Day 3 #ASCO26 5 plenary highlights:
1. #PROTEUS: PeriOp/PostOp Apa in Prostate Ca
2. #SARC041: Adj Abema in dediff liposarcoma
3. #LIBRETTO432 : Adj Selpercatinib in NSCLC
4. #HARMONi6: 1L Ivonescimab in Sq mNSCLC
5. #RASolute302: 2L Daraxonrasib in Panc Ca
@ASCO
1/6
I put together a free guide on using AI the right way in medicine. How to use it as a teacher. Where the ethical line is. 45+ research databases. Formal AI courses from AMA, AAMC, Harvard, Stanford. For medical students, IMGs, residents, and fellows:
https://t.co/DomyhcVGfC
JUST IN: The report we always look for every year: CANCER STATISTICS, 2026
New milestone with 5y Survival of 70%!!! Still a lot of room to improve but also excellent progress !
@AmericanCancer@CACancerJournal@DanaFarber
https://t.co/ZtFDhFOGgU
Treatment of Multiple Myeloma: ASCO–Ontario Health (Cancer Care Ontario) Living Guideline | Journal of Clinical Oncology
@JCO_ASCO@ASCO#mmsm
➡️ https://t.co/6kjOw29B6W
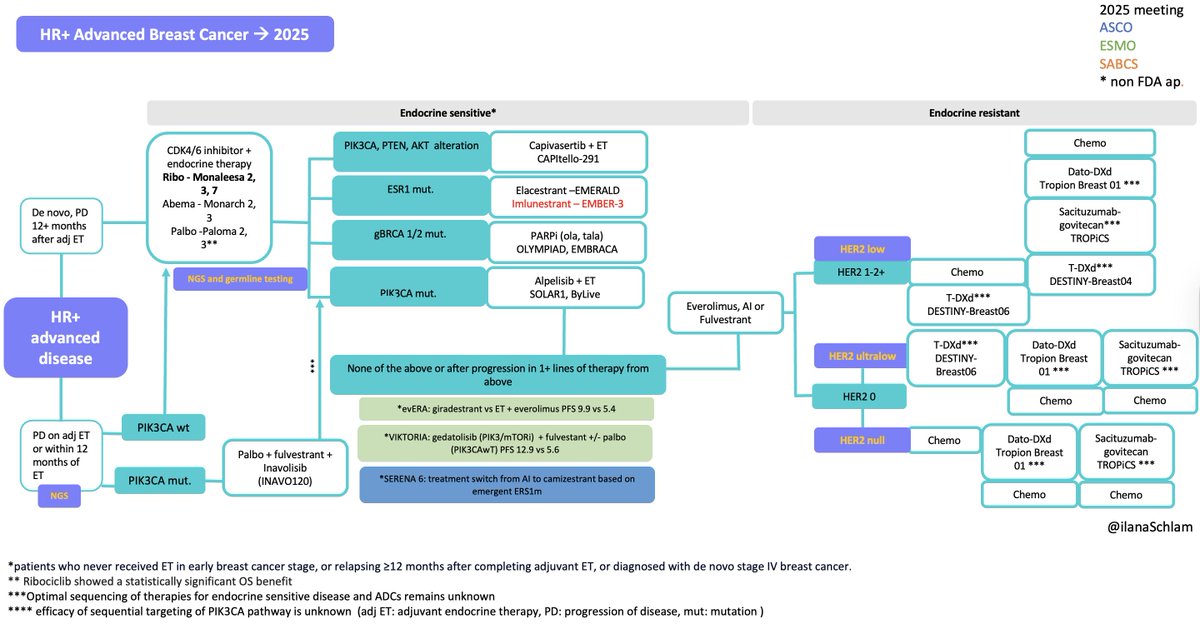
This slide perfectly illustrates the paradox of modern HR+ metastatic breast cancer management.
On paper, the post–CDK4/6 landscape is elegant and biologically rational: NGS-guided decisions, ESR1-targeted oral SERDs, PI3K/AKT pathway inhibitors, PARP inhibitors, and even CDK4/6 continuation strategies. Almost every resistance mechanism has a proposed solution.
In real life, however—in many countries, including my own—most of these red-highlighted options are simply not accessible. The algorithm exists, the evidence exists, the biomarkers exist… but the treatments do not.
So the question is unavoidable: who is this progress really for?
If we cannot deliver these drugs to patients, daily discussions about ever-expanding therapeutic menus risk becoming purely theoretical exercises.
