Un paraguayo estaba mirando el partido con su perro
Y cuando le ganaron a alemania se pusieron a festejar juntos
El bicho no entendia nada pero estaba feliz jsjs
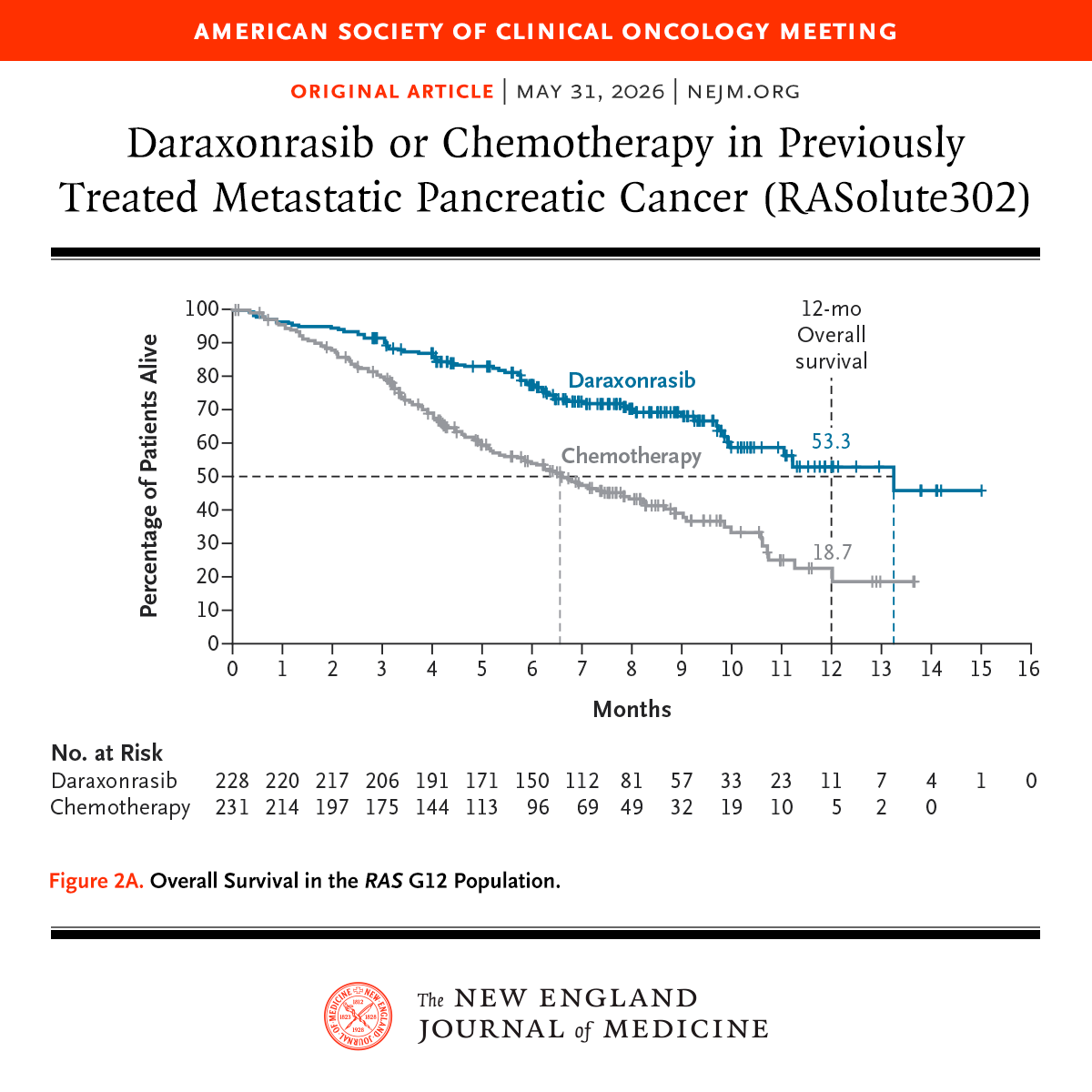
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
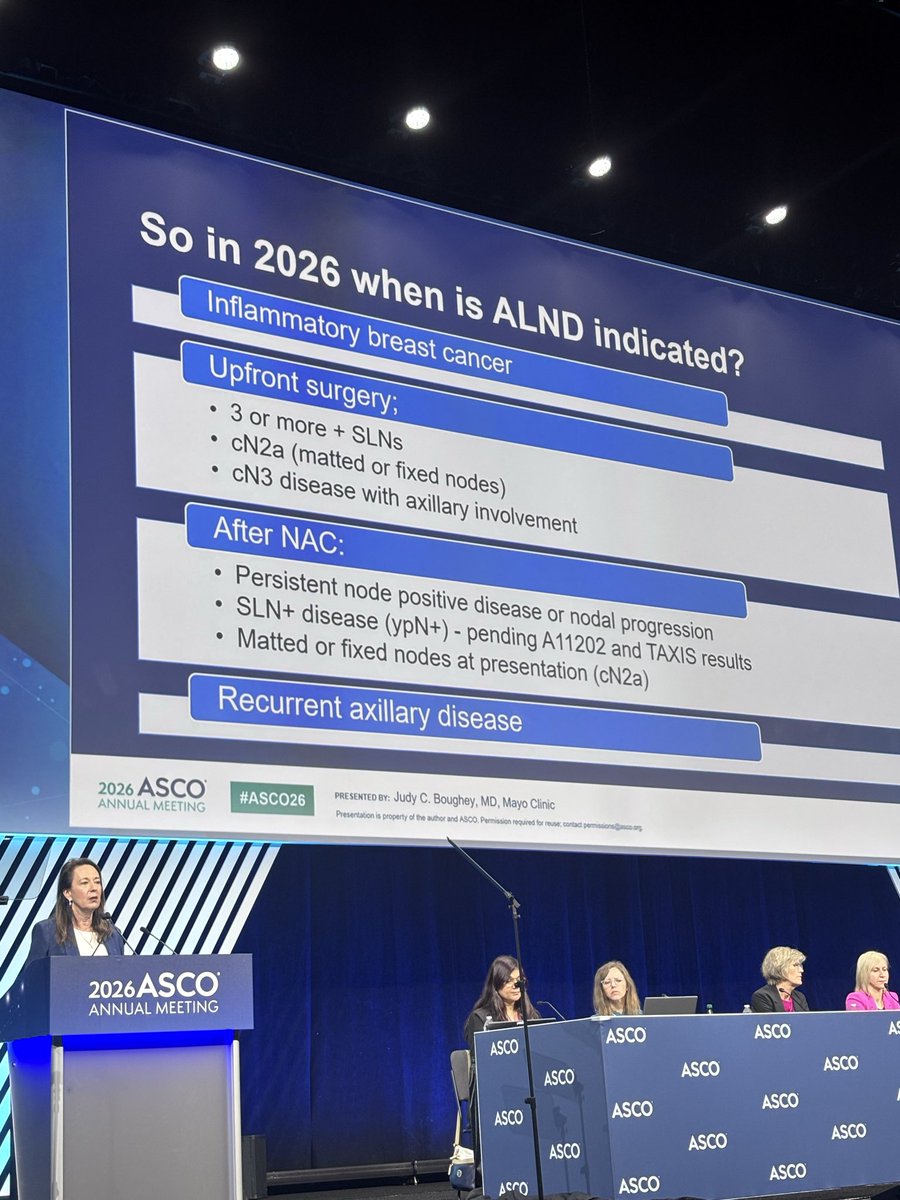
ALND indications in 2026 per Boughey at #ASCO26
1) IBC
2) 3+ positive SLNs
3) cN2a/cN3 upfront and after NAC, persistent nodal disease or matted nodes at presentation.
4) SLN+ (ypN+) still pending A11202 and TAXIS.
Evaluation and Treatment of Iron Deficiency for the Practicing Oncologist | JCO Oncology Practice https://t.co/OlPqUor0xf @JCOOP_ASCO@ASCO@OncoAlert one of the most common consults in General HemOnc Clinics
A ready-to-go OPD algorithm for adjuvant chemo in HR+/HER2– early breast cancer.
Clinical risk + tumor biology + Recurrence Score + age + menopausal status → clear, practical decisions.
Avoid overtreatment.
