$5,614.12 saved on a single CT scan.
Same procedure code (74177 — CT abdomen and pelvis with contrast). Two hospitals. One bill.
Physician-owned hospital (pays real estate taxes, gets no grants): $951.38 self-pay.
Non-profit hospital (pays no real estate taxes, receives federal and state grants): $6,565.50 cash price.
There's a lot of discussion lately about whether physician-owned hospitals inflate charges as massively as non-profits. This is one example from my personal experience. The "non-profit" charged nearly 7x more for the same scan than the for-profit physician-owned hospital.
Section 6001 of the ACA froze new physician-owned hospitals in 2010. The hospital lobby called it patient protection. The data calls it competition suppression.
We all got screwed when they stopped physicians from owning hospitals.
Section 6001 should be repealed.
Do your homework. Support the hospitals that help us. Avoid the ones that don't. Simple as 1-2-3.
#healthcarecosts #POH
On May 21, 2026, the House Ways and Means Committee passed H.R. 8163, the Provider Reimbursement Stability Act, sponsored by @RepGregMurphy (NC-03), co-chair of the @gopdoccaucus. Before I walk through the documented failures this bill addresses, I want to explain what it actually does. It has four specific provisions, and the mechanics behind each one matter.
The budget neutrality threshold has sat at $20 million since the Medicare Physician Fee Schedule was created in 1992. That number is the trigger that forces across-the-board cuts to all physicians whenever any single payment update exceeds it, including accurate corrections to undervalued codes. H.R. 8163 raises the threshold to $54.3 million and indexes it to the Medicare Economic Index every five years so it never falls this far behind again.
When CMS adds new codes to the fee schedule, it estimates how often they will be used and sets a budget neutrality adjustment based on that projection. When the estimates are wrong, the cuts they generate are permanent. No process exists to correct them. H.R. 8163 creates one.
Practice expense relative value units are supposed to reflect the real cost of running a clinical practice, including clinical staff wages, medical supplies, and equipment. The data inputs driving those calculations have no statutory requirement to be updated on any schedule. H.R. 8163 requires updates at minimum every five years.
The fourth provision limits year-to-year variance in the Medicare conversion factor to 2.5 percent. Independent practices have no institutional backstop to absorb sudden large cuts. This provision does not prevent cuts. It prevents cuts that arrive faster than a practice can respond.
None of these provisions add money to the system. They stop the system from generating cuts that have no clinical basis. This week I will walk through exactly what those failures have cost, including what CMS did in 2026 that made the underlying problem impossible to ignore.
We’ve agreed to a partnership with @SpaceX that will substantially increase our compute capacity.
This, along with our other recent compute deals, means that we’ve been able to increase our usage limits for Claude Code and the Claude API.
The Market Has Already Delivered Its Verdict. Only Organized Medicine Has Not.
The institutions that actually credential and reimburse physicians have spent the last three years reaching a conclusion about Maintenance of Certification that organized medicine refuses to acknowledge. These are not the specialty boards, not the AMA, and not the organizations that profit from mandatory participation. They are the bodies that determine whether hospitals and health plans operate with national accreditation, the federal agencies that govern competition in healthcare markets, and the commercial insurers that cover the majority of working Americans. Their verdict is documented in formal credentialing policy changes, updated accreditation standards, federal regulatory guidance naming unnecessary physician recertification as a potential antitrust violation, and bylaw amendments now adopted by more than 250 hospitals and health systems. It is not close and it is not preliminary.
Every major national accreditation body has formally recognized NBPAS as meeting its standards. The Joint Commission designated NBPAS as a Designated Equivalent Source Agency effective July 1, 2022, adding it to the glossary of accreditation manuals covering hospitals, ambulatory care, behavioral health, critical access hospitals, and office-based surgery facilities. The National Committee for Quality Assurance included NBPAS in its 2022 Health Plan Accreditation Standards and Guidelines. URAC, DNV, the Center for Improvement in Healthcare Quality, and the Accreditation Commission for Health Care have all confirmed that NBPAS meets their standards. Their collective recognition of NBPAS means that no credentialing or accreditation standard requires ABMS recertification as a condition of hospital or health plan operation. The ABMS gate is not an accreditation requirement. It is a private preference enforced through institutional inertia. ABMS's response to the Joint Commission's independent designation was to distribute what it called a toolkit created specifically to address what ABMS characterized as NBPAS's false inferences that an NBPAS certificate is equivalent to ABMS certification. The Joint Commission made that designation based on its own standards. ABMS responded by mounting a coordinated institutional campaign to undermine hospital recognition of an organization the nation's premier accreditor had just formally approved.
The federal signal arrived in April 2024, but its foundation had been laid seven months earlier. NBPAS formally filed a complaint with the FTC in September 2023, arguing that ABMS and its constituent boards were using monopoly power to exclude competitors from the continuing certification market. In April 2024, the FTC, DOJ, and HHS jointly launched https://t.co/o3T1CwXKrf, a portal for public reporting of anticompetitive practices in healthcare, and explicitly listed unnecessary healthcare provider recertification or accreditation requirements as an example of potentially anticompetitive conduct that may raise the costs of practicing medicine and reduce the number of healthcare practitioners. The sequence is clear. NBPAS filed the complaint. Seven months later, the federal government launched a portal naming the exact conduct NBPAS had identified. Three months after that, in July 2024, CMS updated its guidance on End Stage Renal Disease Medical Directors to formally accept NBPAS-certified nephrologists, including in rural areas and federally-designated Health Professional Shortage Areas. The federal government identified mandatory physician recertification as a potential antitrust violation and then changed its own clinical guidance in the same direction within the same year.
