We are group of passionate Advanced Musculoskeletal Physiotherapists who also have a website full of resources for physios working in advanced practice roles.
Growth and remodelling of living tissues: perspectives, challenges and opportunities https://t.co/ruq4ut3irF
In many cases, growth and remodelling processes depend strongly on mechanical factors and the associated mechanobiological response at the cellular level.
Nice infographic from a new paper ( Is 9 months the sweet spot for male athletes to return to sport after ACLR)
No association between time to RTS and new injury
👏👏
@enda_king@RoulaKotsifaki
Thrilled to share our new paper in @NatureHumBehav!
https://t.co/pcNX1FCvZJ
We show that combining biological 🧬 and psychosocial 📋 data offers a much stronger, more reliable path to predicting pain and diagnosis. 🧵
Our latest study explores ACL surgical vs. nonsurgical treatment decisions from the perspective of physios:
👉 a mismatch between physio beliefs & the info provided to patients
👉 7 barriers that physios face to offering & providing nonsurgical treatment
https://t.co/ORdYDC5NNx
Great new research from Tjerk Visser & colleagues has given us normative values for calf testing that go beyond reps alone!
Assessing peak height, total work & total displacement can provide valuable insight into calf function.
Visser et al. (2025) 🔗 https://t.co/uVY5VfdpDW
Rehabilitation After ACL Reconstruction ... The Aspetar Way
In Aspetar, our Mission is to assist all athletes achieve their maximum performance and full potential. We aim to give each athlete the individualised support they need based on their injury, their goals and their lifestyle to optimise outcomes as efficiently as possible.
The Aspetar Way is our approach to ensure these aims are achieved with consistency and repeatability to the highest level throughout our team for every athlete:
Individualised Approach.
▶️ Assessment Guided Rehabilitation.
▶️ Multidisciplinary Team (MDT) Contribution.
▶️ Address multiple physical qualities concurrently.
▶️ Focus on motor learning and development rather than training.
Individualised Approach
Although ACL injury is unfortunately frequent in many sports involving landing, pivoting and contact, the journey after injury is a very unique experience for every athlete. While injury to the ACL is a consistent theme with all, there are a variety of ways each athlete may deviate from the time of injury:
▶️ Level of trauma to other structures in the knee
▶️ Disuse and deconditioning post injury and post surgery
▶️ Graft type used (patellar, hamstring, quadriceps)
▶️ Post operative precautions
▶️ Athlete motivation and goals
▶️ Demands of sports they are returning to
▶️ Previous training history
▶️ Response to training stimulus
▶️ Social Support (Work/Family/Financial Commitments and Constraints).
Our approach is also individualised to that athlete’s injury history to ensure we use the time afforded by ACL rehabilitation to target all deficits relating to previous injury not only those related to the current knee injury. Our approach is to modify our exercise selection, programming, periodisation and support to fit these individual differences while helping all to achieve their common goal as effectively and efficiently as possible.
Assessment Guided Rehabilitation
Before starting on any journey it is essential to have clarity about what the end of the process should look like and the steps required to get there. While many rehabilitation processes know where to begin the journey, and commence with clear direction, they often lose their way or fail to complete the journey, ultimately compromising the athlete’s outcomes.
The end of the rehabilitation journey for most athletes, the clinicians, and various stakeholders that are supporting them is:
▶️ To return to their pre-injury sport
▶️ To do so with the absence of symptoms (pain or instability) in the knee
▶️ To minimise the risk of subsequent injury to either knee
▶️ To return to their preinjury levels of performance (or higher)
Focus on Quality vs Quantity – its not what you do but the way that you do it!
There is regular feedback on the quality of execution of each exercise in the program as much as the number of sets and repetitions. This helps the athlete avoid:
1⃣ - Rushing through the exercises to complete the prescribed dosage but without the quality to achieve the technical changes and motor patterns
2⃣- Not recognising the exercise is no longer technically challenging (i.e. landing exercise) or is not intense enough (leg press for a 10RM but athlete could do 4-5 more repetitions at the prescribed weight) this not achieving the desired adaptation
3⃣- Not listening to their body during the exercise execution for example either aggravating their anterior knee during a quadriceps strengthening exercise or feeling the load/strain in their lumbar spine instead of their hamstrings during a deadlift or bridge exercise for example..
SUMMARY
During ACL rehabilitation, our processes should match the goals of each individual athlete, provide clarity on the key physical outcomes we want to achieve, and track their progress throughout. Physiotherapists are required to utilise their entire rehabilitation skillset to develop all the relevant qualities concurrently giving us the best chance of supporting each athlete to achieve their maximum performance and full potential after injury while being supporting each member of the MDT in completing their roles and responsibilities.
Furthermore, systems can be reviewed and refined on an annual basis to further enhance our standard of care as our clinical practice, technology and research evolve over time.
✍️– Written by @enda_king
🔗Read Full Paper 👉 https://t.co/oZ6iXg1h5w
🛑Almost 1/5 of the axial load of the wrist, transferred by Triangular fibrocartilage complex (TFCC), located between the ulnarhead, lunate & triquetrum on ulnar side of the wrist.
It's the most important stabilizer of distal radioulnar joint,as well as of ulnar side of carpus
🛑Radiographic Dx of shoulder dislocations mentioned.Most shoulder displacements occur in an anterior– inferior direction.
