Finally published on Cell Death&Disease (@Nature group)! A comprehensive review I had the pleasure and the honor to write with prof. Paolo Calabresi (Università Cattolica del Sacro Cuore) and prof. @lvolpic (UAB).
Have a read!
https://t.co/Hdw2rEhAm1
🧠📚 #Neurology#Parkinson
A new Research Topic in @FrontMedicine is out:
"Predicting Clinical Trajectories in Prodromal & Early PD and Atypical Parkinsonism"
Submit your contributions!
Abstract🗓️April 13, 2026
Manuscript🗓️August 1, 2026
#Parkinsonsdisease#Neurology#Biomarkers@FrontiersIn
#MondayTip#Tandem occlusions
🛑Simultaneous blockage of the extracranial ICA and an intracranial artery, commonly MCA
⚠️Atherosclerotic disease or artery-to-artery embolism
📉More severe strokes & worse clinical outcomes vs isolated LVO
☝️EVT is the mainstay👉careful strategy
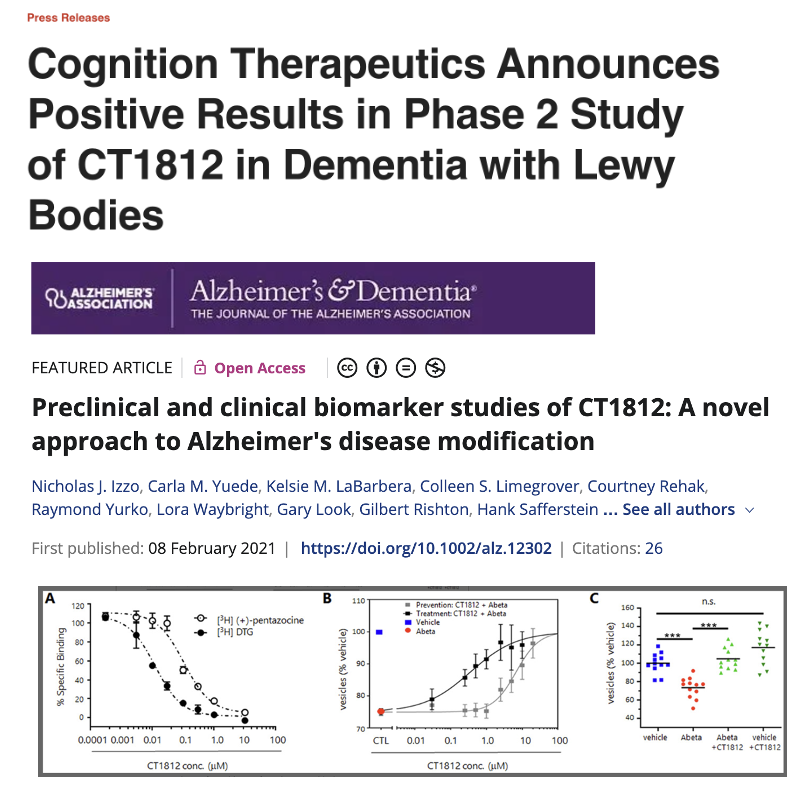
A new drug has shown promise for Dementia with Lewy Bodies in the just released data from the SHIMMER (CT1812) trial. The data just released revealed that participants taking CT1812 performed better across measures of behavior, function, cognition, and movement. The treatment was well-tolerated. The next step is a BIG trial. The compound has been of great interest in Alzheimer's.
https://t.co/eNthyNgOCV #dementiawithlewybodies #Alzheimers
Happy to share our last comprehensive review about the state of the art of biomarkers in Parkinson's disease and future prospectives regarding new promising biomarkers in the frame of the recent "cultural revolution" in the conceptualization of PD.🧠🩸
https://t.co/EzVca8ioVU
Doing neurology residency interviews today.
My favorite question to ask is “If you were a cranial nerve, which one would you be and why?”
Let’s see how Chat and Claude answer 😂
🚨Just Published in Neurology @GreenJournal !
