🧠🦎 A new article published in Practical Neurology’s new journal club format!
GLP-1 receptor agonists—originally inspired by Gila monster venom 🦎—could become disease-modifying therapies for IIH.
🔗 https://t.co/ye65hGL5FM
#Neurology#IIH#GLP1#MedTwitter
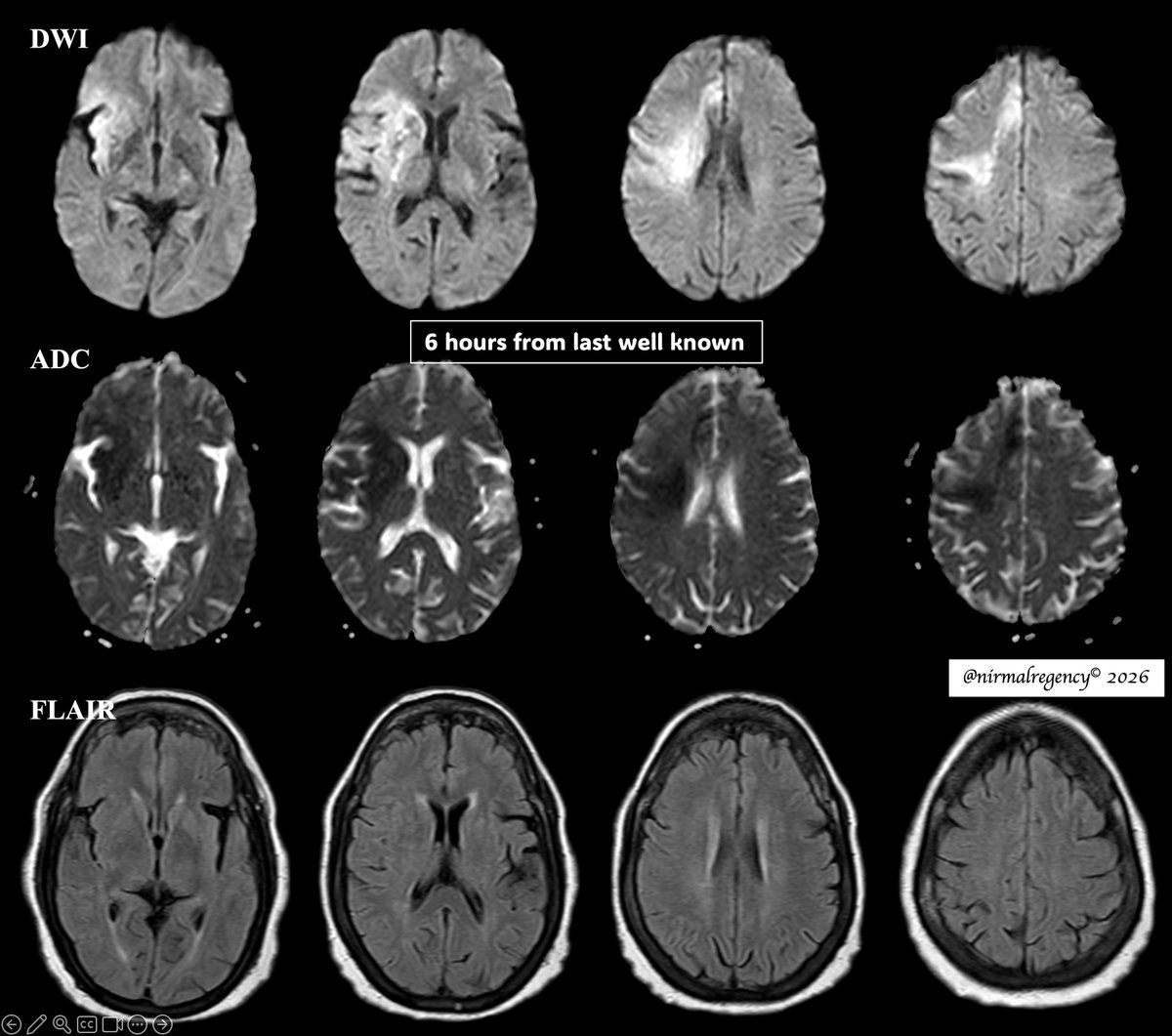
Radiologists in the ED increasingly face imaging findings linked to recreational substances, that leaves a broad neuroimaging footprint in the emergency department.