The three largest commercial insurers have followed. UnitedHealthcare, the largest health insurer in the United States, formally confirmed in a letter to NBPAS that its credentialing policies do not require participation in MOC programs, that physicians certified by NBPAS may be credentialed under its existing policies, and that physician competency is best demonstrated through initial board certification, ongoing clinical practice, and a commitment to lifelong learning. That statement is a precise repudiation of the ABMS mandatory recertification model, delivered in writing by the organization that insures more Americans than any other. Elevance Health, formerly Anthem, operates Blue Cross Blue Shield plans in 14 states and covers more than 115 million lives. Elevance accepts NBPAS under its alternative credentialing criteria for physicians with ten or more years of clinical experience. Health Care Service Corporation, the largest customer-owned health insurer in the United States, operating Blue Cross Blue Shield plans in Illinois, Montana, New Mexico, Oklahoma, and Texas, formally accepts NBPAS board certification. Blue Cross Blue Shield of Massachusetts, a five-star NCQA-rated plan, has accepted NBPAS. The American Thoracic Society has added NBPAS as a recognized board certification option in its professional database.
Hospital adoption is accelerating entirely through physician-led bylaw amendments, requiring no legislation and no institutional permission beyond a Medical Executive Committee vote. NBPAS is now recognized by more than 250 hospitals and health systems nationwide. Forty-four hospitals added NBPAS to their bylaws in 2025 alone. Named institutions include HCA Florida Woodmont Hospital, Ascension Saint Thomas hospitals in Tennessee, WVU Medicine, hospitals in the ScionHealth network, Hackensack Meridian Health in New Jersey, and St. Joseph's Health Hospital in Syracuse. Most hospitals, as NBPAS has documented, simply were not aware that an alternative existed.
The single most instructive holdout is Blue Cross Blue Shield of Michigan. Despite a physician-led campaign of more than 40 formal requests, intervention from Governor Whitmer's office, and a direct response request from the Michigan Department of Insurance and Financial Services, BCBSM refused to remove its MOC requirement. BCBSM holds more than 80 percent of the commercial insurance market in Michigan. That market concentration means a single insurer's refusal to recognize NBPAS functions as an effective statewide prohibition regardless of what any hospital bylaw or state legislature has done. Dr. Robert Vanderbrook is a solo family medicine physician in Clare, Michigan, practicing in a federally-designated Health Professional Shortage Area, which is a community the federal government has formally identified as lacking adequate physician access. BCBSM removed him from its networks because he chose NBPAS over ABFM recertification. Many of his patients refused to go elsewhere and opted to pay out of pocket to continue seeing him regardless of the financial strain. The BCBSM position is not an argument for the ABMS patient safety rationale. It is an illustration of what market-dominant enforcement of a discredited mandatory program looks like when it lands on a real physician in a real community that cannot afford to lose him.
The state legislative map tells the same story the market has told. Fifteen states have now passed laws limiting or restricting MOC requirements as a condition of physician practice. Six of them (Oklahoma, Texas, Georgia, South Carolina, Arkansas, and Tennessee) have passed comprehensive legislation prohibiting state licensing boards, insurance providers, and hospitals from requiring MOC participation as a condition of licensure, hospital privileges, or insurance panel participation. Oklahoma was first in 2016. Texas followed, with a bill signed by Governor Greg Abbott and sponsored by two physician-legislators: Senator Dawn Buckingham, MD, and Representative Greg Bonnen, MD. Georgia, South Carolina, and Arkansas followed. Nine additional states (Washington, Arizona, North Carolina, Kentucky, Missouri, Maine, Maryland, and others) have passed starter legislation, typically beginning with the licensure provision and building from there. More than a dozen others have introduced legislation that is pending or has expired in prior sessions. The pattern is consistent: a state begins with a narrow bill, builds legislative familiarity with the issue, and returns the following session with broader protections. The AMA's formal policy position has not changed. The enforcement infrastructure beneath it is being systematically removed, one state at a time.
Texas is the most instructive case study because it shows both the momentum and the remaining friction in a single legislative cycle. Texas SB 2207, which would have allowed NBPAS-certified physicians to truthfully advertise as board certified with full disclosure of their certifying board's name, passed the Senate Health and Human Services Committee unanimously at 7-0, passed the full Texas Senate 29-2, and passed the House Public Health Committee 9-1. The bill did not reach a House floor vote before the session ended. In a session where more than 7,000 bills were introduced and only 437 became law, SB 2207 ran out of calendar time rather than political support. The TMA's official policy states it opposes mandatory MOC requirements for licensing, health plan contracting, and hospital credentialing, citing excessive cost, time away from patients, and lack of sufficient research documenting benefits to patient care. Notwithstanding that official position, the TMA testified against SB 2207 before the House Public Health Committee on May 12, 2025, a hearing that ran through the night and concluded testimony at 2:30 in the morning. Physicians who had driven hours to testify in support could not wait out the schedule.
At the TMA's House of Delegates meeting in April 2026, physician members introduced Resolution 202, which would have required the TMA to support efforts to amend Texas Medical Board advertising rules to allow NBPAS-certified physicians to advertise as board certified. The resolution came within two percentage points: 48 percent in favor, 52 percent opposed. That vote is a leading indicator. Nearly half of the TMA's own physician delegates voted to require their association to stop opposing legislation their colleagues in the Texas Senate supported 29-2. The trajectory of that number across future sessions is the story. The AMA holds its formal policy. The states are moving regardless and within the state medical associations themselves, the physician membership is closing the gap between what organized medicine says and what practicing physicians actually want.