Still a chance for EVT in BA occlusion🧠and NIHSS<10
Thrombectomy leads to better outcomes vs IVT alone💉
Thanks to IRETAS and SITS collaborators
Here is a thread 👇 @carlowcereda@a_ciacciarelli@ZiniAndrea
https://t.co/fbdsalhsNA
We're excited to share that the Parkinson’s Foundation has published a new article in the December issue of The Joint Commission Journal on Quality and Patient Safety titled “Protecting Parkinson’s Patients: Hospital Care Standards to Avoid Preventable Harm.”
More than 300,000 people with Parkinson's disease are hospitalized each year. While hospitalized, people with PD face increased risk of preventable harm, including longer hospital stays & deterioration of PD symptoms. There is a critical need to heighten awareness of this problem and advance overall patient safety.
Read more: https://t.co/ar5navAhHw
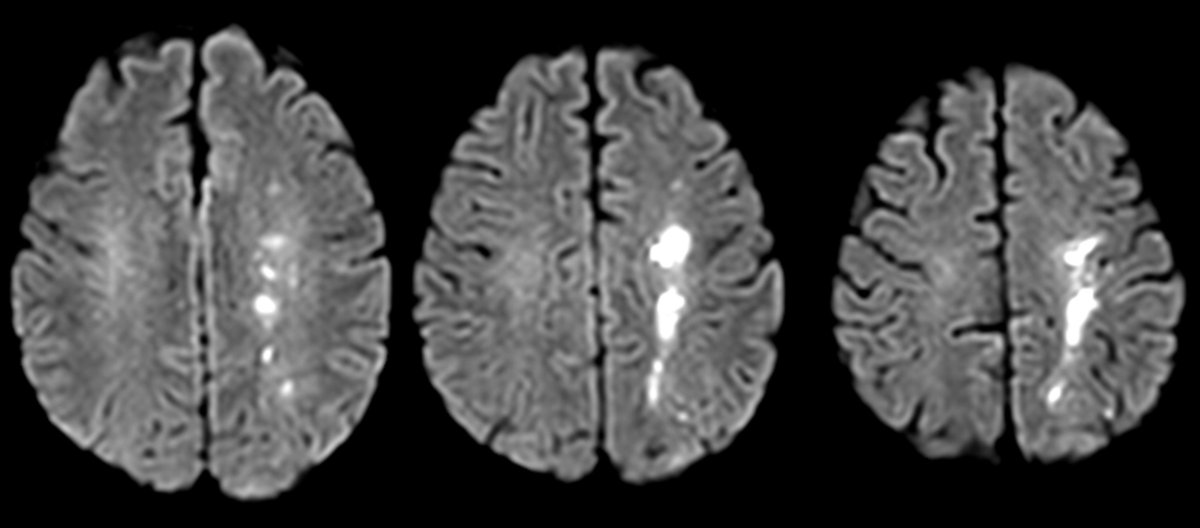
Anyone can see the bright spot on diffusion—what sets you apart is if you can tell them why it’s there!
Can you tell a stroke’s etiology from its appearance on MRI?
Main stroke types:
Artery to artery embolism
—Vulnerable plaque ruptures & causes clot formation
—Occludes the artery & distal blood flow
—Makes a wedge shape
Distal hypoperfusion:
—At the border zones
—Remember borderzones almost look like a fancy letter H for Hypoperfusion = two vertical lines (ant, internal watershed) that have curls at each end (ant & post external watersheds)
Vasculitis
—Inflammation ofvessel wall
—Idiopathic, autoimmune, or infectious
—Remember: Vascu-LIGHT-us = tons of little regions LIGHT up on DWI
—Remember Vascu-LITE-us = usually in LITE vessels or small vessel territories
Impingement on perforators:
—Large vessel plaque covers opening of small perforator in its wall
—Perforators affect the Ps = pons, putamen (lenticulostriate)
Small vessel dz
—Many different pathologies that cause occlusion of small, unnamed vessels
—Remember: Small & subcortical both start w/—tend to be subcortical
Cardioembolic
—Emboli from heart stasis or vegetations
—Remember: Emboli & everywhere both start w/E = emboli go everywhere
So now you know how different etiologies have different distributions on MRI.