Know the patterns, save time, save lives.
https://t.co/PmFNe2PT0b
#RGphx@RadioGraphics@teachplaygrub
Continuous EEG within 7 days after stoke identifies additional epileptiform abnormalities with prognostic value for post-stroke epilepsy beyond routine (short-duration) EEG.
https://t.co/mYX3hIxvDn
#EEG#epilepsy
The efficacy and safety of ketogenic diet therapy among adolescents and adults with drug resistant epilepsy: A systematic review and meta-analysis https://t.co/srCLvOmbTc #Neurology#Epilepsy
Maybe the best description of the general neurologist
1. Knows the 3 C's of neurology:
• The Common
• The Critical
• The Curious
2. Comfortable in the ward and ICU
3. Skilled in diagnosis (localization, imaging, EDX, LP) and treatment (thrombolysis, ASMs, immunotherapy etc)
Seminars in epileptology: Holistic management of epilepsy in adults with intellectual development disorders https://t.co/DeIEeEGGdt #Neurology#Epilepsy
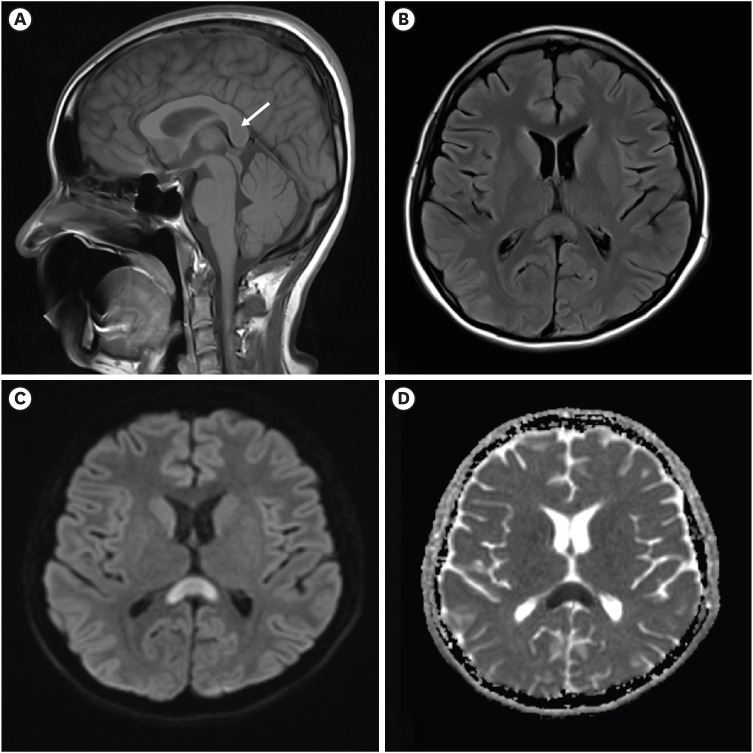
Good short review on the never ending issue of NPH … I the end, it seems it’s essentially a disease with no long-term effective treatment, so maybe its diagnosis (and the neuroradiological effort to do it) become less important ?
A new antiseizure medication that many clinicians are reading about now is cenobamate.
As this molecule gradually enters more epilepsy practices, it is probably worth looking at it quietly through the trial data first rather than through excitement alone.
The most interesting part of cenobamate is not that it is new.
It is that some of the adjunctive therapy trials showed seizure freedom numbers that are higher than what many clinicians are used to seeing in refractory focal epilepsy studies.
