Child dead from a perforated appendix, peritonitis, sepsis after an ANP played Dr in ED
Fever, vomiting, tachycardia, 10/10 pain. No bloods,urine, no proper obs, transcription error hid the fever. Enema for “constipation” and sent home. NO SENIOR REVIEW
This needs to STOP 🛑
This is the sad reality of a normal day in the NHS. No strikes, No excuses.
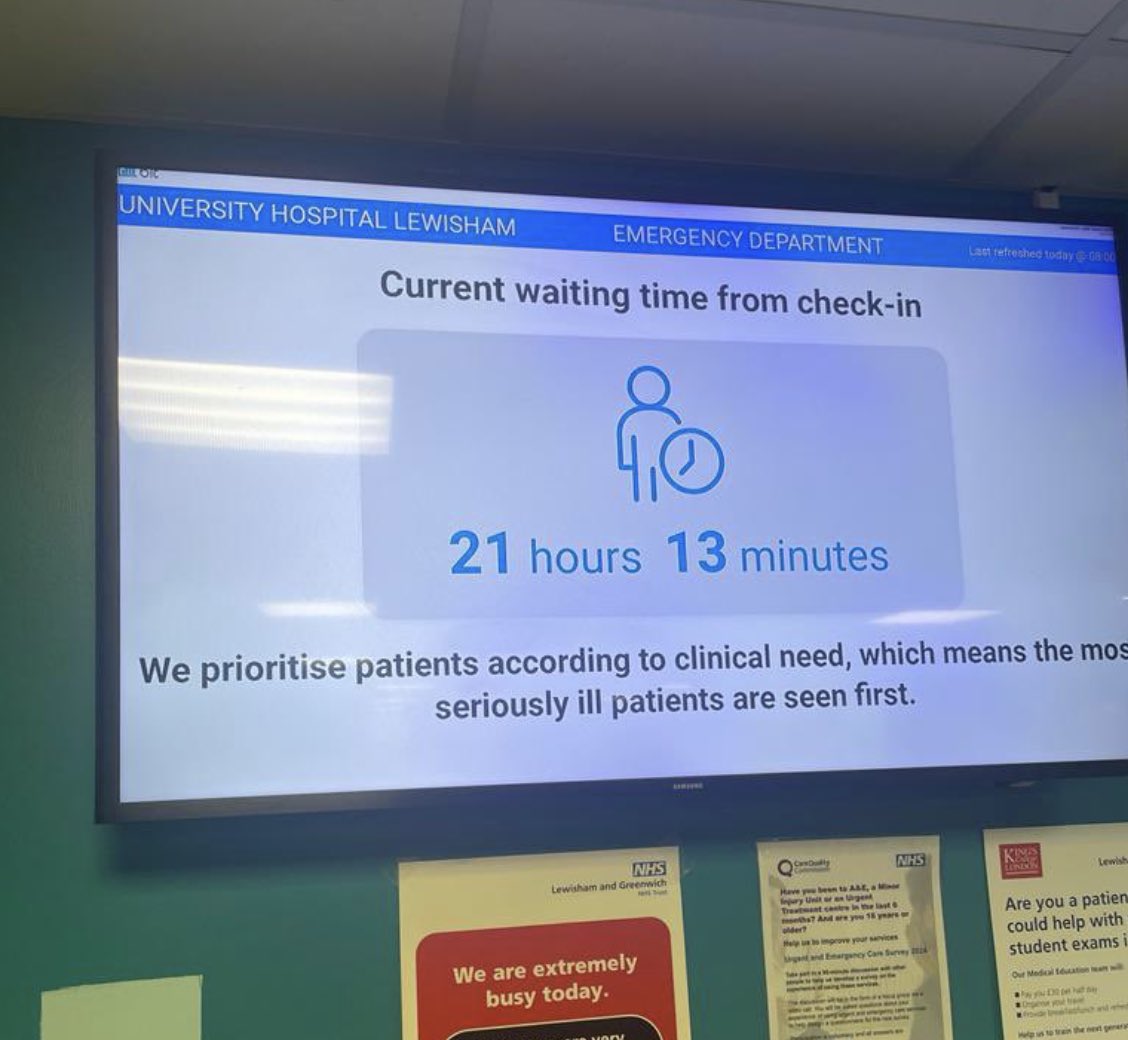
Yet we’ve got fully qualified doctors sitting unemployed while patients are left waiting 21 hours in A&E.
Years of mismanagement and catastrophic workforce planning failure.
