NOW AVAILABLE: The NLA's Updated Clinical Guidance on Familial Hypercholesterolemia (FH)
This updated expert clinical consensus on FH reflects more than a decade of advances in screening, diagnosis, and treatment.
📄Read the full consensus statement: https://t.co/9YNEJ8UvRj
🎥Watch our CME-accredited video podcast with key authors: https://t.co/WBZd6SFNoy
📰View the press release: https://t.co/fFEMVN8S7X
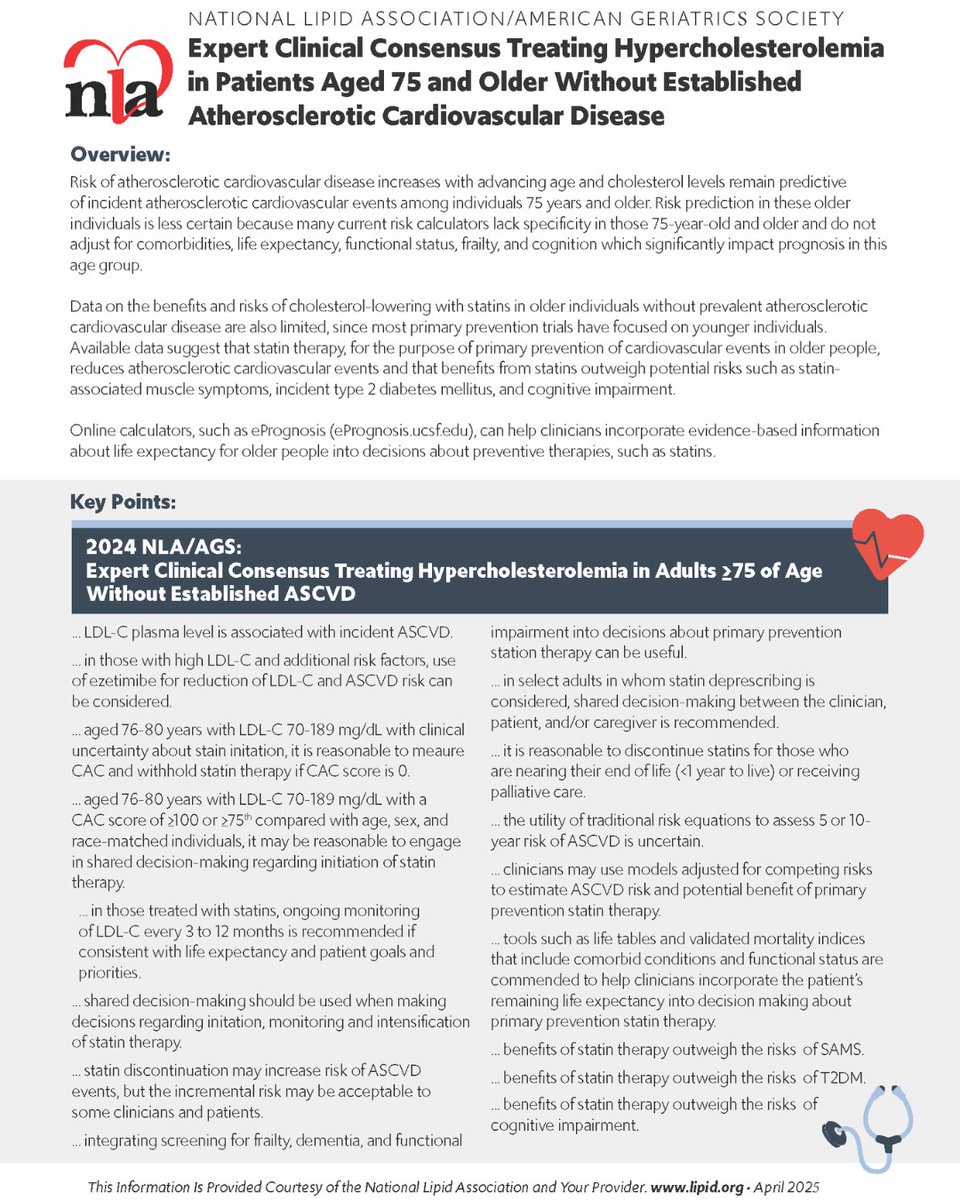
📢NEW NLA & @AmerGeriatrics expert clinical consensus on managing #hypercholesterolemia in adults older than 75 years without a history of #ASCVD.
