9/ We have loved working on this and learnt so much. Thank you to the amazing Nick Williams! To all the team, Joe Lee, @luiza_moore, Anna Godfrey. To Peter Campbell and Tony Green. Our funders @CR_UK@mpnrf@EHA_Hematology and our dear patients.
8/ Importantly, the rate of expansion of mutant-JAK2 predicted the time to MPN diagnosis..... a possibility of early detection and disease prediction? #stopcancer
7/ Clone growth rates varied: <10%/yr to >200%/yr for multiply mutated clones. #JAK2V617F clones grew at different rates in different individuals - ie patient-specific factors (germline, environment) influence its consequences as shown by @bloodgenes lab and others.
5/ We found in utero and childhood acquisition of DNMT3A mutations too. In one patient, the #DNMT3A mutation was acquired within few weeks of conception – the start of life. Ageing per se didn’t drive such clonal haematopoiesis – it simply took an age for the clones to grow.
4/ JAK2 mutations were acquired early in life - in utero and childhood despite a diagnosis many decades later, up to 54 years before MPN diagnosis for one patient #JAK2V617F
3/ We used DNA mutations to trace the ancestral relationships between colonies - building a "family tree" of blood production for each patient. We could then time the cancer driving genetic events and trace how the mutant clones expanded over the patient’s life.
2/ We took single blood cells from patients with MPN and grew each cell into a colony. We then sequenced each colony's whole genome (>950 whole genomes).
1/ "How long have I had it for?"
Our patients with #bloodcancer have always wanted to know. We set out to answer it. We studied patients with MPN #mpnsm and found quite unexpected results. Excited to share our preprint https://t.co/elOrvlUIjL
🔐Use of in situ simulation to evaluate the operational readiness of a high‐consequence infectious disease intensive care unit.
This excellent paper from @TajFregene, @jambuc33 and @v_alien is #FOAMed forever!
🔗https://t.co/w9TKS8ByMb
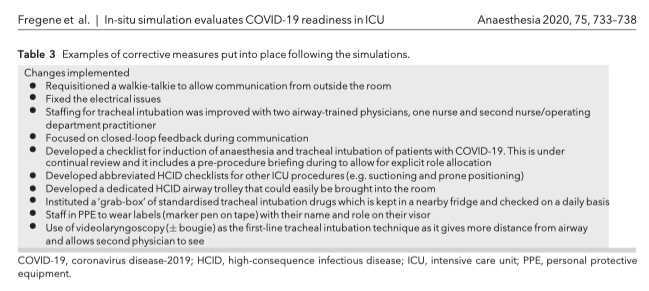
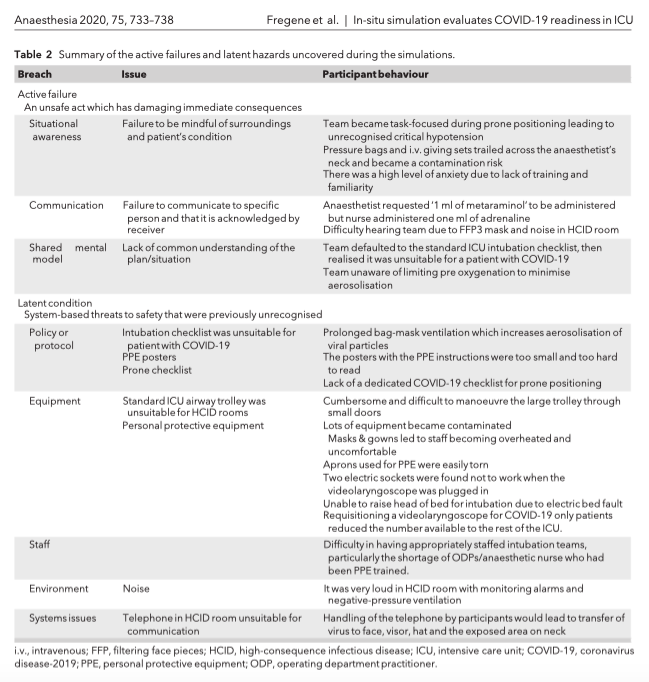
🔐"The problems identified encompassed aspects of operational readiness of the ICU for admission of patients with COVID‐19. These included staff preparedness, equipment shortages and lack of tailored guidelines."
@TajFregene @jambuc33
@v_alien
🔗https://t.co/w9TKS8jXUD
🔐This new in situ simulation study from @TajFregene, @jambuc33 and @v_alien shows how multiple operational deficiencies were found and corrected before the admission of the first patient with COVID-19 at high-consequence infectious disease ICU.
🔗https://t.co/w9TKS8ByMb