The policy argument for Congress, state legislatures, and hospital medical staffs is now straightforward. The market, the federal regulators, and every national accreditation body have reached their verdict. The largest commercial insurers have concluded in writing that mandatory ABMS MOC is not necessary for physician credentialing. The FTC and DOJ have named unnecessary physician recertification as a potential antitrust violation. The Joint Commission, NCQA, URAC, and DNV have all recognized the alternative. Two hundred and fifty hospitals have made the bylaw amendment. Fifteen states have passed legislation. The only institutions still treating ABMS MOC as the exclusive and mandatory pathway are the ABMS itself, the AMA, and a handful of insurers with sufficient market dominance to enforce a requirement the rest of the market has abandoned. What remains is not a debate about evidence or patient safety. That debate is over. What remains is finishing the work.
The AMA Built the Monopoly, Wrote the Standard That Protects It, and Applied That Standard to Block the Only Competition
The American Medical Association established the American Board of Medical Specialties in 1933. That founding relationship is not historical background. The AMA today holds a delegate vote in the ABMS General Assembly, places representatives on ABMS committees, and owns the AMA PRA Category 1 Credit designation that ABMS member boards require physicians to fulfill as their mandatory CME standard. The Accreditation Council for Continuing Medical Education, a separate organization, accredits the specialty societies and academic medical centers authorized to sell the qualifying activities. The AMA owns the required credit standard. The ACCME accredits the providers selling the products that satisfy it. Many of those ACCME-accredited providers are the same specialty societies that govern the ABMS boards setting the requirements in the first place. Every spot in that circuit has a financial interest in mandatory physician participation. When the AMA issues official policy defending ABMS as the definition of legitimate physician certification, it is defending an institution it built, whose mandatory requirements generate revenue through a system the AMA controls the standard for, and whose commercial infrastructure the AMA's governance participation has helped entrench for nearly a century.
The tax designations of the organizations in this system are worth stating precisely because they are revealing. ABMS, the parent body, is organized as a 501(c)(6) business league under the IRS code, which is the same category as chambers of commerce and trade associations, created for the improvement of business conditions among members. Its individual member boards, including ABIM, are organized as 501(c)(3) charitable organizations, the designation reserved for entities serving a public benefit. A 501(c)(6) is expected to serve member business interests. A 501(c)(3) is expected to serve the public. ABIM claims the charitable designation while operating a mandatory commercial fee program, paying its CEO $1,385,563 annually, and running a patient-facing website that falsely labels physicians who have chosen a competing credential as no longer certified. The gap between the designation and the conduct is not incidental. It is the operating model.
The financial numbers are drawn directly from ABIM's IRS Form 990 for the fiscal year ending June 2023, available through ProPublica's Nonprofit Explorer. ABIM reported $90 million in total revenue, derived almost entirely from certification and recertification fees. Its 283 employees received $39 million in total compensation averaging $138,000 per employee. Richard Baron, President and CEO, received $1,385,563 in fiscal year 2023 alone. His cumulative compensation from ABIM over the six years from 2018 through 2023 totaled $7 million. Across all 24 ABMS member boards, the combined net balance grew from $237 million to $642 million between 2004 and 2014, a $405 million increase funded entirely by mandatory physician fees. A cost analysis published in the Annals of Internal Medicine by Sandhu, Kazi, and colleagues at UCSF found that ABIM's MOC program costs an average of $23,607 per physician over ten years. The overwhelming majority of that cost represents the monetized value of approximately 180 hours of physician time extracted from clinical practice. ABIM had previously characterized the program as costing $200 to $400 per year. Independent economic modeling showed a figure more than ten times that when physician time is properly accounted for. The ABMS spent $80,000 on federal lobbying in 2023 on issues described in its own filings as related to high quality physician certification, per OpenSecrets federal lobbying disclosures. A 501(c)(6) business league spending federal lobbying dollars to protect mandatory commercial recertification requirements it helped embed in the Affordable Care Act, while its member boards collect fees under a 501(c)(3) charitable designation, is not operating as a quality assurance system. It is operating as a market protection enterprise with a charitable tax shield.
The ongoing recertification costs do not capture the full financial picture because they exclude what ABMS extracts at the point of entry. A Health Affairs analysis framed board certification as a two-sided market in which hospitals require certification for granting specialty-specific privileges, forcing physicians to purchase not only initial certification but also MOC and recertification from a near-monopoly market as a means of access to continued employment. The entry cost alone is substantial. A new heart failure cardiologist completing fellowship training faces direct certification fees of $7,145 for boards in internal medicine, cardiology, and heart failure cardiology, on top of a median of $190,000 in medical school debt that grows to approximately $325,000 over the seven years of post-medical school residency and fellowship training. These are the economic conditions under which ABMS then introduces mandatory ongoing recertification fees. The financial barrier is not limited to the recertification cycle. It begins at the career entry point and compounds from there.
The Accreditation Council for Graduate Medical Education adds a third institutional layer to this system that is rarely discussed in the context of board certification reform. ACGME accredits and controls all graduate medical education for MDs and DOs in the United States. Taxpayers fund graduate medical education through ACGME-accredited programs at a rate exceeding $15 billion per year. ACGME requires current board certification, meaning ABMS MOC participation or grandfathered status, as a condition of holding an ACGME-accredited faculty position. When NBPAS formally requested that ACGME remove this requirement, ACGME responded by asking NBPAS to complete an evaluation checklist that included criteria only organizations offering initial board certification could meet. This is identical to the circular standard the AMA applies in H-275.926. NBPAS submitted a statement to the House Judiciary Antitrust Subcommittee in May 2025 describing ABMS and ACGME as having created a vertically integrated, self-reinforcing system that blocks competition, limits physician autonomy, and misuses taxpayer-funded resources. The public is funding, through $15 billion in annual federal GME dollars, the pipeline that produces the physicians the ABMS mandatory commercial program then captures at the point of career entry.