What a betrayal to patients
If resident doctors end up striking again in this dispute on jobs and pay, remember;
1. This 21 hour wait at a London A&E outside winter or any strike action.👇🏼
And;
2. The fact that 8555 resident doctors have been turned away from emergency medicine in late 3 years alone.
The UK GOVERNMENT cannot imagine paying DOCTORS the global going rate or hiring similar numbers of doctor per 100,000 patients as comparator countries, but can imagine cutting the number of specialist training places for doctors. This is perverse.
People in the UK need to wake up. This thread explains how the government is using the GMC to remove the requirement for consultant surgeons, anaesthetists, and physicians to be medically qualified. @ShaunLintern surely this should worry you and your readers?
- there is only ONE nurse in Europe allowed to perform ERCP (usually carried out only by specially trained surgeons), in Rotherham in England
- this nurse regularly introduced himself as ‘a consultant interventional radiologist’ to patients, obfuscating the fact he’s a consultant NURSE
- even his supervising surgeons were not themselves trained in ERCP as it’s so specialised!
- in one case he continued with surgery despite the supervising doctor instructing him to stop
- he made mistakes dosing sedatives and I n the procedure itself, leading to the death or harm of at least 68 patients
Doctors wanting to perform ERCP must pass rigorous speciality exams and enter special training programmes under close supervision. Why do we have lesser standards for nurses?
Patients must now routinely ask their ‘doctors’ if they are actually doctors if they want proper care in the uk!
Dr Elaine is the UK’s first deaf/blind doctor. She is under multiple specialists in London. She is on 24 hour LTOT.
Her request to be pre-allocated to London was declined and was allocated Dorset.
This is a catastrophic failure by the @UKFPO, who simply isn’t hated enough.
“…The doctor is the only professional capable of performing the core act that justifies the hospital’s existence: diagnosing the disease and establishing the treatment…. This functional hierarchy is not a social convention or an inherited privilege: it is a direct consequence of training…”
As a practicing spine surgeon who pours my heart into healing patients every day, let’s be real: Declaring healthcare a “right” isn’t noble—it’s a sneaky way to force doctors like me into servitude.
My skills, time, and labor aren’t yours to command. True rights protect freedom, not demand others’ sweat.
If healthcare’s a “right,” I don’t own my own hands anymore. Taxpayers lose their earnings, hospitals their property. It’s not care—it’s compulsion. A free society can’t survive treating humans as resources to plunder.
Bring back the free market in American healthcare to maximize access to care and undo the ACAs attempts to socialize healthcare in the US!
Sophy Ridge: "20,000 foreign doctors come to the UK every year, but we reject about 16,000 med school applicants, & this is because of money right? It's cheaper for us to import trained doctors from abroad rather than subsidise training in the UK"
It tells you everything that a US insurer looks at the NHS and is “impressed.”
Of course they are — it’s the dream scenario for any payer: a workforce that can’t leave, can’t negotiate, and delivers massive productivity for very low wages.
That’s not praise of UK doctors.
It’s an indictment of how much the system extracts from them.
I've been a doctor since 1991. I've seen enough of my colleagues kill themselves because of the stress of this work to have zero f**ks left to give in dealing with people who abuse and malign us.
I qualified in London, worked as a medical SHO until 1995, eventually completed GP training in 1999, worked as a GP, initially locum then partner, until 2012. Then moved to Australia and became a rural generalist. I now work predominantly in the emergency, ward and HDU of a busy remote hospital, dealing with patients with the highest morbidity on the planet.
I have seen medical practice evolve. There are no 80 hour weekends for internal medicine residents anymore, but the intensity of the work has increased, the complexity has increased, the expectations have increased, the blame dumping onto juniors has increased, the general mindless bullshit has increased and the pay and conditions have got exponentially worse.
Resident doctor in a busy hospital remains one of the physically and emotionally toughest jobs in the world. People who think it's a 'job like any other job' have no f***ing idea.
Pay the residents what they are worth - which is a lot more than the BMA is asking for - and improve their conditions out of all recognition or watch them leave the profession or leave the country.
Then all you whiners will be whining your pathetic little hearts out about how there is no-one competent left to look after you. And you will deserve it.
It's your choice.
The reason they train is the same reason they strike:
they entered medicine under the promise of a normal career, not a decade-long bottleneck with below-market wages.
Most countries don’t treat doctors like this.
The UK’s system is the outlier.
Full breakdown of why in the thread below.
https://t.co/N13K896cLB
The UK didn’t accidentally underpay its doctors. It built a system where long, low-paid training, high debt, and a monopoly employer function like indentured servitude. Other universal systems don’t operate this way. The NHS does because politicians designed it that way.