Remember, catching a stroke on DWI isn’t the end of your job—it’s the beginning!
Just published our systematic review about the use of botulinum toxin in FOG in Parkinson's disease with a spotlight on its multimodal mechanisms of action in the sensorymotor system. 🧠 💉
Have a read here! @Toxins_MDPI#Parkinsonsdisease#Neurology
https://t.co/56B5Naj4F0
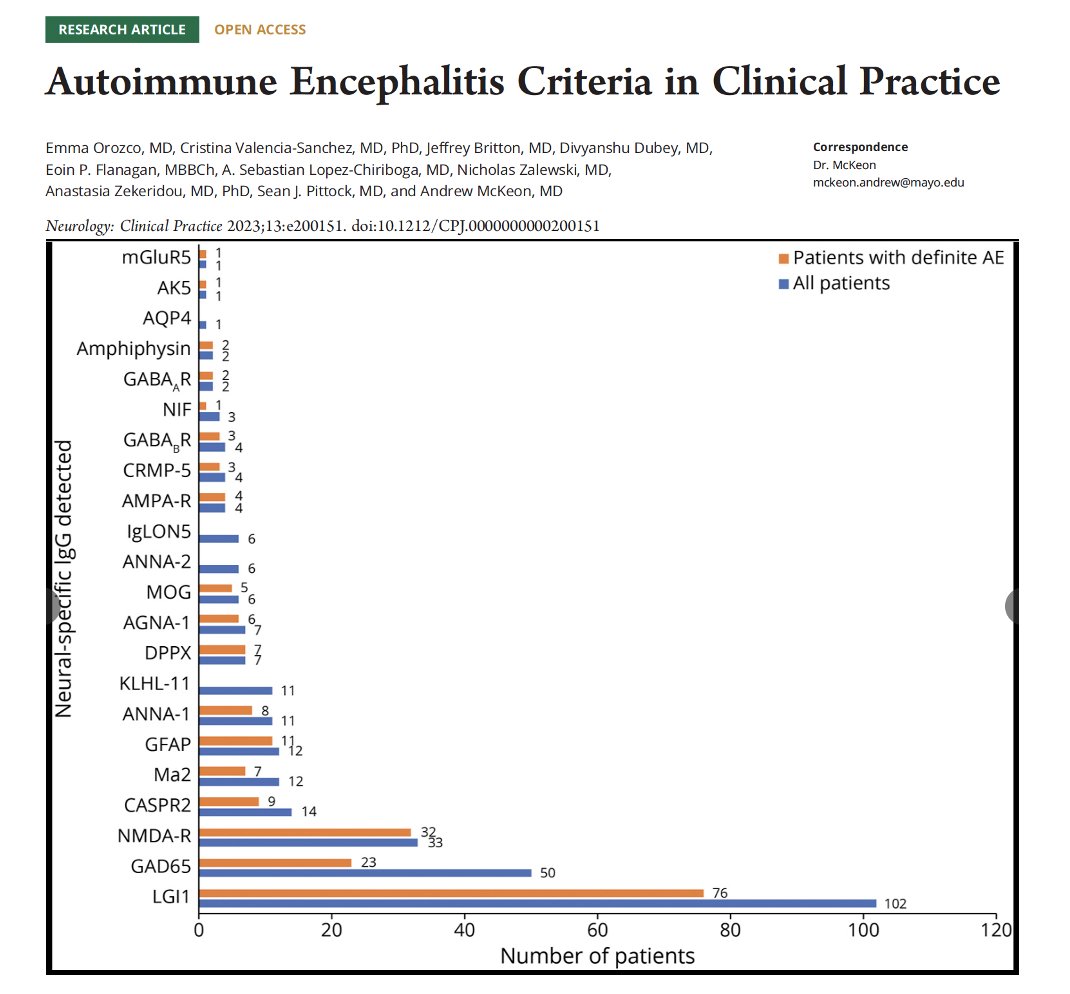
Think first about LG1, GAD65 and NMDA antibodies first; at least by percentages. Are you drowning with thinking about possible autoimmune antibody syndromes in practice. Love this chart by Orozco and colleagues @GreenJournal Clinical Practice.