The specific AMA policy ABMS deploys to block the National Board of Physicians and Surgeons is H-275.926, Medical Specialty Board Certification Standards. It requires that any certifying body recognized as equivalent to ABMS must offer an independent, external assessment of knowledge and skills for both initial certification and recertification or continuous certification in the medical specialty. NBPAS is disqualified on the first count: it does not administer its own initial certification examinations. ABMS cited this policy explicitly in its public statement opposing NBPAS recognition.
The problem with that disqualification is that NBPAS does not ignore initial certification. It treats prior ABMS or AOA board certification as a non-negotiable prerequisite for entry, with no exceptions. NBPAS was founded by and structured around physicians who have passed the ABMS initial certification examination, and it is premised on the view that the ABMS initial examination is a genuine professional threshold worth preserving. The AMA's standard penalizes NBPAS for endorsing the ABMS examination as the gold standard and declining to duplicate it independently. Any organization that attempted to offer its own competing initial certification examination would face immediate and far more aggressive institutional resistance from ABMS, ACGME, and the hospital credentialing infrastructure those organizations have built together. The standard was not designed to establish a quality threshold. It was designed to describe what ABMS does and disqualify everything that does not fully replicate it.
The second disqualifying ground has collapsed from within. The claim that NBPAS's recertification pathway does not constitute an independent external assessment of knowledge and skills is now inconsistent with what ABMS's own member boards require of their own diplomates. As of September 2024, eight of the 24 ABMS member boards no longer offer a traditional secure examination for recertification at all. Three more use it only for re-entry. The ABMS's own published standard for continuing certification, effective January 2024, replaced the 10-year high-stakes exam with modular and longitudinal assessments system-wide. Consider the American Board of Orthopaedic Surgery. ABOS administers a Web-Based Longitudinal Assessment in which it assigns specific journal articles to diplomates and requires them to answer questions on those articles to maintain certification. A diplomate who is a hand surgeon, a pediatric orthopaedic surgeon, or a spine specialist tests on content ABOS has chosen regardless of whether those articles bear any relationship to their actual clinical practice. This is what the AMA's H-275.926 accepts as an independent external assessment of knowledge and skills. NBPAS requires 50 hours of AMA PRA Category 1 CME in the physician's specialty every 24 months, with the physician selecting CME activities relevant to what they actually do clinically. The distinction between what ABOS requires and what NBPAS requires is not one of rigor or patient protection. It is one of who selects the content and who collects the fee.
The ABMS does not limit its opposition to policy documents and lobbying arguments. It operates CertificationMatters, a patient-facing website that displays the message "Your Doctor Is No Longer Certified" when patients search for physicians who have chosen NBPAS over ABMS recertification. These physicians hold valid unrestricted medical licenses. They have passed ABMS initial certification examinations. They meet NBPAS's documented CME requirements. The not certified label is false on its face. It is an active public misinformation campaign designed to drive patients away from physicians who have exercised a legally protected professional choice, deployed by an organization using patient safety language to accomplish what policy and lobbying cannot: the commercial exclusion of a competitor that the Joint Commission, NCQA, URAC, and DNV have all formally recognized.
There is also a direct antitrust dimension to how H-275.926 functions. Physicians and legal scholars have documented that ABMS's initial certification monopoly and its mandatory ongoing MOC program constitute a tying arrangement. Under that arrangement, one product, initial certification, is tied to a second product, ongoing maintenance fees, under threat of professional exclusion. NBPAS breaks that tie. It accepts the ABMS initial certification as the entry threshold and offers a different, less expensive, less burdensome pathway for what follows. The AMA's H-275.926, by requiring that any legitimate alternative offer both initial and ongoing certification, mandates that any competitor replicate the entire ABMS bundle rather than compete on any component separately. That is a structural protection for a bundled monopoly, written by the organization that founded and continues to govern the monopoly it is protecting. A class action lawsuit filed in 2025 against ABIM's policies blocking osteopathic physicians from serving as internal medicine residency and fellowship directors without ABIM certification adds further dimension to that structure. The suit argues that this restriction channels trainees toward ABIM certification while excluding qualified DO physicians from academic leadership roles, limiting competition and restricting access to academic employment. The certification gate does not only affect practicing physicians. It shapes who trains the next generation of them.