📌 Chung et al. Neurology 2020
Adjunctive cenobamate 200 mg/day showed:
• Median seizure reduction:
55.6% vs 21.5% placebo
• ≥50% responder rate:
50.4% vs 22.2%
• Seizure freedom during maintenance:
28.3% vs 8.8%
📌 Krauss et al. Lancet Neurology 2020
Dose-response trial:
100 mg
200 mg
400 mg
Responder rates increased progressively:
40%
56%
64%
Maintenance-phase seizure freedom:
4%
11%
21%
Placebo:
1%
The long-term extension studies also suggested that at least some patients maintained benefit over years, not just during an early response window.
But there is another side to the molecule which is equally important.
Cenobamate is not a drug that rewards aggressive escalation.
The practical learning from most experienced users seems to be:
Slow titration matters enormously.
Because alongside efficacy, clinicians also need to think about:
• DRESS risk
• Somnolence
• Dizziness
• Ataxia
• Cognitive adverse effects
• Drug interactions
• QT shortening
• Liver monitoring
One very important OPD pearl:
A significant part of cenobamate intolerance may actually be interaction-related intolerance.
Especially with:
• clobazam
• phenytoin
• phenobarbital
So the polytherapy architecture matters as much as the molecule itself.
At present, the most reasonable way to view cenobamate is probably this:
An important newer option for drug-resistant focal epilepsy with promising efficacy data, but one that requires careful titration, interaction awareness, and patient selection.
No molecule replaces proper epilepsy classification, adherence assessment, sleep correction, surgical evaluation where appropriate, and rational long-term epilepsy strategy.
The goal is not only fewer seizures.
The goal is seizure control with preserved cognition, balance, function, and quality of life.
#Epilepsy #Neurology #Epileptology #Cenobamate #NeuroTwitter
Most temporal lobe seizures are not localised by one symptom in OPD.
Not by déjà vu.
Not by lip smacking.
Not by one abnormal EEG line.
They are localised by watching the seizure movie in order.
Think of TLE as a subway map.
Station 1: Aura Gate
Ask: what happened first?
Rising epigastric sensation, fear, déjà vu, smell or taste aura
Think mesial temporal.
Auditory buzzing, ringing, vertigo, sound in one ear
Think lateral temporal.
Station 2: Consciousness Station
When did the patient stop responding?
Temporal seizures often build gradually and leave confusion behind.
Absence is brief.
Frontal can be abrupt and dramatic.
Tempo matters.
Station 3: Automatism Junction
The mouth says temporal.
The hands may tell the side.
Lip smacking, chewing, swallowing
Temporal network.
Manual automatisms
Often ipsilateral.
Dystonic stiff arm
Contralateral.
One OPD question can be gold:
Which hand was fumbling, and which arm became stiff?
Station 4: Lateralisation Signal Box
Dystonia, clonus, forced version
Opposite hemisphere.
Postictal nose wipe
Same side.
Aphasia or postictal dysphasia
Dominant hemisphere.
Ictal speech or vomiting
Often non-dominant, but interpret with caution.
Station 5: Temporal-Plus Trap Exit
Some seizures only look temporal.
Think insula, operculum, orbitofrontal or TPO network when there is:
throat tightness
painful aura
perioral sensory symptoms
early hypermotor behaviour
discordant MRI, EEG and semiology
failed temporal surgery
The temporal lobe may be the platform.
The train may have entered from another line.
OPD rule worth saving:
Localise TLE by the movie:
First symptom
tempo
automatisms
lateralising signs
postictal language
EEG/MRI concordance
Not one sign.
The whole seizure sequence. #Neurotwitter #Medtwitter #TLE
1/3 🧠
L5 is neurologically awkward; it lacks a routinely emphasized reflex equivalent to the patellar-L4 or Achilles-S1
So most clinicians default to
- EHL weakness (big toe extension)
- sensory changes over the dorsum of the foot
- gait findings
when localizing L5 radiculopathy
A high CK is not the diagnosis.