Key Points:
- The authors assessed 'clinical practice applicability of autoimmune encephalitis criteria.'
- 538 folks included in the analysis from Mayo Clinic.
- Subacute onset of memory deficits, altered mental status and/or psychiatric symptoms are important symptoms.
- The 3 most common and definite AE-IgGs detected were 'LGI1 (76, 34%), NMDA-R (32, 16%), and high-titer GAD65 (23, 12%).'
My take: I love this paper as guidelines do not always help you in the real-world. I think it will be important to focus clinicians on some of the common autoimmune antibody related encephalitis syndromes (first). We should also teach that the GAD65 is the one that may be commonly present, but not always responsible for the encephalitis syndrome.
https://t.co/APfk8puqCk #autoimmune #paraneoplastic #parkinson
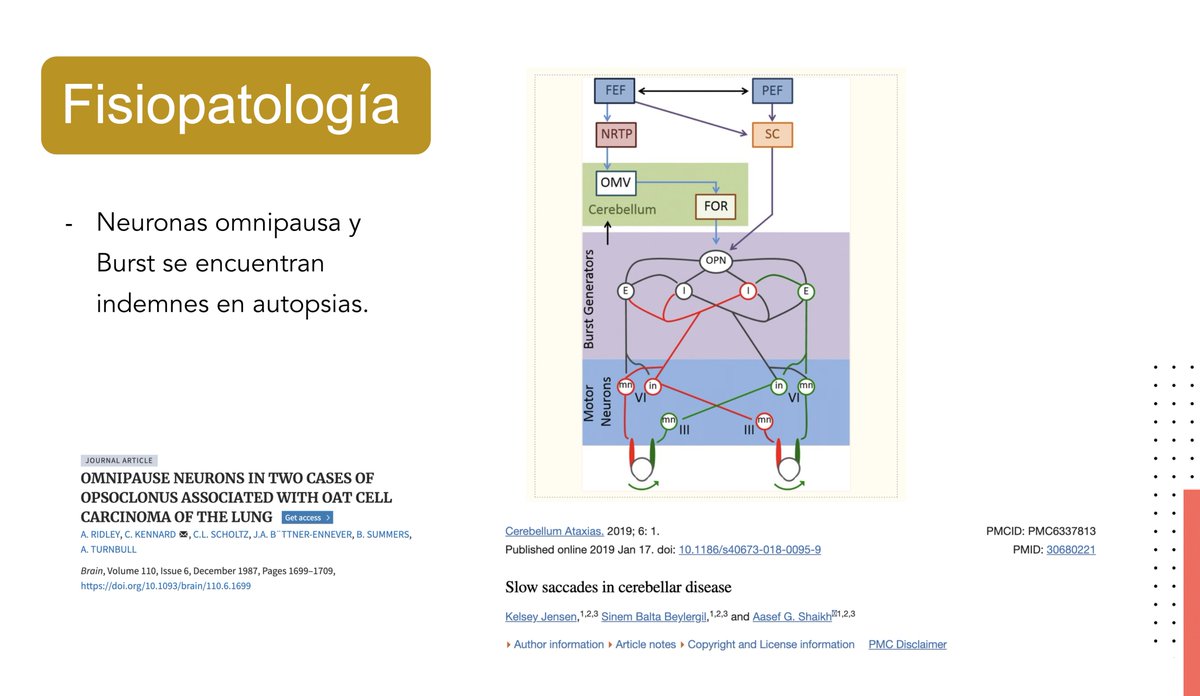
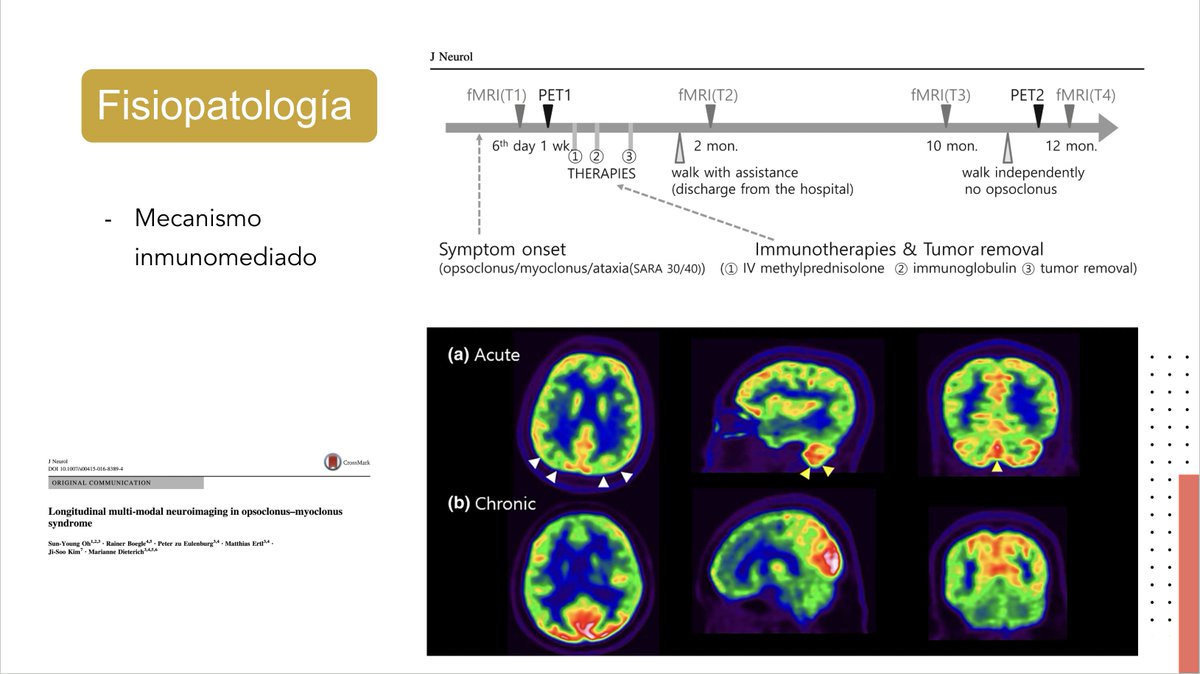
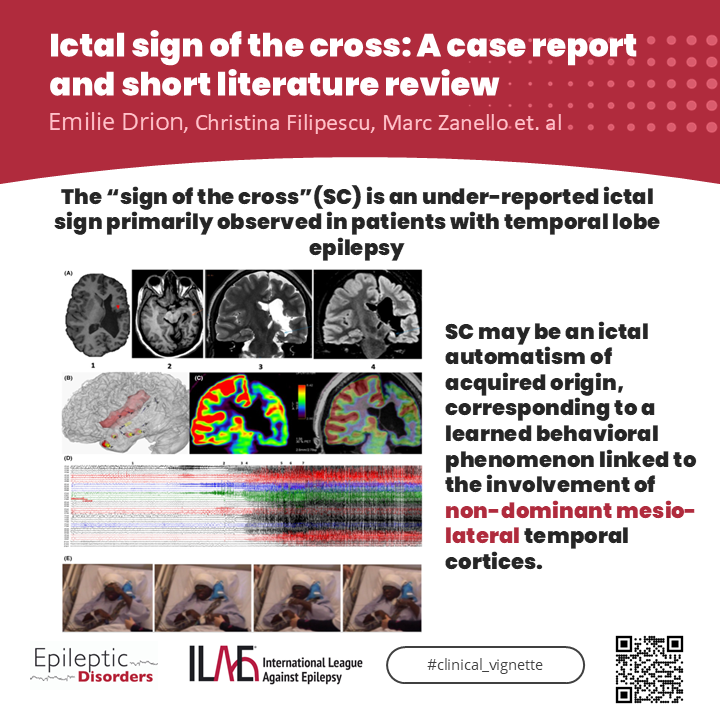
Opsoclonus myoclonus syndrome is a rare paraneoplastic syndrome . Neural generator is not known but evidences suggest the role of fastigial nucleus disinhibition from the loss of function of inhibitory (GABAergic) Purkinje cells in the cerebellum.
https://t.co/vjQtRHSJBn