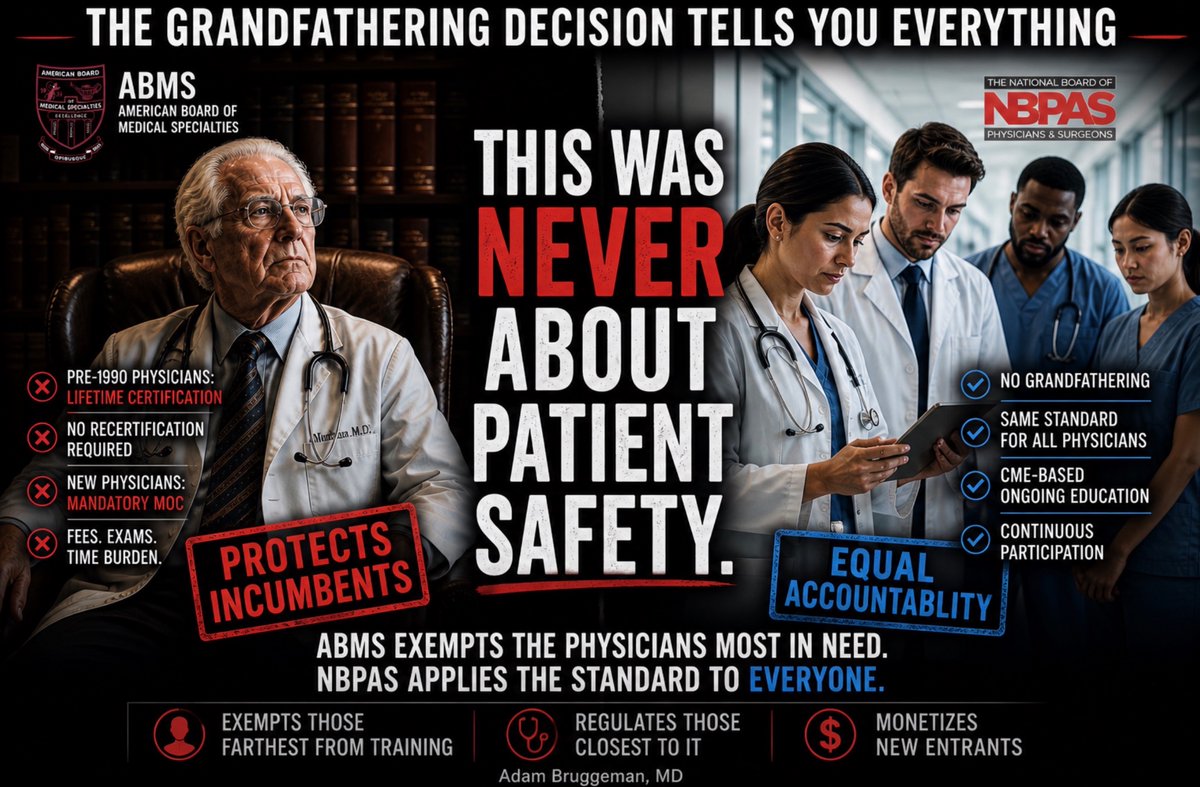
Maintenance of Certification Controversy - The Impact of the Grandfather Clause
When the American Board of Medical Specialties introduced Maintenance of Certification requirements in 2000, it faced an immediate question: which physicians needed ongoing recertification most urgently? The answer, under any honest patient safety rationale, was obvious. The physicians most likely to be practicing outside current clinical standards were those whose training was farthest removed from contemporary evidence-based medicine. These were the senior physicians who had completed residency in the 1960s and 1970s and whose foundational medical education predated three decades of pharmacological, surgical, and diagnostic transformation. If the purpose of ongoing recertification was patient protection, those were the physicians the program should have reached first.
ABMS grandfathered them entirely. Physicians who had obtained initial board certification before 1990 received permanent, non-expiring credentials with no ongoing recertification obligation. The mandatory commercial program was built around the physicians who had trained most recently. These were the physicians whose knowledge base was most current, who had just completed ACGME-accredited residencies and passed rigorous initial certification examinations. The patient protection rationale, applied honestly, demanded the opposite. The grandfathering decision at launch tells you what the program was actually designed to do.
That decision was not corrected as the program matured. It was institutionalized. The American Medical Association, which founded ABMS in 1933 and retains a delegate vote in the ABMS General Assembly today, has codified grandfathering as permanent policy in H-275.924 Principle 23, which explicitly states that physicians with lifetime board certification should not be required to seek recertification. The organization that built ABMS defends it against every reform effort and owns the AMA PRA Category 1 Credit designation that ABMS member boards require physicians to fulfill as their mandatory CME standard. It has officially and permanently protected the cohort of physicians the patient protection argument would most urgently cover. That means this is not about legacy protections but instead an institutional commitment to an arrangement that has never been about patient safety.
The National Board of Physicians and Surgeons, the organization the AMA has disqualified from recognition, explicitly prohibits grandfathering. NBPAS holds every physician who seeks its certification to the same 24-month CME documentation requirement regardless of when they trained, how long they have been in practice, or what year they completed residency. The Practical Neurology summary of NBPAS's Joint Commission recognition states this directly: NBPAS prohibits the discriminatory practice of grandfathering, which gives lifetime elite status without recertification requirements to a significant portion of US physicians. The organization the AMA has disqualified using patient protection language is the only certifying body in the country that applies the patient protection rationale without exception. The organization the AMA protects exempts the physicians the patient protection rationale would most urgently cover.
This is the efficient demolition of the ABMS patient safety argument, and it requires only the structural choices ABMS and the AMA made themselves. It needs no external critique. The grandfathering decision at launch, the AMA's codification of it as permanent policy, and NBPAS's explicit prohibition of it together establish that the mandatory commercial recertification program was designed to extract fees from new entrants while protecting incumbents. It was not designed to ensure that the physicians treating patients today are current in their specialty knowledge.
On April 30, 2026, the Department of Justice and the Federal Trade Commission issued a joint letter to the Tennessee Supreme Court describing the American Bar Association's exclusive accreditation authority over law schools as a monopoly. The letter documented that the ABA's governance is dominated by parties with financial interests in limiting competition, that its standards exceed any defensible baseline, and that its history includes documented antitrust violations. The ABMS has a concerning similarity to that description. Paul Teirstein, MD, the cardiologist who founded NBPAS, described the ABMS precisely in a Wall Street Journal op-ed published October 19, 2025: a private nonprofit entity that operates like a regulator, controlling a credential held by nearly 95 percent of practicing physicians, required by most hospitals and insurers as a condition of employment, with no accountability to the physicians or patients it claims to serve. The combined net balance of all 24 ABMS member boards, which are all 501(c)3 nonprofits, grew from $237 million in 2004 to $642 million in 2014. The American Board of Internal Medicine alone reported $90 million in revenue in fiscal year 2023, with its President and CEO receiving $1,385,563 that year and $7 million over the preceding six years.
The program was embedded into the Affordable Care Act (ACA) through federal lobbying while ABMS was simultaneously lobbying Congress on its own behalf. You might ask how the ACA codified ABMS certification. The ACA wrote a statutory definition of maintenance of certification that matched the ABMS program, then CMS attached a Medicare bonus payment through PQRS quality reporting of ABMS participation on top of that statutory definition. The taxpayer-funded bonus flowed exclusively to ABMS-certified physicians participating in ABMS MOC. The DOJ and FTC just drew the legal and policy map for challenging exactly that kind of structure. This week I am making the case for reform.
