Are you looking for real-life examples and use cases of generative AI in healthcare?
This website comes up with such lists of relevant examples with detailed descriptions.
You will find stories about using generative AI to create new medical images or to detect fraud, among many others.
Here is the list: https://t.co/XpuZorlzzv
Artificial intelligence–based retinal imaging for brain health assessment: a scoping review - The Lancet Digital Health https://t.co/e9SfCwLh43
The future of medical care
I agree with @EricTopol. Average waist “diameter “ of an average man is 23cm. Maximum depth of penetration of of the available US technology now is 15-30cm. In this Midjourney model people are submerged in a hot tub to provide water medium for US wave travel. Air is a poor conductor. Water is poorer conductor than jelly. In the described model it’s a dome like a CAT Scan. With a maximum 30cm penetration, I don’t know how much images we can see. They can use video game technology and recreate an image, but I’m not sure how much it is medically reliable. Let’s see
AI of radiologist read as normal mammograms shown to detect high-risk of breast cancer out several years
"Artificial intelligence scores from sequential
mammograms in individuals diagnosed with breast cancer showed elevated scores up to 10 years before diagnosis"
a retrospective study, but supported by prospective study in 3-5 year time horizon
https://t.co/NafnAkpEfo
https://t.co/ead144H2XW
I’m a cardiac surgeon. I agree that CAC Zero score is not a Green light for good heart health. Plaque vulnerability of rupture is the highest risk. In fact calcified plaques (identified by CAC Score) are more stable than a soft plaque. In near future we will be looking for more quality of the plaque more than stenosis of the lumen. Soon AI guided CTA coronary angiogram will be first line of test before any stress test.
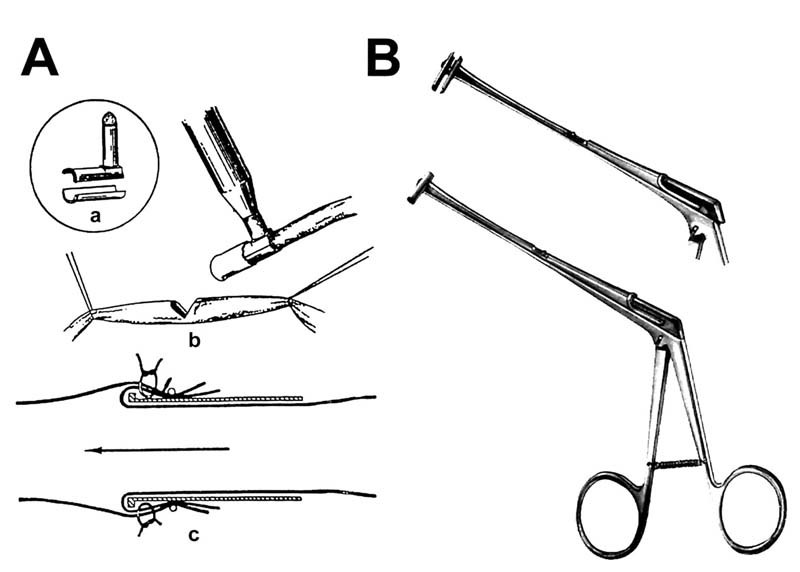
This book is a remarkable landmark of an early work on coronary bypass surgery. For details on Kolesov life and work, read free online.
Konstantinov IE. Vasilii I Kolesov: a surgeon to remember. Tex Heart Inst J. 2004. PMID: 15745284
https://t.co/jxX8BVaDdU
🫀⚡ CCTA is no longer “just a test.” It is becoming the operating system of modern cardiology.
This review makes something very clear: Coronary CT has crossed a threshold.
It is no longer simply about detecting stenosis.
It is now integrating:
👉 anatomy
👉 physiology
👉 plaque biology
👉 inflammation
👉 procedural planning
👉 AI-driven prediction
—all inside one examination.
For years, cardiac imaging was fragmented:
- stress test for ischemia
- angiography for anatomy
- IVUS/OCT for plaque
- separate risk scores for prognosis
Now CCTA is starting to merge all of these layers together.