It is only the entry ticket.
Inflammatory myopathy should be approached by pattern first, not by calling everything polymyositis.
First, look at the weakness.
Slow, asymmetric weakness with finger flexor and quadriceps involvement
Think inclusion body myositis.
Rapid proximal weakness with a CK volcano
Think immune mediated necrotizing myopathy, especially anti HMGCR or anti SRP.
Subacute proximal weakness with mechanic’s hands, Raynaud’s, arthritis or ILD
Think antisynthetase syndrome, especially anti Jo 1, PL 7 or PL 12.
Rash with or without weakness, sometimes even with normal CK
Think dermatomyositis, especially MDA5, TIF1 gamma, NXP2, Mi 2 or SAE.
Antibodies are powerful, but only when the phenotype agrees.
MRI tells you activity versus damage.
Biopsy still matters in seronegative cases, suspected IBM, poor steroid response or dystrophy mimics.
The real mistake is stopping at muscle.
Always ask about:
lung, skin, swallow, heart and cancer risk.
Myositis is not one disease.
It is a pattern recognition exam where the wrong lane can cost muscle, lung and time.
Pattern first.
Antibody next.
Biopsy when needed.
Screen beyond muscle.
Treat the subtype, not the CK.
#Neurotwitter #Medtwitter
Source: Allenbach Y, Benveniste O. Inflammatory Myopathies. NEJM, 2026.
Pragmatic. Full of information. Cutting edge. Cool figs!
Honored to lead The Lancet review on Encephalitis. With amazing Sophie B, Ava E, Kiran T & @DeannaSaylor1
We hope you enjoy reading it:
https://t.co/0baEHVhjeH
@mayoneurores@mayocliniclabs@MayoClinic@NDCNOxford
To call it or not to call it? That is the question!
Do you feel a bit wacky & wobbly when it comes to calling normal pressure hydrocephalus on imaging?