Theoretical knowledge alone is not enough; translating it into practice is essential, but this is unfortunately not in the hands of physicians. It is a global problem.
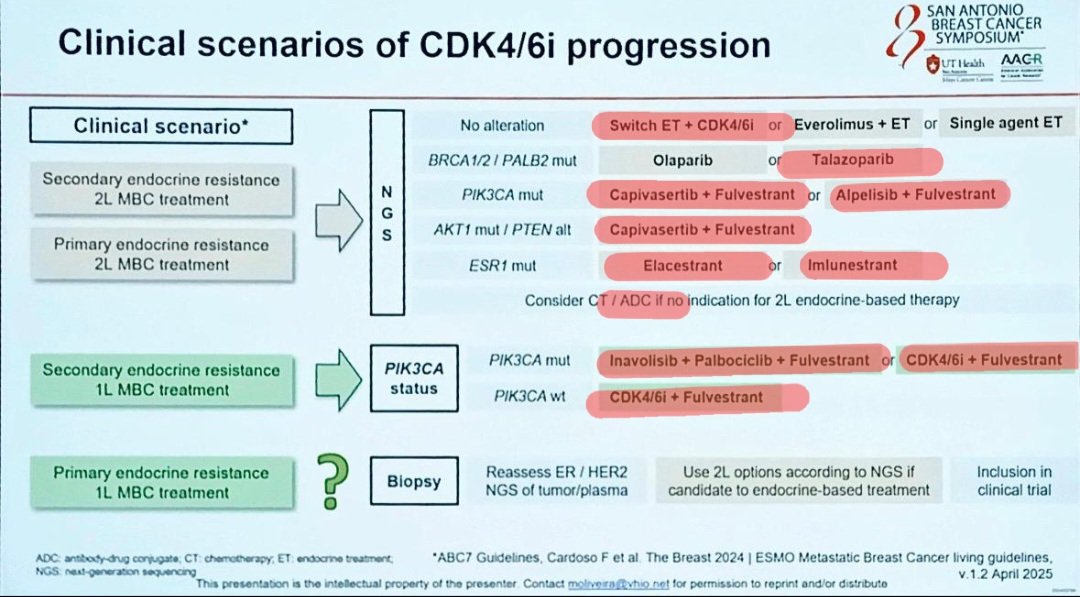
So, where were we? What were we supposed to give patients with ESR1 mutations, those with PIK3CA alterations, and those with co-mutations? And then the questions keep coming: what if the DFI is less than 12 months? If ctDNA turns positive before radiologic progression—was that SERENA-6 or PADA-1?
After every conference, I find myself trapped in this paradox. Hopefully, one day everyone will have fair access to the treatments they deserve. Wishing you a nice weekend—it was a good conference. #SABCS25
Management of Cancer During Pregnancy: ASCO Guideline
It is a remarkably comprehensive guide that addresses every question thoroughly👇
https://t.co/NXtQjTcsIb
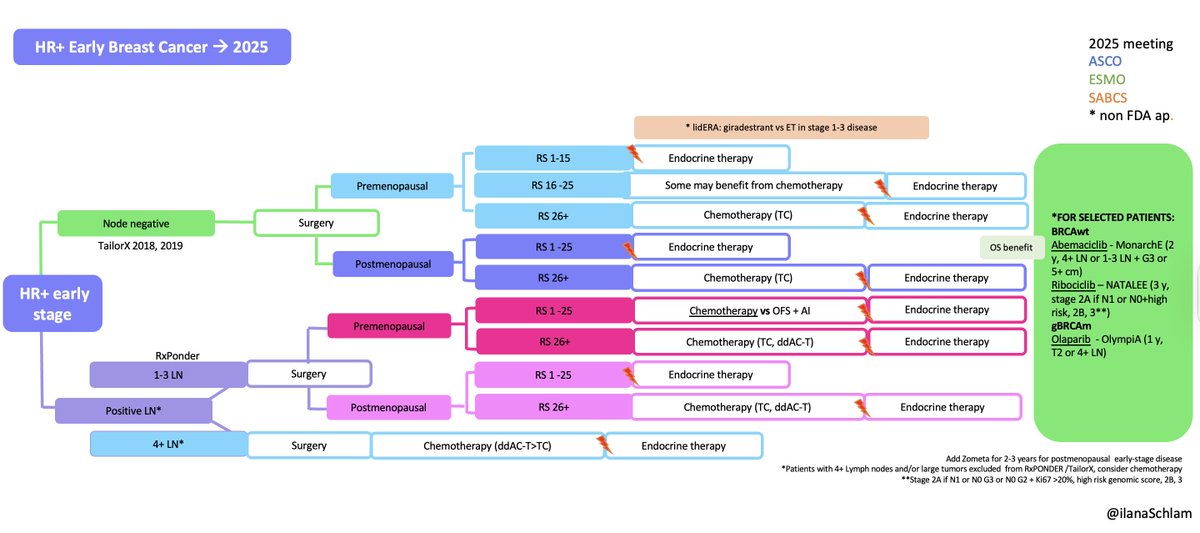
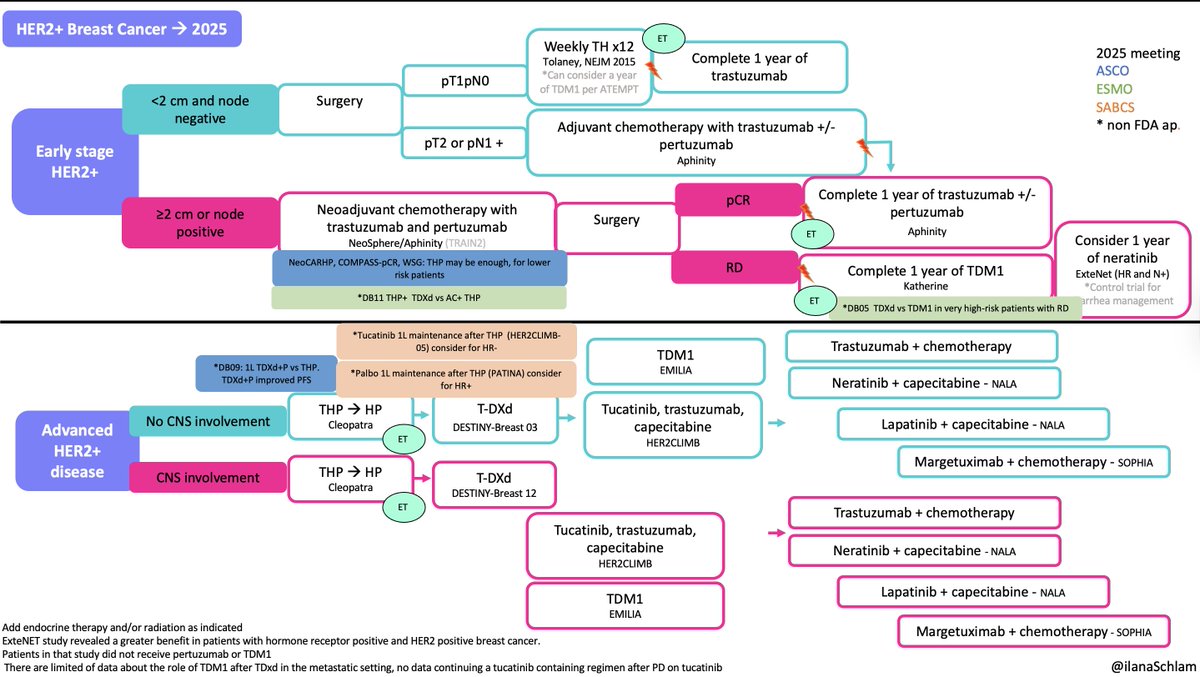
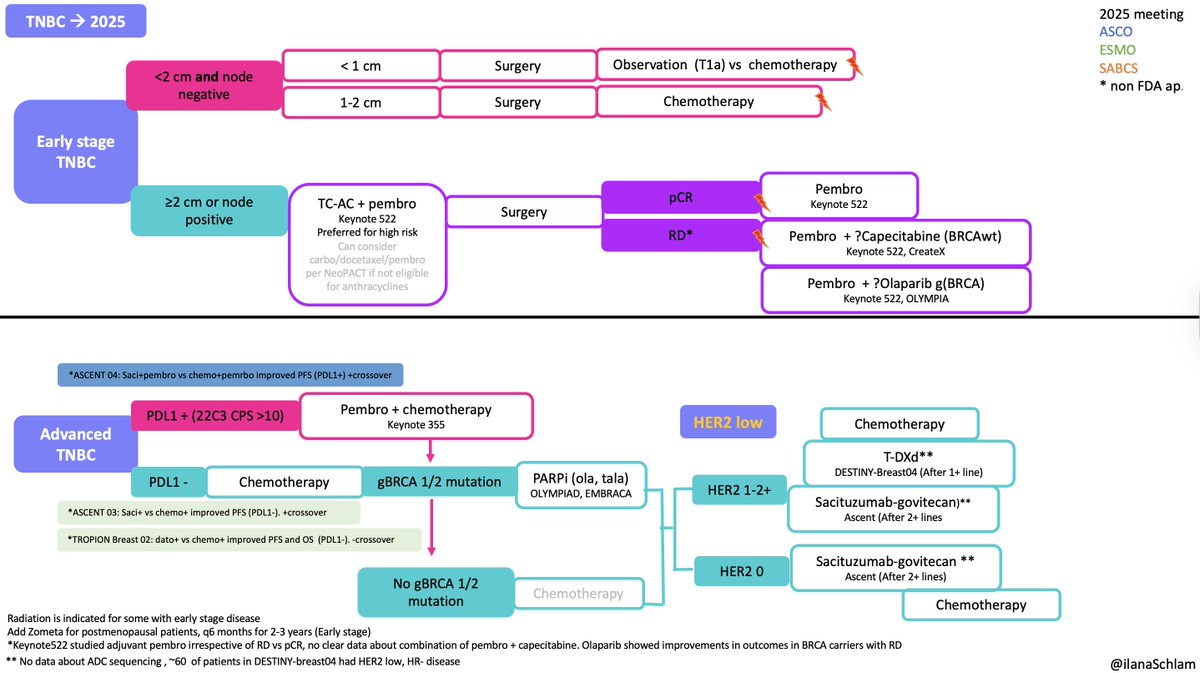
