 trials in these settings incorporate ICIs, with the exception of the sotorasib study, which is focused on PD-L1–negative patients and whose design was likely influenced by the hepatotoxicity seen with the sotorasib–ICI combination.
A striking coincidence to have had RVMD present at the 12th A-TOPIC (Asia Oncology Phase I Trials Conference) yesterday.
Daraxonrasib vs chemotherapy in 2L PDAC:
OS 13.2 vs 6.7 months
HR 0.40, p<0.0001
A PARADIGM SHIFT.
This may represent the biggest advance in oncology since anti-PD-1 therapy, and perhaps the greatest improvement ever seen in GI oncology.
This could create substantial opportunities for combination strategies: chemotherapy, allele-specific RAS inhibitors, PRMT5 inhibitors, anti-EGFR/other RTK-directed agents, and future p53 reactivators, with possible movement into adjuvant/neoadjuvant settings.
Also watching with interest the clinical-stage tri-complex inhibitors ERAS-0015, BPI-572270, and GFH276.
Will tri-complex inhibitors and newer SIIP inhibitors with ON-state activity show non-overlapping resistance patterns?
@myESMO@oncoalert #oncotwitter #PDAC
Malaysian early phase researcher Dr Voon Pei Jye (Sarawak General Hospital) continue to make waves by taking the stage this weekend at the 12th Asia Oncology Phase 1 Trials Conference (A-TOPIC) in Taiwan. The conference gathers early phase researchers within the region, sharing insights of innovative drug developments in cancer.