Read the article now: https://t.co/cOANMlQbdU
A common misconception is the thought that low LDL-C might increase risk of hemorrhagic stroke or dementia. This great review provides a summary as to why these claims are unfounded.
https://t.co/weHlul1xQZ.
MUST READ - New Term SMurfs - (1) IT IS CRIMINAL FOR CLINICIANS NOT TO TEST LP(a) IN ALL. We really need to take Lp(a) increases very seriously. - Way outside of the box, but I am at the point to advise Lp(a) patients to take a PCSK9i to blow away apoB and at least lower Lp(a) somewhat (25-30%). Fingers crossed that obicetrapib becomes a player in attacking Lp(a). @nationallipid@society_eas
How about this study (in press) - EZETIMIBE as a player to prevent Alzheimer's Disease and Related Dementia (ARRD). See Aging Biology | Ezetimibe lowers risk of Alzheimer’s and Related Dementias over 7-fold, reducing aggregation in model systems by inhibiting 14-3-3G::hexokinase interaction (https://t.co/G6fX85Hoq7) @nationallipid@society_eas@lipiddoc @TheFHFoundation
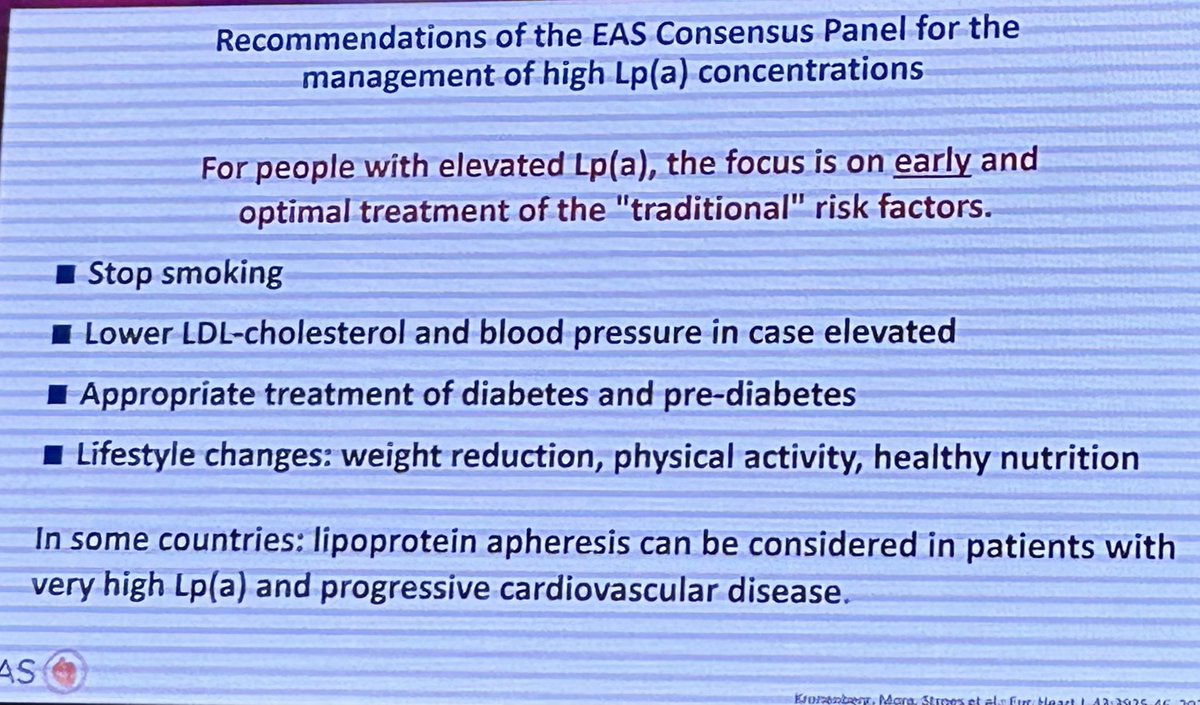
👉High Lp(a): Actionable strategies for risk assessment and mitigation
☝️This review focuses on the identification and clinical management of patients with high Lp(a).