In 2025, many important and long-awaited studies were published. I included them but kept the algorithms unchanged, as there are open questions about how these data will impact practice, particularly in early and metastatic HER2+ disease and mTNBC.
@DFCI_BreastOnc#SABCS25
@hhashmi87@Dr_AmerZeidan@VincentRK How do you define Dara exposed vs Dara Refractory? Is there a certain timeperiod post dara you would think patient will respond to Dara+Tec in 2L as they did in the original trial?
BCMA-Based Therapies in Multiple Myeloma #mmsm
Summary of the approved drugs/combinations targeting BCMA with details on approval date, lines of therapy, supportive studies, common AEs as well as need for REMS
Updated 10/2025
Wow.
All the benefit of checkpoint inhibition in A-BRAVE (high-risk TNBC) was seen in patients with TILs ≥ 30%. No benefit with low TILs.
Unbelievable that we didn’t get to see the TILs data from KN522 yet. Hope we’ll see them soon.
Congrats @vitti10! #ESMO25#ESMOAmbassadors
The bar is raised! Periop 🥪 EVP for cis ineligible (90%) or refusing (10%) MIBC = new SOC *KN905/EV302*
✅pT0 rate highest ever in MIBC 57% ITT, 65% cystectomy sub-pop
✅2yr EFS & OS on par w DDMVAC in cis eligible
-cis eligible EVP🥪 trial *KNB15/EV304* readout awaited #ESMO25
Important data from monarchE and NATALEE adjuvant CDK46 inhibitor @myESMO
With @tess_omeara, here's our take on who needs, and who does not need, adjuvant abema/ribo, co-published in @Annals_Oncology
https://t.co/ofrZzrsTqF
🚨 #ESMO25 | ASCENT-03 (LBA20)
🧬 Sacituzumab Govitecan (SG) vs physician’s-choice chemo in 1L PD-L1-negative or IO-ineligible mTNBC
Results (n = 558; median FU 13.2 mo):
Median PFS: 9.7 mo vs 6.9 mo → HR 0.62 (0.50-0.78), p < 0.0001 ✅
ORR: 48.4 % vs 45.5 %
Median DOR: 12.2 mo vs 7.2 mo
OS: immature
Safety:
G3+ AEs ≈ 66 % vs 62 %
Neutropenia 43 % / 41 %, diarrhea 9 %, anemia 16 %
Tx discontinuation 4 % vs 12 % → better tolerability
📈 Interpretation:
SG delivers a clinically meaningful PFS gain (~3 mo) and more durable responses, with manageable toxicity.
💡 Context:
Comparable PFS to KEYNOTE-355 (IO + chemo ≈ 9.7 mo), showing ADC monotherapy can rival IO + chemo in PD-L1–negative or IO-ineligible mTNBC.
