Last week I finished pain fellowship, concluding a nearly 20 year journey of training & life. What a ride!
So what is next? I'm thrilled to announce that I will be starting my integrated lab and clinical practice @WashUPain focused on the study and treatment of #neuropathic pain.
Thanks for this @JTLonsdale — I’ve been having an exhausting argument with biotech VCs for the last week about not offshoring biotech R&D to cheaper scientific labor in China. Sort of getting nowhere 😛 I don’t know if it’s possible for tech folks to give a warning about the stupidity of Sequoia China, etc, so we don’t have to learn all this the hard way in biotech:
https://t.co/SkpPiWLQK8
A reasonable average time to funding from idea to getting the money is probably 2-3 years. Executing the work is another 2-3 years if you move quickly. In the age of DeSci + AI, these timelines will literally become geologic in scale. People will develop therapies on an idea while grants are still under resubmission status.
Don’t go to medical school.
That’s the caveat I’d add to this very good piece from @tylercowen. He says go into biomed. He’s right. Just don’t do it by becoming a doctor.
I was a residency director for 10 years. I’m a physician building with AI now. Here’s where this goes.
Start med school today and you see your first patient independently in 7 years. That is an eternity of AI progress.
During those 7 years, AI will get VERY good at gathering the history, reviewing the chart and labs, pulling the relevant literature, and handing the doctor a ranked differential with a proposed plan. The doc and patient decide and fine-tune. The AI explains it to the patient and writes the orders.
It’s a more fun job. We do the interesting part and skip the grind.
It is also a job we will need far fewer people to do. If each thinking doctor gets 5-10x more productive, the math is simple. We need maybe 50% fewer of them. That assumes cost craters and demand explodes. If it doesn’t, we’re looking at 90% fewer.
So who do we keep. The best of the established experts, or the new grads?
And did I mention the established experts make the rules?
The hands-on people are safer for longer. Nurses, PTs, surgeons, lab techs. You cannot 10x a pair of hands.
The thinkers don’t get replaced. They get leveraged.
And leverage that strong means the door closes behind the people already inside.
The overemphasis on evidence-based medicine, didactic medicine, statistics, USMLEs, tests, board certifications, algorithms, 1st line/2nd line etc. has made the average physician highly vulnerable to AI. A single highly skilled physician with 20 years of out-of-the-box know-how + AI fluency will do the work of 100-1,000 physicians in 10 years. This is the near term reality. Similar things will happen to wet labs, but this will take more time because it will require actual roboscientist technology to be more advanced- PIs will run labs with almost no humans.
On Friday someone asked me how they should think about what they should do with their career. I told her the most important thing to recognize is that progress proceeds as a series of S curves, and the most important thing is to recognize when an S curve is going to take off and get in at the bottom. The rest -- what exactly you do, for example -- is less important. This is true if you’re a scientist just as much as if you’re an entrepreneur.
With AI today, we don't exactly know where we are on the S curve or when/if it will flatten, but we're certainly not exactly at the bottom anymore. That said, the economy is going to change dramatically in the next 10 years, and there are a bunch of other technologies that are clearly just over the horizon, so there are lots of other S curves that are taking off right now. There are major opportunities in every direction. There has probably never been a better time to be a scientist or entrepreneur.
Love this. I hope this becomes much more common. One bottleneck I hope you can speak to. Data security with PHI. I see that being a barrier to physicians doing things. I’ve wanted to make a patient facing UI to gather clinical data but then don’t know how to do this in a way that my institution/law permits.
Something just changed in medicine that most physicians haven't noticed yet.
As of early 2026, a practicing doctor can prototype a working clinical tool — solo, in a weekend. No CS degree. No team. No budget.
I gave Cardiology Grand Rounds @UCSDHealth on the emerging role of the physician-developer today.
Here's what changed, and why the next decade of medical software gets built by us 🧵
@ethanjweiss It really is incredible how fast it is to make insight from data. I will get new data in clinic, send to claude, have a report when I walk out of the room. Amazing times.
Outstanding work, powerful tool and intriguing findings! Any reason you all honed in on trigeminal, while showing global nerve density reductions? Clinically, symptoms present in the longest axons first (hands and feet) but as one digs more, it seems the pathology can be found more broadly than that.
Using MouseMapper, we generated the first whole-body peripheral nerve maps in obesity and discovered that overall nerve density is reduced in obese mice.
Insightful article. A thought. Isn't 'doing math' like working problems or just working on a question, a form of spacing (you do it at intervals) and retrieval (you're looking to long term memories to do the math)? Maybe the conclusion is that Anki-like flashcards are not as useful for this kind of work.
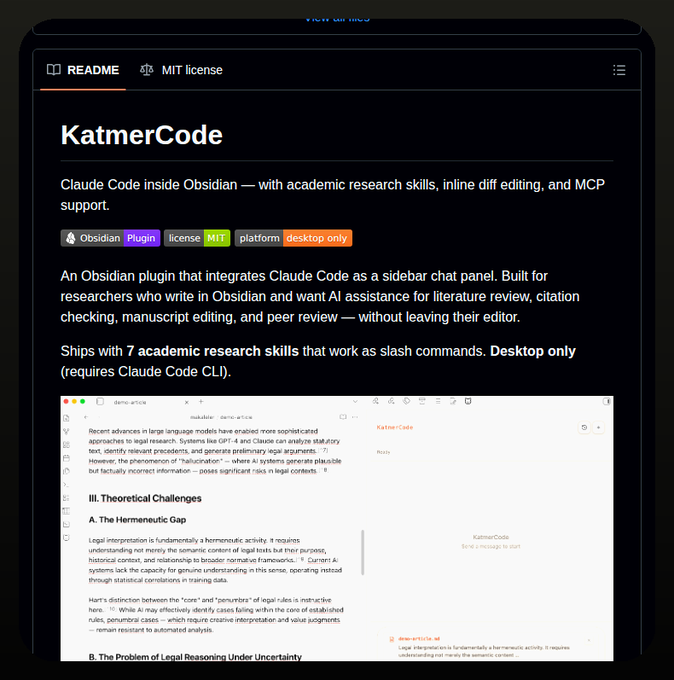
Claude Code + Obsidian for academic research!