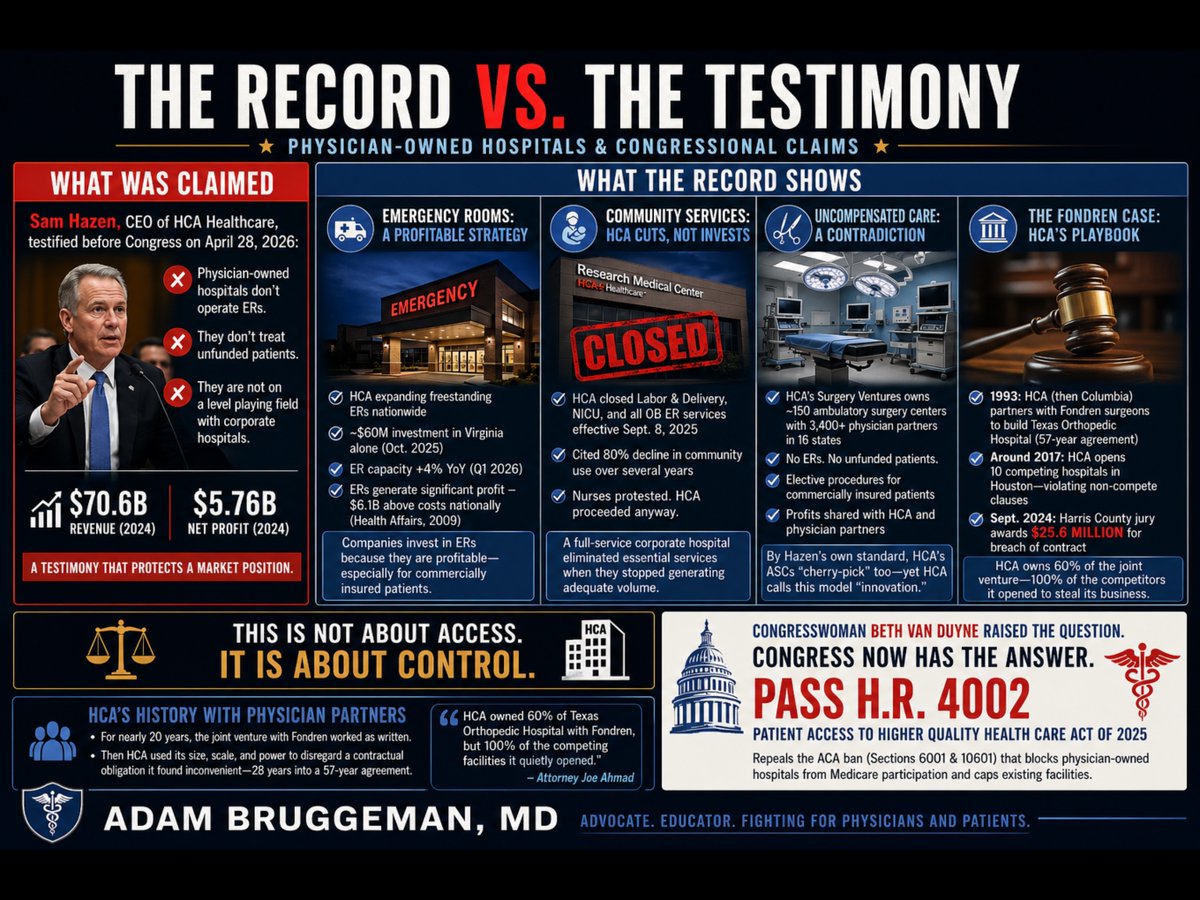
Yesterday, Sam Hazen, CEO of HCA Healthcare, sat before the House Ways and Means Committee and argued that physician-owned hospitals are not on a level playing field with corporate hospitals because they lack functioning emergency rooms and do not treat unfunded patients. Hazen delivered this argument while representing a company that posted $70.6 billion in revenue and $5.76 billion in net profit in 2024. He was not offering a neutral observation about healthcare access. He was protecting a market position.
Congresswoman Van Duyne did not let the testimony pass unchallenged. She pointed directly to HCA's own Research Medical Center in Kansas City, Missouri, which closed its labor and delivery unit, its neonatal intensive care unit, and all associated obstetrics emergency services effective September 8, 2025. HCA cited an 80 percent decline in community use of those services over several years as its justification. Nurses at the facility publicly protested the planned shutdowns and called on HCA to reverse course. HCA proceeded anyway. That is a full-service corporate hospital making a purely financial decision to eliminate essential community services when they stopped generating adequate volume. The same CEO who told Congress that physician-owned hospitals fail community obligations made that decision.
The emergency room argument deserves particular scrutiny. Mr. Hazen's implication is that operating an ER is a financial burden that justifies the premium reimbursement HCA collects across its outpatient system. The capital record contradicts that framing entirely. In January 2024, Hazen personally told HCA investors that the company's freestanding emergency room capacity would "grow consistently" in 2024 and 2025 to meet rising patient demand. In October 2025, HCA committed nearly $60 million to construct three new freestanding emergency rooms in Virginia alone, expanding its footprint there from eight to eleven standalone ER facilities. HCA has simultaneously been opening freestanding ERs in South Carolina, Florida, and throughout its other markets. In the first quarter of 2026, HCA reported that its emergency room capacity grew 4 percent year-over-year. A peer-reviewed analysis published in Health Affairs found that hospital emergency department revenue exceeded costs by $6.1 billion nationally as far back as 2009, a margin of 7.8 percent overall, with privately insured ED patients generating $17 billion in profit. Companies do not invest tens of millions of dollars in freestanding emergency infrastructure because that infrastructure is a burden. They expand aggressively into emergency care because it is profitable, particularly for commercially insured patients. When physician-owned hospitals choose not to operate ERs, they are not avoiding a community obligation. They are declining to compete in HCA's most profitable and most aggressively expanded service line.