#BreastCancer#RecurrenceScore#OncotypeDX#PrecisionOncology
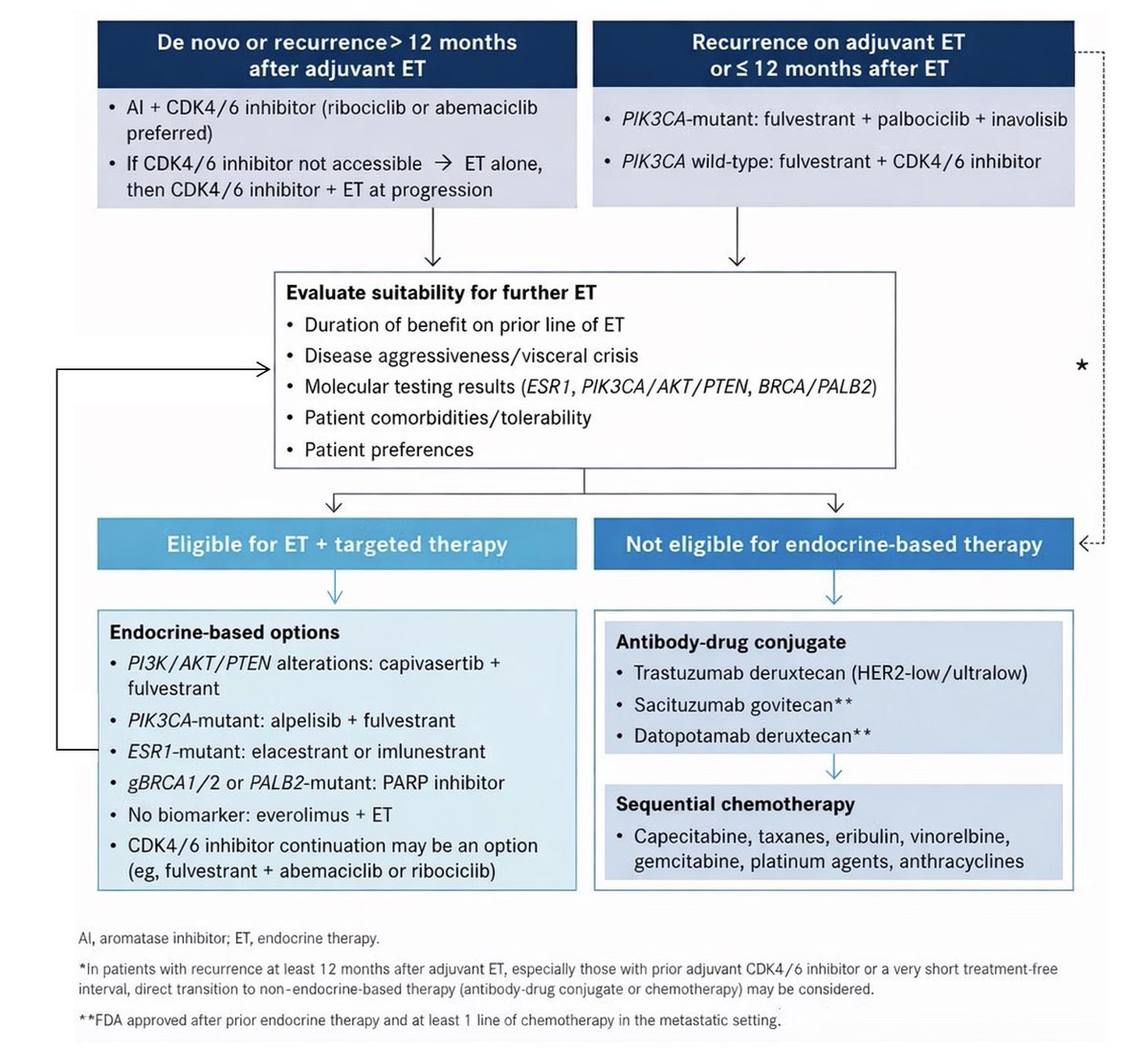
Algorithm of ET ± targeted treatment options after ET + CDK4/6 inhibitors. Some options are not yet approved— caution!
From Dr. Alessandra Gennari’s excellent discussion at #ESMO25👇
This distinction is important:
In HER2-positive mCRC, if a RAS mutation is present, T-DXd should be preferred.
If RAS is wild-type, either T-DXd or other anti-HER2 agents can be used.
Excellent summaries👇
HR+/HER2– metastatic breast cancer management is changing fast!