Specifically, the authors highlight the clinical value of measuring Lp(a) and its use in determining Lp(a) associated CVD risk by providing actionable guidance, based on scientific knowledge, that can be utilized now to mitigate risk caused by high Lp(a)
🔓Open Access
https://t.co/kkxnMJT6gQ
@society_eas@LpaForum
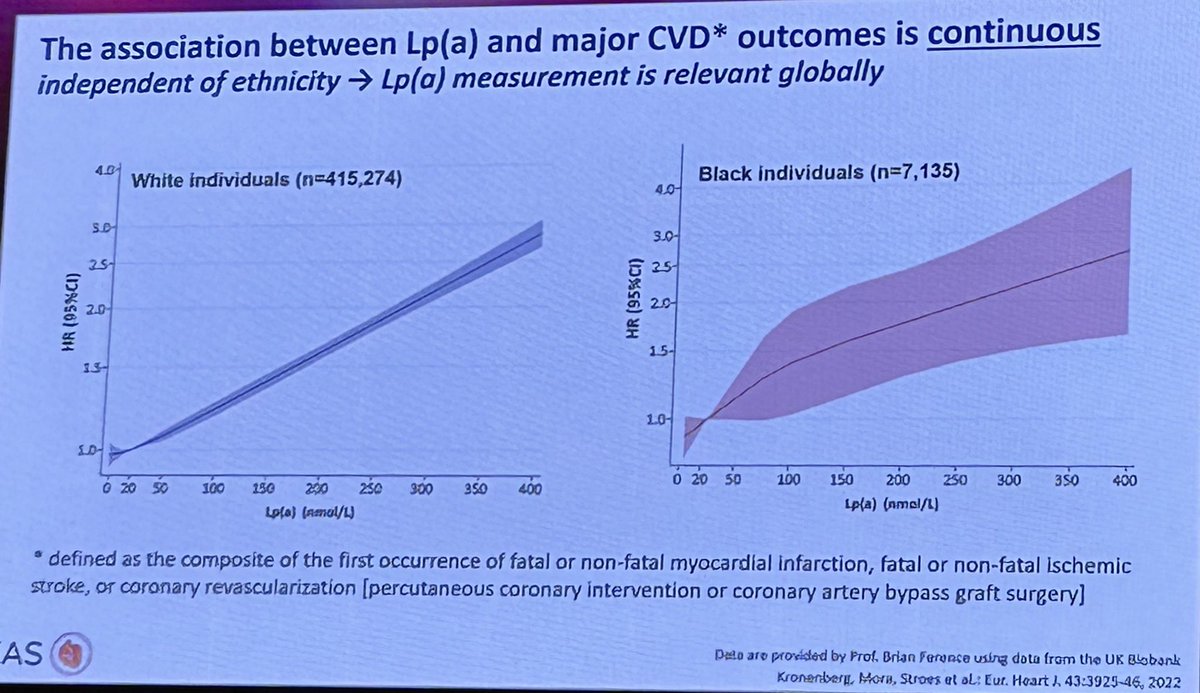
Lp(a) | Prof Florian Kronenberg
❤️ Lp(a) is an independent risk factor for CVD & should be measured at least once in a 👥 lifetime
If Lp(a) is ⬆️ we should 👇🏼
🔹Test the family, much like what we do in FH
🔹⬇️ modifiable CVD risk factors (ie LDL) as early as possible
#MedTwitter #cardiotwitter #MedEd @natraff8@society_eas@escardio@ACCinTouch@RACGP
Thank you, Dr. @ErinMichos. Our📜reveals increased risks in🤰with RA, including preeclampsia, PPCM, arrhythmias, AKI, and VTE during delivery admissions. A collaborative approach involving rheumatologists, cardiologists, and high-risk ob is needed @OHSUCardFellows#CardioTwitter
An excellent review of the power of zero and the low prevalence of non-calcified plaque when CAC = 0.