The uncompensated care argument carries an equally significant contradiction. Through its Surgery Ventures division, HCA jointly owns and operates approximately 150 ambulatory surgery centers with more than 3,400 physician partners across 16 states. Those ambulatory surgery centers have no emergency rooms. They do not accept unfunded patients. They perform elective procedures on commercially insured patients and return profits to both HCA and its physician co-owners. By the precise standard Mr. Hazen applied to physician-owned hospitals before the Ways and Means Committee, his own company's Surgery Ventures facilities are doing exactly what he described as an unfair advantage. The distinction HCA is actually drawing is not between facilities that serve whole communities and those that do not. It is between facilities that HCA controls and those that it does not. When physicians own a hospital independently, HCA calls it cherry-picking. When HCA installs those same physicians as partners in ASCs under its corporate umbrella, it calls it innovative care delivery.
The history of how HCA treats physician partners outside of its direct control is documented in a Harris County, Texas courtroom. Fondren Orthopedic Ltd., a group of orthopedic surgeons, entered a limited partnership with what was then Columbia Hospital Corporation in 1993 to jointly own and operate Texas Orthopedic Hospital in Houston. The agreement ran for 57 years. For roughly two decades it functioned as written. Around 2017, HCA, which had assumed Columbia's position, began employing orthopedic surgeons at competing facilities across the Houston area, ultimately opening 10 competing hospitals offering the same services as the joint venture, in direct violation of the non-compete provisions of the partnership agreement. Simultaneously, HCA invoked those same non-compete clauses against the Fondren physicians, blocking them from doing what HCA was openly doing. In September 2024, a Harris County jury returned a verdict of $25.6 million against HCA for breach of contract. Lead attorney Joe Ahmad stated publicly that HCA owned 60 percent of Texas Orthopedic Hospital with Fondren, but 100 percent of the competing facilities it quietly opened to redirect patients away from their jointly held hospital. The jury found that HCA had the size, the scale, and the power to disregard a contractual obligation it found inconvenient, approximately 28 years into a 57-year agreement.
The legislative response is already written. H.R. 4002, the Patient Access to Higher Quality Health Care Act of 2025, introduced by Congresswoman Van Duyne and Congressman Henry Cuellar (D-TX-28), would repeal Sections 6001 of the Affordable Care Act, which banned new physician-owned hospitals from Medicare participation in 2010 and capped existing facilities at their March 2010 capacity. That ban was not derived from patient outcome data. It was a lobbying achievement. The evidence accumulated in the 15 years since passage shows that physician-led facilities consistently deliver care at lower cost with higher patient satisfaction than large corporate systems.
Thank you @RepBethVanDuyne for being a champion for patients, physicians, and communities!
Dr Oliverson is completely right
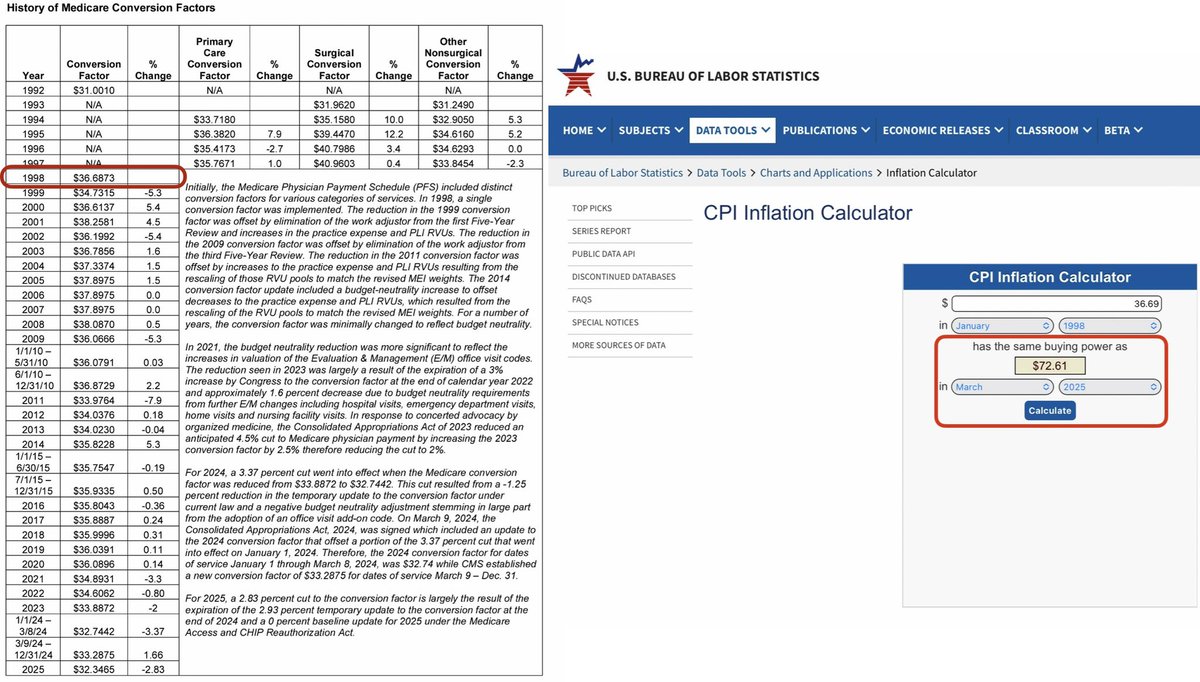
In 1998, the Medicare conversion factor was $36.69 for physicians. In 2025, just with inflationary updates, that number would be $72.61. It was $32.35.