The paradigm shift is obvious
From: ❌ “Is there obstructive CAD?”
To: 👉 “What is the biological trajectory of this patient?”
The paper highlights how modern CCTA now provides:
✅ plaque characterization
✅ quantitative plaque burden
✅ CT-FFR
✅ PCAT inflammatory analysis
✅ radiomics
✅ AI-driven phenotyping
And Photon Counting CT accelerates everything.
Because PCCT is solving one of the oldest problems in coronary imaging:
👉 blooming
👉 limited spatial resolution
👉 poor stent evaluation
👉 calcium interference
With PCCT:
⚡ spatial resolution approaches ~0.25 mm
⚡ calcium blooming is dramatically reduced
⚡ stent lumen visualization improves substantially
But here’s the deeper implication
We are moving away from: ❌ lumen-centric cardiology
toward: 👉 multi-dimensional atherosclerosis phenotyping
And AI becomes critical here.
Not because it “replaces” physicians.
But because humans cannot realistically integrate:
✅ plaque texture
✅ morphology
✅ inflammation
✅ radiomics
✅ flow dynamics
✅ longitudinal progression
at scale.
My take
The future cardiac CT exam will not answer:
👉 “Is there a stenosis?”
It will answer:
👉 “How dangerous is this artery biologically?”
👉 “How will this patient evolve?”
👉 “Which therapy changes the trajectory most?”
Bottom line
CCTA is evolving from:
👉 diagnostic imaging
to:
👉 computational cardiovascular phenotyping
⚡ And once imaging becomes biology + AI + prediction…
the entire architecture of cardiology changes.
#CCTA #Cardiology #PhotonCounting #AI #PrecisionMedicine #Atherosclerosis #CardiacCT #PlaqueImaging #yesCCT
My boss's boss is like 42, never married, no kids. Earns $275-300K per year. Goes on a minimum of two international vacations a year w/ his girlfriend. 10+ days, all out.
Eats the best food, stays in top notch accomodations. Excursions, tours, nicest beaches, etc.
Great guy, I'm happy for him.
But what I've realized is that without kids, you end up chasing a lifestyle that has to continually be topped in order for you to be satisfied and find happiness.
What he and others like him don't understand is that when you have children, seeing THEM experience life's most basic things and watching their eyes light up at all the "firsts", brings greater pleasure and joy than any vacation or travel experience ever could.
Seeing THEM try blueberries for the first time is greater than dining at the best 5 star restaurant in Europe.
Seeing THEM learn how to walk is greater than walking the Great Wall of China or strolling along the most picturesque beach.
Watching THEM giggle uncontrollably at "peek-a-boo" tops any A-list comedian act.
Seeing THEIR excitement when building a fort out of cardboard boxes and making a door big enough for daddy is superior to staying at 5-star resorts.
Flying kites with THEM far outweighs excursions like parasailing or helicopter rides.
Seeing THEM perform a recital on stage for the first time is more rewarding than watching a Broadway show or top notch symphony orchestra.
-----------------
When you have children, all of a sudden you realize that life's greatest joys are not in the pursuit of things or pleasure or travel, but rather in the LOVE and bond you share with your very own image bearers.
Seeing the beauty and magnificence and wonder of life all over again for the first time through THEIR eyes and expressions gives you something the world simply cannot offer, nor even come close.
☝️Respectfully disagree
👉Inflammation is not the “missing piece” in coronary disease—it is a secondary response, not the primary driver.
1️⃣ The causal pathway is already well established: apoB-containing lipoprotein retention initiates atherosclerosis; inflammation follows.
2️⃣ Decades of trials targeting inflammation have largely underdelivered, with inconsistent or null effects on hard cardiovascular outcomes.
3️⃣ Even when inflammation is reduced (e.g., CRP lowering), clinical benefit is absent or marginal—hardly a compelling therapeutic target.
4️⃣ The concept of “residual inflammatory risk” is conceptually attractive, but clinically weak; many patients with events have low CRP levels.