https://t.co/cxl7W9fjfV by my former fellows - Irfan Zeb and Yasmin Hamirani
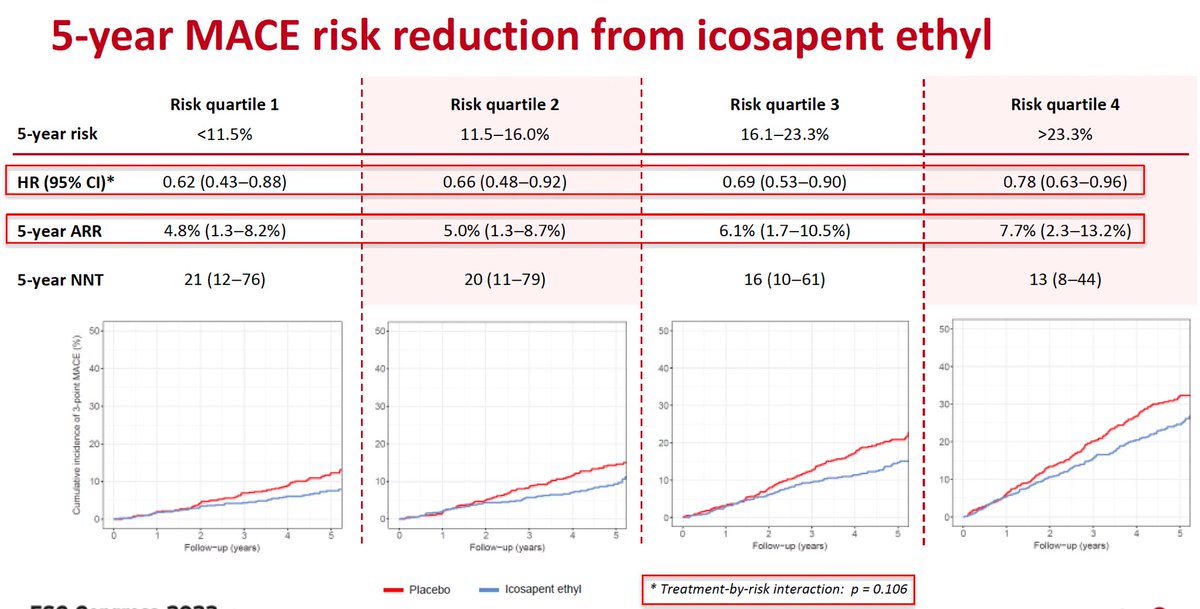
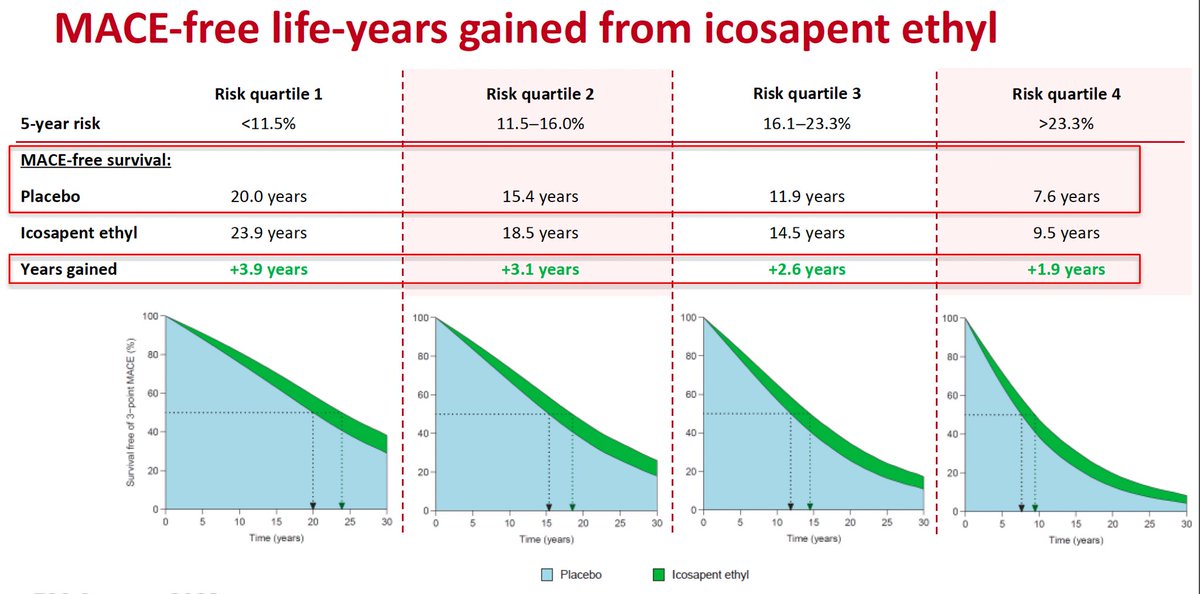
⚠️Effects of icosapent ethyl on residual CV risk according to predicted baseline risk: #REDUCE-IT
👉Among patients with ASCVD and ↗️TG levels, icosapent ethyl significantly ⤵️ MACE across all quartiles of baseline CVD risk
👉5-year ARRs are largest for 👥 with the highest residual risk
👉Lifetime benefit (gain in MACE-free life expectancy) is largest for younger 👥 with a relatively low to moderate residual 5-year risk #ESCCongress @riesgo_SEC
