Rare privilege this week: performed the inaugural case on the new Da Vinci Xi at Sterling Hospitals, Ahmedabad — a robotic ureteric reimplant in a redo patient.
Full circle moment: my father, @DrKandarp_Uro , inaugurated Sterling's first robot years ago.
Ureteric avulsion is one of the most challenging situation that a urologist can face.
Also, when faced with such a situation, a good reconstruction is a must : sharing a link of robotic Ileal replacement on the left side using a single dock .
https://t.co/kaA0TChnsf
The session witnessed active participation and meaningful interaction, making it a valuable and informative experience for all attendees.
@adityaparikh_
The talk will be delivered by Dr. Aditya Parikh, a distinguished Uro-oncologist and Robotic Surgeon at Shyam Speciality Hospital, Ahmedabad. With advanced fellowship training from University College London Hospitals (UCLH) and MPUH,
MUST READ for urologist and radonc!
Real world data on late GU toxicity after radiotherapy for prostate cancer
Short term is underestimation of the real burden for the patient. Important when counselling patients for decision making.
@aleantonellibs1@RicBertolo
What a pleasure Professor Traxer to have had your expertise in demonstrating challenging cases and pushing the boundaries forward for at AIE 2025 @DrKandarp_Uro
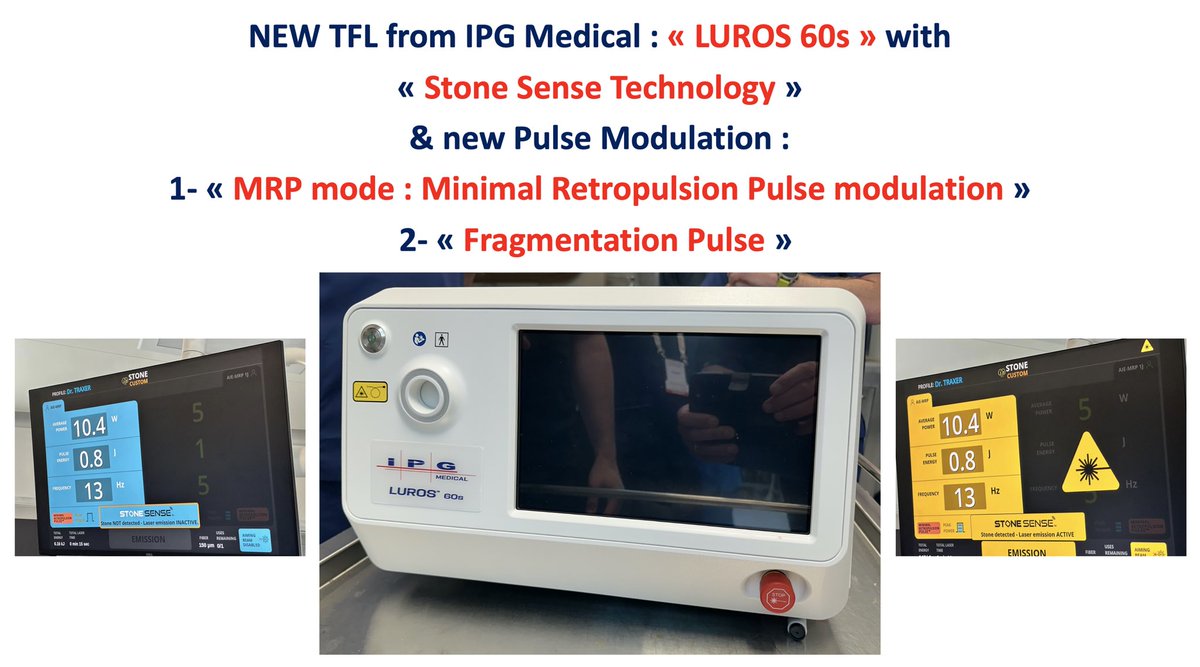
BN179: INDIA, Dec.19th-2025 very privileged to perform the very first Clinical evaluation of the new TFL Laser of IPG Medical : «The TFL LUROS 60s ». With new STONE SENSE- MRP (Minimal Retropulsion pulse) and New Fragmentation Pulse modulation: 20 to 30 J and 1Hz for kidney stone
BN179: INDIA, Dec.19th-2025 very privileged to perform the very first Clinical evaluation of the new TFL Laser of IPG Medical : «The TFL LUROS 60s ». With new STONE SENSE- MRP (Minimal Retropulsion pulse) and New Fragmentation Pulse modulation: 20 to 30 J and 1Hz for kidney stone
“Can surgery still matter in metastatic prostate cancer?” 🩺
💥 RAMPP trial says maybe yes - even in low-volume mHSPC.
🧪 Design:
De novo low-volume mHSPC (≤5 bone mets ± nodes)
👥 Fit for RP + systemic therapy (ADT ± ARPI)
🆚 Radical prostatectomy (RP) + BST vs BST alone
🎯 Primary: Cancer-specific mortality (CSM)
📊 Results (~5 yrs):
•🩸 CSM: 13% vs 23% → HR 0.39, p=0.045 ✅
•🧭 Progression: 59% vs 60% (NS)
•💀 OS: 81% vs 74% (p=0.13)
•⚙️ Complications ≥ G3: 14%, no peri-op deaths
💬 Takeaway:
RP added to BST reduced CSM in low-volume mHSPC — mirroring the STAMPEDE RT signal 🔁
But OS gain unproven → discuss in MDT before adopting.
📖 Graefen et al. European Urology 2025.
🔗DOI: https://t.co/XMhMFVLHPW
#OncoTwitter #ProstateCancer #mHSPC #UroOnc
@OncoAlert@myESMO@ESMO_Open@ASCO@EuropeanUrology@EUplatinum@Uroweb