5️⃣ We are mistaking timing for mechanism: treating end-stage disease and blaming inflammation for failure is a convenient but flawed narrative.
6️⃣ The real problem is cumulative exposure to apoB over decades—still insufficiently addressed in most patients.
7️⃣ Shifting focus toward inflammation risks diluting efforts from what actually works: early, intensive, and sustained lipid lowering.
☝️In short: inflammation matters biologically—but as a therapeutic target, it remains an underperforming hypothesis.
@society_eas@nationallipid@Drlipid
When using 3DVUS to look inside the arteries of young people, 88% of those whose plaque progressed had a calcium score of 0. In those whose plaque progressed, the percentage that still had a CAC of 0 was still 76%. This shows us again that CAC is a much later stage finding. You can have plenty of soft plaque without calcium.
The study also showed that those whose disease progressed were the oldest and those with the highest LDL-C.
https://t.co/emuWLRjPpB
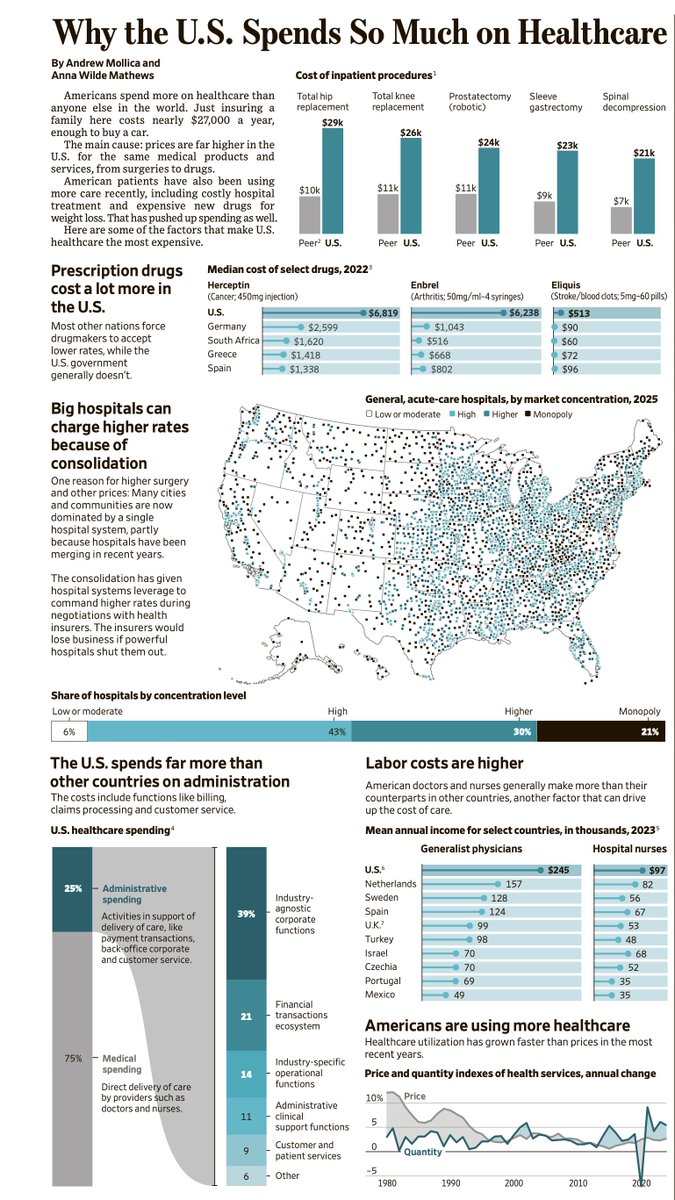
The multitude of ways that jack up American healthcare costs (without improving outcomes)
@armollica@WSJGraphics@annawmathews
gift link https://t.co/FjseZsYQiT
Most of the Heart Attacks are due to Plaque rupture from unstable plaque and not from severe stenosis. High LDL Cholesterol is the main culprit. Aim for <55mg of LDL C