The @IASLC MCSC & ART has just published the practical approach for unresctable LA-NSCLC in @JTOonline! We provides 5 cases representing challenging scenarios for multidisciplinary discussion, inspiring best care for thoracic tumor boards.
Read more 👉 https://t.co/sW0BThq5AK
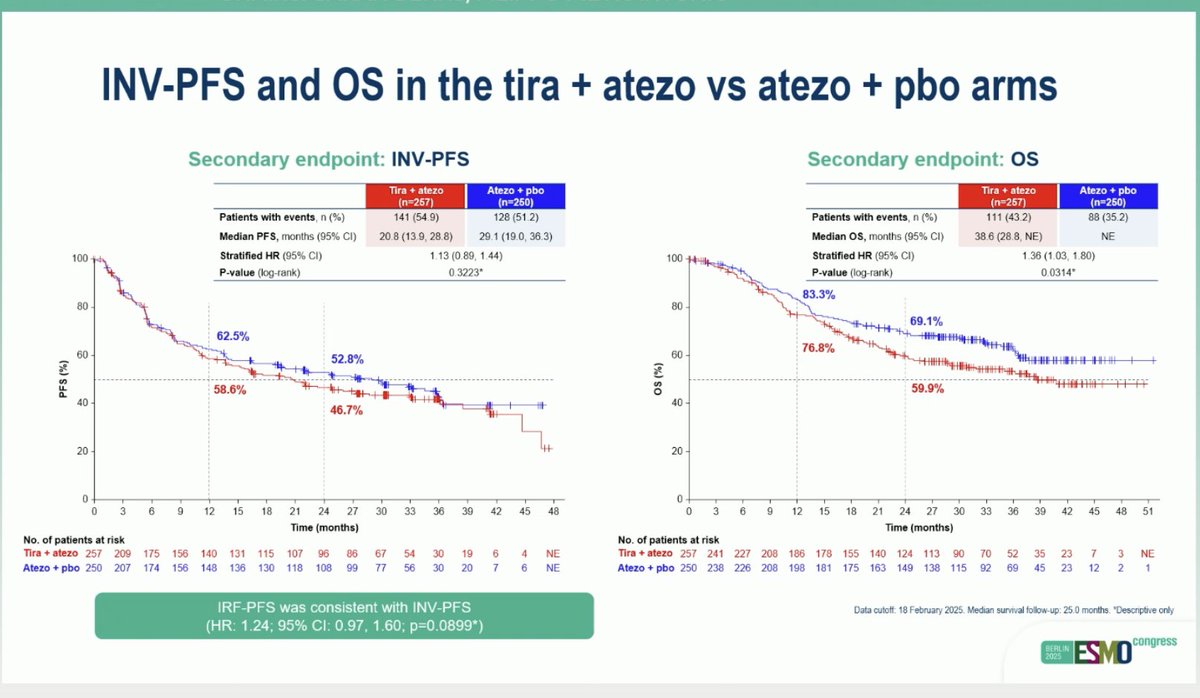
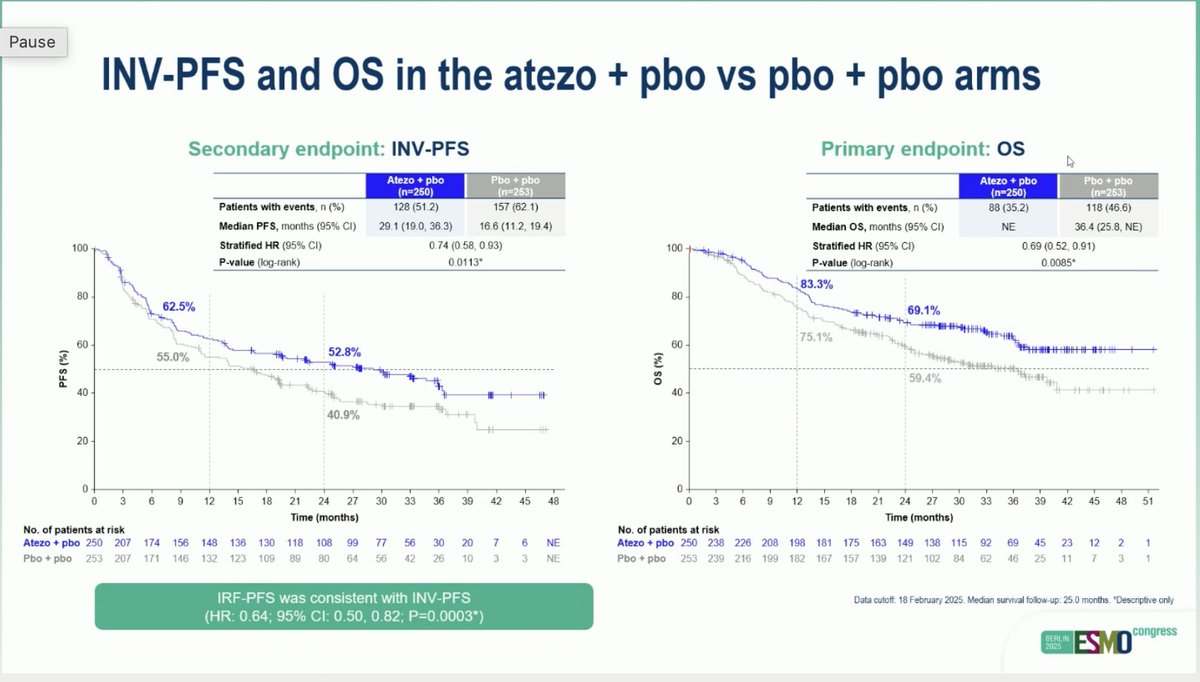
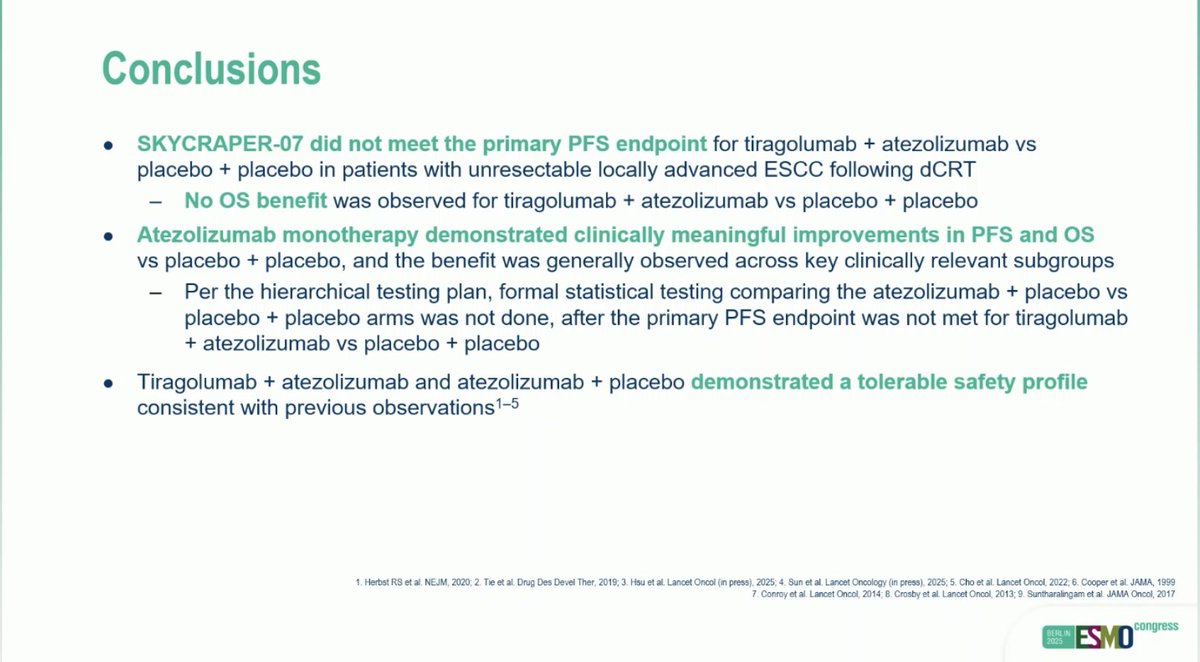
SKYSCRAPER-07: Phase III study of atezo with or without tiragolumab in unresectable ESCC that has not progressed following dCRT
#ESMO25#ESMOAmbassadors
👉 mPFS: 29 vs 20.8 vs 16.6
👉 mOS: n.r. vs 38 vs 36 mo
🧐Atezo improves outcome, but adding tiragolumab to atezo with detrimental effect
@myesmo
IMvigor011: Adjuvant atezolizumab for MIBC patients with postoperative ctDNA+ → Positive for DFS & OS.https://t.co/4b9abM75Rn
A fightback after IMvigor010 all-comer approach.
Given NIAGARA & positive EV303 (and highly anticipated EV304), adjuvant atezo may not be mainstream—yet highlights potential adaptive strategies, e.g. de-escalation after neoadjuvant if ctDNA–.
In solid tumors, MRD-guided treatment warrants pan-cancer exploration!
#BladderCancer #MIBC #ctDNA #MRD #Immunotherapy #Atezolizumab #Oncology #CancerResearch #GUonc #ClinicalTrials @myESMO@OncoAlert