The AMA graph shows that hospitals are roughly at consumer inflation
What isn’t accounted for is additional facility fees that hospitals make when physicians are employed in their facilities. Those numbers are 3x what a physician makes under Medicare and even greater under private health insurance.
@IndeMedAction
“I didn’t write those penalties.” - Pete Stark
The Stark Law prohibits a physician from referring patients to an entity in which they have a financial interest. That sounds neutral but it isn’t.
A hospital-employed orthopedic surgeon who refers every post-operative patient to the hospital’s owned SNF, physical therapy, imaging center, and home health agency has a financial interest in every one of those referrals. His salary, his productivity bonus, and his continued employment depend on staying within the system. None of that triggers Stark. The bona-fide employment exception covers it entirely.
An independent orthopedic surgeon who owns an MRI with two partners? Well, they would have to go through a full stark analysis and legal review with complex written arrangements and ongoing compliance infrastructure. One technical violation of Stark and the False Claims Act exposure is existential.
These scenarios show the same financial conflict with radically different legal treatment.
The consequences for patients are hard to ignore. A recent NORC survey found that 61% of employed physicians have moderate or no autonomy to make referrals outside their system, and nearly half said they adjust treatment options based on organizational incentives. Hospital employment doesn’t eliminate the financial conflict of the referral relationship. It just hides it inside a compensation structure Stark never touches.
Marc Greenberg, MD, an orthopedic surgeon in Baltimore, put it plainly in Becker’s this week: “We’ve created a system where for-profit entities can have healthcare ownership. But the people who took an oath to serve the patient — who’ve shown a commitment to caring — can’t.”
There is no federal prohibition on hospitals requiring employed physicians to refer within the system. No law prevents health systems from structuring compensation, call coverage, or scheduling to steer referrals to owned facilities. No equivalent of Stark governs the institutional referral relationship at all.
Congressman Stark was trying to protect patients from corrupted referrals. What his law produced was a system where the most powerful referral relationships in American healthcare are completely unregulated and the physicians most accountable to patients are the ones most restricted.
Oh come on…
On self-referral “conflict of interest”: The Stark Law already governs physician self-referral. POH physicians must publicly disclose their ownership interest to every referred patient.
Now… what do hospital controlled doctors disclose?? Nothing. They have zero disclosure obligation when they refer patients to the same corporate system that signs their paycheck. They are systematically incentivized to use higher-cost outpatient hospital settings rather than independent facilities. A 2020 Journal of General Internal Medicine analysis of Texas BCBS claims found hospital-owned physician practices generated 5.8% higher annual spending, 13% higher imaging costs, and 21.7% higher outpatient facility costs than independent practices, driven entirely by utilization and site-of-service billing. If the concern is financial conflicts driving utilization, the data points to hospital consolidation, not physician ownership.
On the “data is clear” claim about cherry-picking: The data is actually clear in the opposite direction. The 2015 BMJ study examined 219 POHs and 1,967 non-POHs across 95 hospital referral regions and found Medicare patient proportions were statistically identical with 47.1% at POHs versus 47.2% at non-POHs. Medicaid proportions were 14.9% versus 15.4%. Minority patient proportions were similarly equivalent. The 2024 Physicians Advocacy Institute analysis of 20 high-cost DRGs found no evidence of cherry-picking after controlling for patient age, race, and health status. At the same time they found POHs delivered care at 8-15% lower Medicare cost per episode. The 2023 JAMA Network Open study found POHs had 17.5% lower commercial negotiated prices and 46.7% lower cash prices in the same geographic markets. The “cherry-picking” narrative collapses under peer-reviewed scrutiny.
On rural hospital harm: The FAH report this argument relies on was commissioned by the Federation of American Hospitals and the American Hospital Association. It is a modeled simulation based on hypothetical scenarios, not observed real-world outcomes. The legislation in question (H.R. 2191) specifically requires a 35-mile separation between a new POH and any existing rural hospital, which is a provision designed precisely to avoid the competitive overlap this model assumes. More importantly, 152 rural hospitals have closed since 2010 (when the POH ban took effect). The ban did not protect rural access. It accelerated consolidation, reduced competition, and drove up costs. Markets with POHs have 16.7% lower concentration scores than markets without them. The real threat to rural hospitals is a Medicare reimbursement structure that already produces -11.8% Medicare margins for sole community hospitals. Fixing that requires payment reform, not protecting incumbent hospital systems from physician-led competition.
What’s perhaps not discussed enough is that nearly every procedure performed in hospitals today is subject to utilization review (prior authorization). If someone is looking over the claim to make sure it is indicated and medically necessary, all of these arguments go away anyway. It doesn’t matter if the physician takes the procedures to their own facility, particularly if the physician hospital provides the same or better quality and the same or lower price.
The ACA Section 6001 ban on physician ownership was legislative horse-trading, so let’s not pretend to take some high road that this is about protecting patients. Fifteen years later, consolidation has accelerated, patient choices have narrowed, and the organizations lobbying hardest to keep the ban are the ones profiting most from it.
@RooshWilliams Bro watched y'all video on LOR today only for our first two shots today to be a
1) Sengun Flamingo Fadeaway
2) Amen Thompson brick
LMFAO
It could all be so simple.
Use Reed as our primary PG. Have the Reed PnR be our primary action, with Amen operating off the baseline.
KD can run the secondary action off of that.
I guarantee you that we'd generate much more efficient offensive possessions.
4) Sengun mismatch on the defender that switched up on him.
Lastly, you'd get secondary action as defenders are scrambling to get right wherever they were wrong