Looking forward to discussion on esmo day 3
#ESMO25 @myESMO@OncoAlert
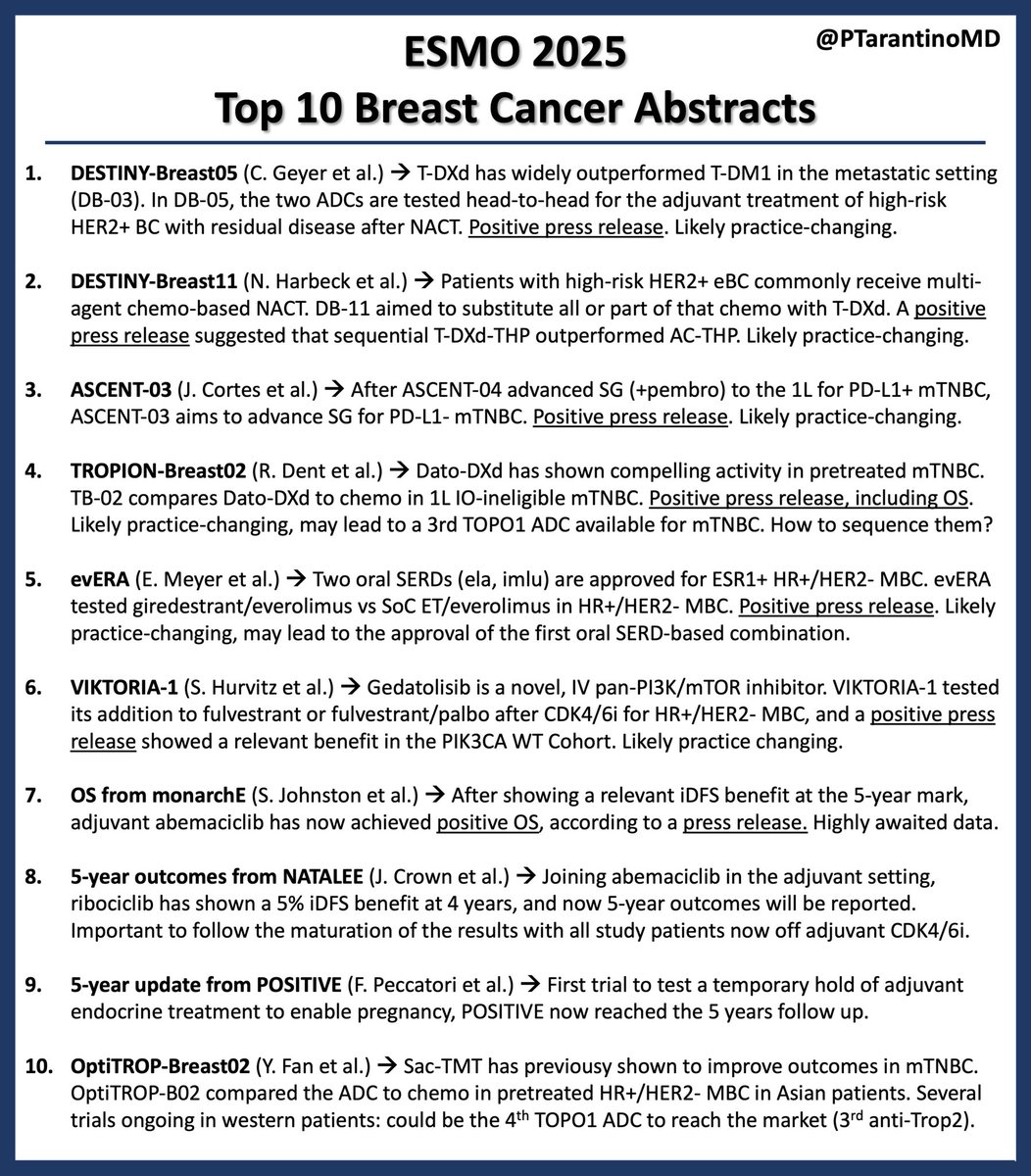
One week to #ESMO25. An unprecedented ESMO conference. Seven positive press releases, anticipating the expansion of T-DXd to the curative setting, two Trop2 ADCs reaching first-line mTNBC, 2 novel ET-based combos, adjuvant CDK4/6i improving OS. See you in Berlin! #ESMOAmbassadors