You don’t want to overcall it, but you don’t want to miss it either!
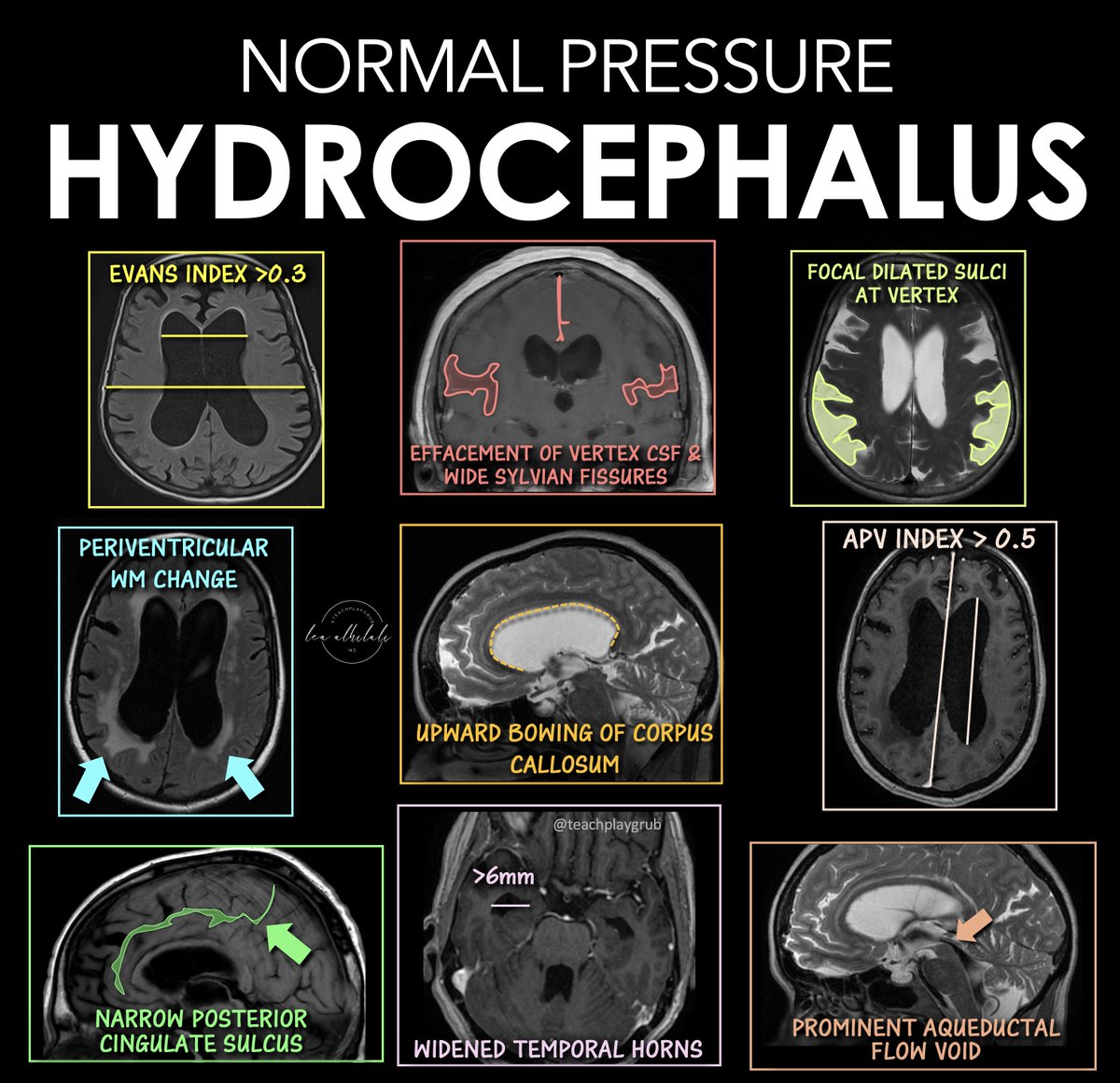
Here are the signs of NPH
🔹 Evans Index > 0.3
--Enlarged frontal horns relative to skull width → ventriculomegaly.
Remember it: “One out of three is too big for me!”
🔹 Periventricular White Matter Change
--T2/FLAIR hyperintensity from transependymal CSF flow.
Remember it: “Leaking pressure leaves a glow.”
🔹 Narrowing of the Posterior Cingulate Sulcus
--Tight high-convexity sulci from crowding at the vertex.
Remember it: “The top gets squeezed shut.”
🔹 Effaced Vertex CSF + Wide Sylvian Fissures
--Tight sulci up top but enlarged fissures laterally (DESH pattern).
Remember it: “Dry on top, wet on the sides.”
🔹 Upward Bowing of the Corpus Callosum
--Ventricular expansion pushes the corpus callosum upward.
Remember it: “If the corpus callosum is arched, the patient can’t march (wobbly)”
🔹 Temporal Horns > 6 mm
--Early temporal horn dilation from hydrocephalus.
Remember it: “Big horns before big vents.”
🔹 Focally Dilated Sulci at the Vertex
--Patchy enlarged sulci despite surrounding crowding.
Remember it: “Holes in a leaky roof = too much water on the brain!”
🔹 APV Index > 0.5
--Increased ventricular-to-parenchymal proportion suggesting hydrocephalus.
Remember it: “Glass half full is too much!”
🔹 Prominent Aqueductal Flow Void
--Increased CSF flow through the aqueduct on MRI.
Remember it: “If the aqueductal flow is super black, the ventricles are out of whack.”
Classic NPH imaging theme: enlarged ventricles + tight high convexities + disproportionate CSF redistribution.
Hopefully now you won't wobble on the diagnosis of NPH!!