Posterior dislocations are uncommon & Inferior dislocations (luxatio erecta) are rare. Some authors mentioned another type (superior) dislocation as rarest
🛑Injuries to Tarsometatarsal (TMT) joint complex (Lisfranc joint) are not common, but frequently missed.
Midfoot
pain on palpation, specifcally at TMT joints, plantar ecchymosis & edema are all highly suggestive of a Lisfranc injury and an instability test should be performed
🦶🏼
Medial ankle impingement
PM ankle impingement
T/N joint
Deltoid ligament (5% of all ankle sprains)
Navicular stress # (N-spot)
Tib post tendinopathy
STJ
Spring ligament
Os naviculare (at least 20% of us have this)
FHL tendinopathy (often mis-diagnosed as plantar fasciitis)
Should you get an MRI to predict #osteoarthritis? 🤔 This week on @jointactionorg, we talk with Drs. Alison Chang & Ali Guermazi about the pros, cons, and common misconceptions around MRI scans in OA diagnosis. Hint: more isn't always better! https://t.co/Q7JgG0ezQF
📢📢New paper:
An international consensus on the etiology, risk factors, diagnosis and Management for individuals with Frozen Shoulder: a Delphi study
https://t.co/HNNITTZ5d7
Vertebral arteries(VAs) are chiefly responsible for blood supply for posterior circulation contributing to nearly 1/3 of the overall cerebral blood flow. V1–V3 are extracranial,while V4 is intradural.
Asymmetry in the VAs is present mostly left dominance
https://t.co/bm6gGeWs4q
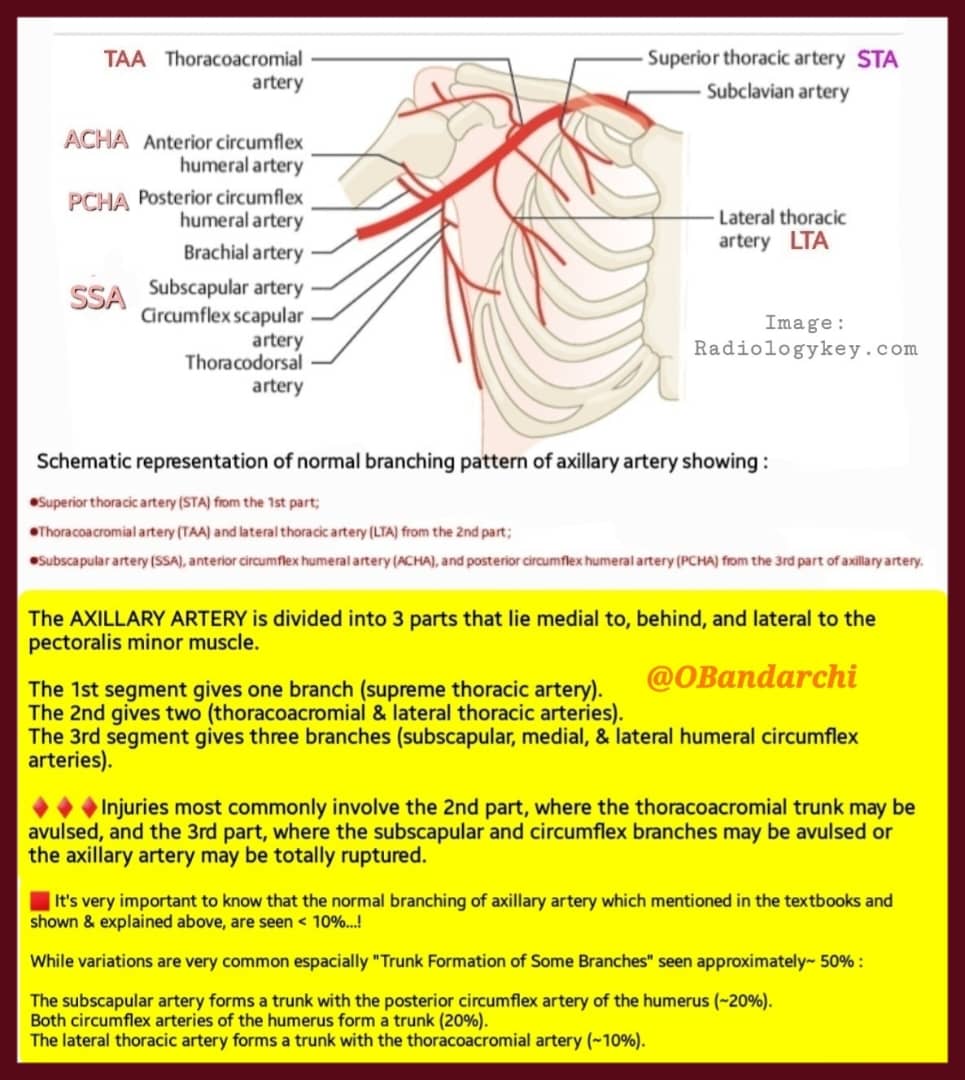
🛑Normal branching pattern of axillary artery shown.
It's worth knowing that normal branching of axillary artery which mentioned in the textbooks & shown here are seen in only< 10%.
On the other hand, variations are common esp. "Trunk Formation of Some Branches" which seen~ 50%
💥 #Review
❓ "Is neurogenic inflammation involved in tendinopathy❓"
"There is strong evidence for the upregulation of nerve
ingrowth markers, the #glutaminergic and #sympathetic nervous systems in tendinopathic tissue."
Read more 👉 https://t.co/5O5CZkscJH
#WeAreBOSEM