Link to the repo in quoted post from Tom below.
BTW, there's so many implementations of Obsidian + Codex/Claude Code, can you recommend one that works well for you?
It‘s time to remove the question mark!
A huge congrats to @CraigMCrews, Ray Deshaies and the scientists @ArvinasInc.
1st FDA approval for a #PROTAC on May 1st 2026. A day to remember. Extra drinks at the Proxidrugs GRC in a few weeks!
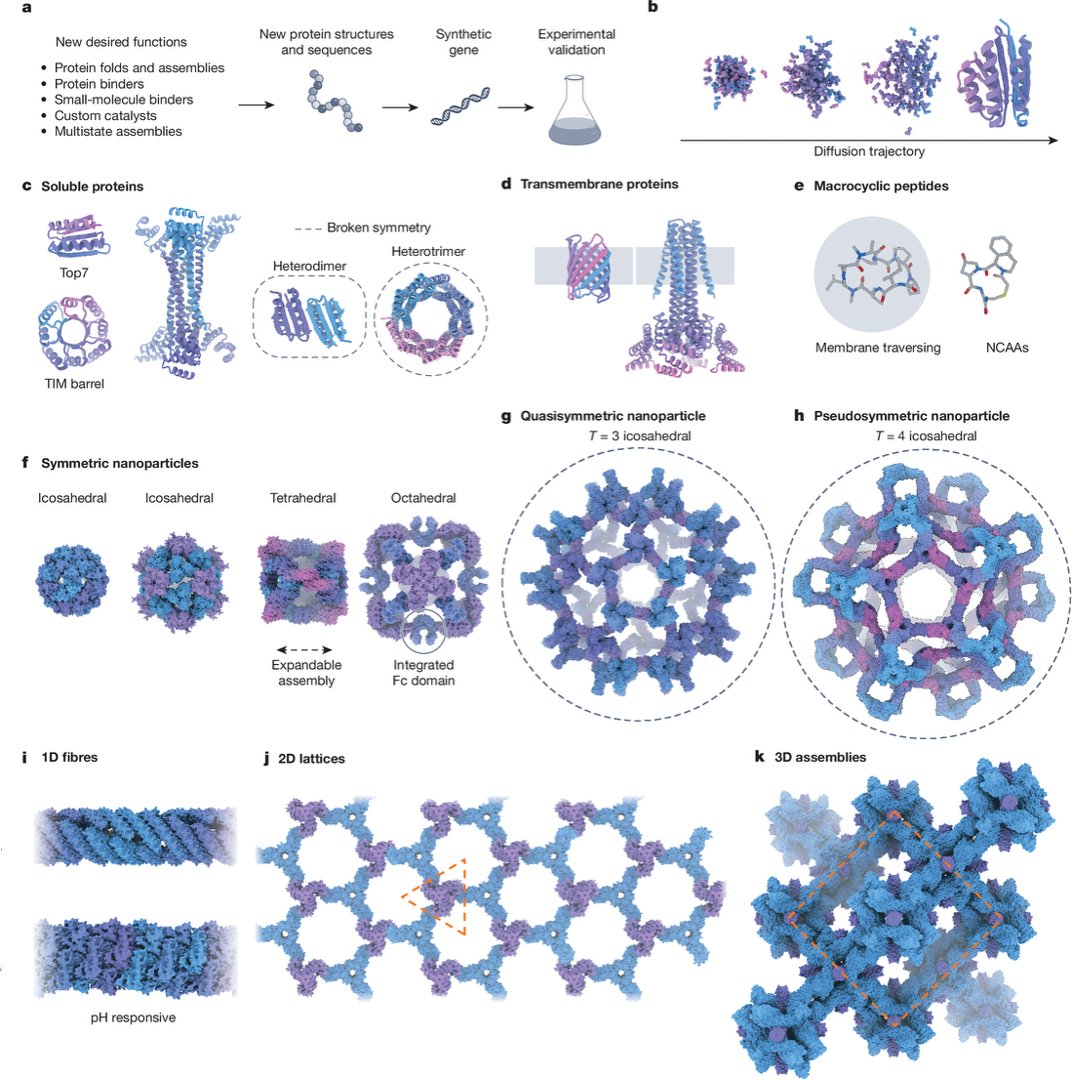
1/ Excited to share our new Review in @Nature:
“The past, present and future of de novo protein design.”
Here, we mainly focused on structure-guided protein design. The field is entering a new phase: now that we can design new proteins, what should we build next?
I'm genuinely enjoying working on what will be my SnapGene replacement software. Chiseling away toward my freedom is uniquely exciting and I can promise the software will be maintained...bc I'm using it daily. Aiming for a May 24th release date of v1.0.0
https://t.co/3mkWtVqa1T
@ImmunoFever@itchdoctor Thanks for sharing. How are you and your lab achieving this? How was the uptake from your team? I have a small, new-ish lab, so I have been able to establish workflow and requirements from the outset.
Notion is our action/task manager and 'Wiki'. Actual experimental and lab metadata live in @airtable, acting as a LIMS. As others said. Notion chokes on any serious number of rows. Airtable and Notion connected selectively via WhaleSync. It works well for us now as a LIMS/PM system.