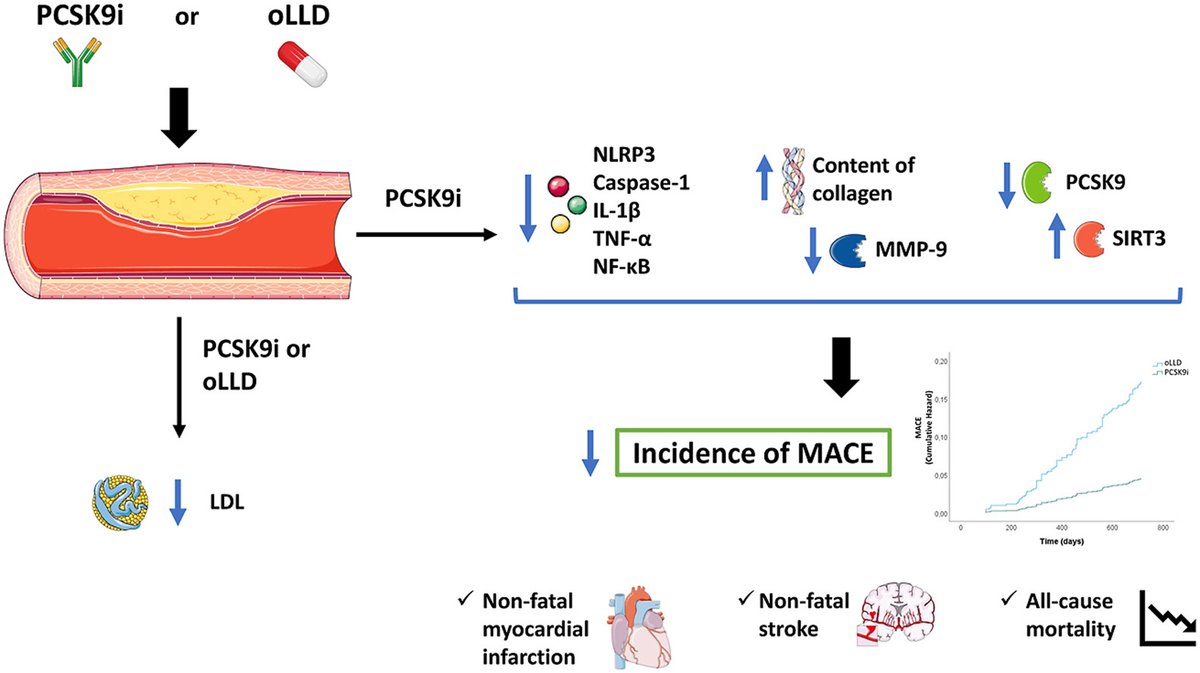
• #PCSK9i monotherapy is associated w/ a ⬇️ incidence of a composite of MI, stroke & 💀
• The expression of inflamm proteins within the plaque is associated w/ the incidence of #MI, stroke, & 💀
🔗 https://t.co/WbZSclmV4o
@CelestinoSardu@P_Paolisso@arturocesaro@society_eas
Muvalaplin, a selective small molecule inhibitor of Lp(a) formation, was not associated with tolerability concerns and lowered Lp(a) levels up to 65% following daily administration for 14 days. https://t.co/YepZB4HQ8w #ESCCongress