In this piece👇 @elmayermd and I share our perspective on how targeted agents, oral SERDs, & molecularly informed sequencing are reshaping decision-making
@DFCI_BreastOnc@OncoAlert
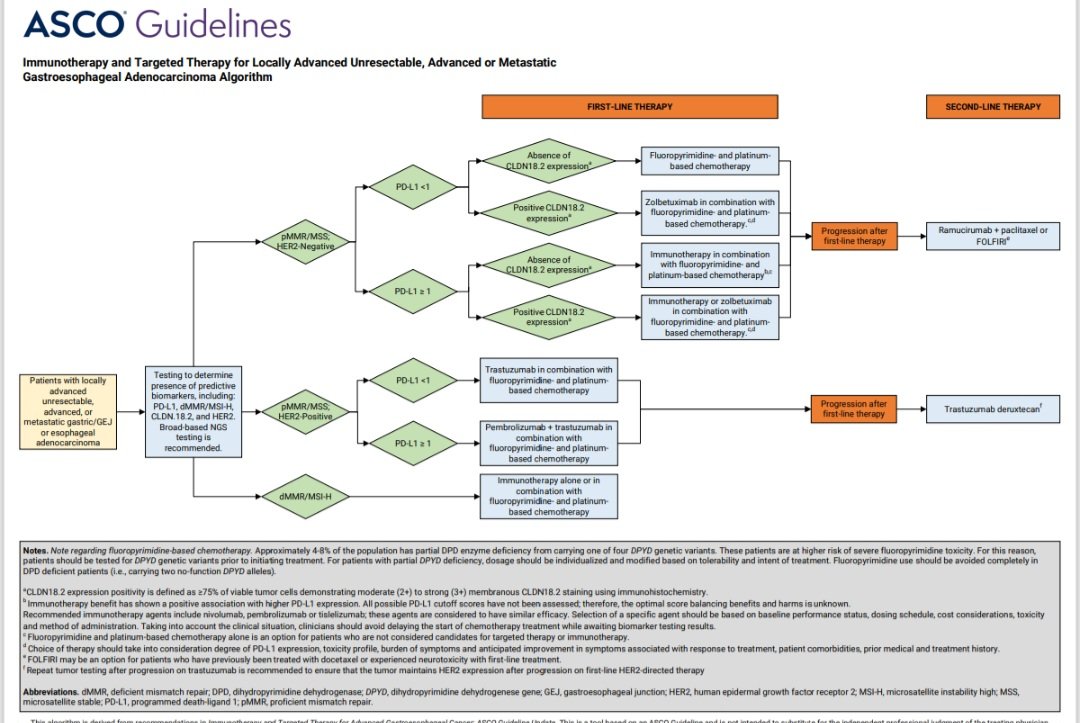
🚨 Gastric Cancer 2026 – Evidence That Should Change Practice
The new JAMA Review (Jan 2026) pulls together the trials that now define modern gastric cancer care. Here is the trial-led snapshot every oncologist should know 👇
🌍 Why this matters
Gastric cancer remains the 5th leading cause of cancer death worldwide, with most patients still presenting at advanced stages. Outcomes are now tightly linked to trial-backed biomarker selection.
🦠 Prevention evidence
• Community H. pylori eradication trial (Pan et al., Nat Med 2024) showed significant long-term reduction in gastric cancer incidence.
Prevention is still the most powerful intervention.
🔪 Perioperative and locally advanced disease
• FLOT4 – Established perioperative FLOT as the global standard (OS 50 vs 35 months).
• MATTERHORN – FLOT + durvalumab improved 2-year event-free survival (67.4% vs 58.5%).
• NEONIPIGA – MSI-H/MMR-deficient tumors showed striking pCR rates with neoadjuvant ipilimumab + nivolumab, challenging chemotherapy altogether.
🧬 First-line metastatic disease – biomarker driven
• CheckMate 649 – Nivolumab + chemo improved OS in PD-L1 CPS ≥5.
• KEYNOTE-859 – Pembrolizumab + chemo improved OS across PD-L1 strata.
• ToGA – Trastuzumab + chemo established HER2-positive standard.
• KEYNOTE-811 – Pembrolizumab + trastuzumab + chemo pushed median OS beyond 20 months in HER2+ disease.
• SPOTLIGHT & GLOW – Zolbetuximab + chemo improved OS and PFS in CLDN18.2-positive tumors.
🎯 Second-line and beyond
• DESTINY-Gastric01 – Trastuzumab deruxtecan improved OS in HER2+ disease post progression.
• RAINBOW – Ramucirumab + paclitaxel improved survival and quality of life.
• TAGS – Trifluridine-tipiracil showed modest but real benefit in later lines.
🤝 Supportive care is evidence-based
• Interdisciplinary supportive care trial – Early nutrition and psychosocial support improved OS by ~3 months, rivaling many systemic therapies.
📌 Take-home message
Gastric cancer in 2026 is no longer chemo-first.
It is trial-defined, biomarker-led, and multidisciplinary.
Skipping biomarkers or evidence-based sequencing is no longer defensible.
#OncoTwitter #MedTwitter
#GastricCancer #GI26
@ASCO@ESMO_Open@OncoAlert@myESMO
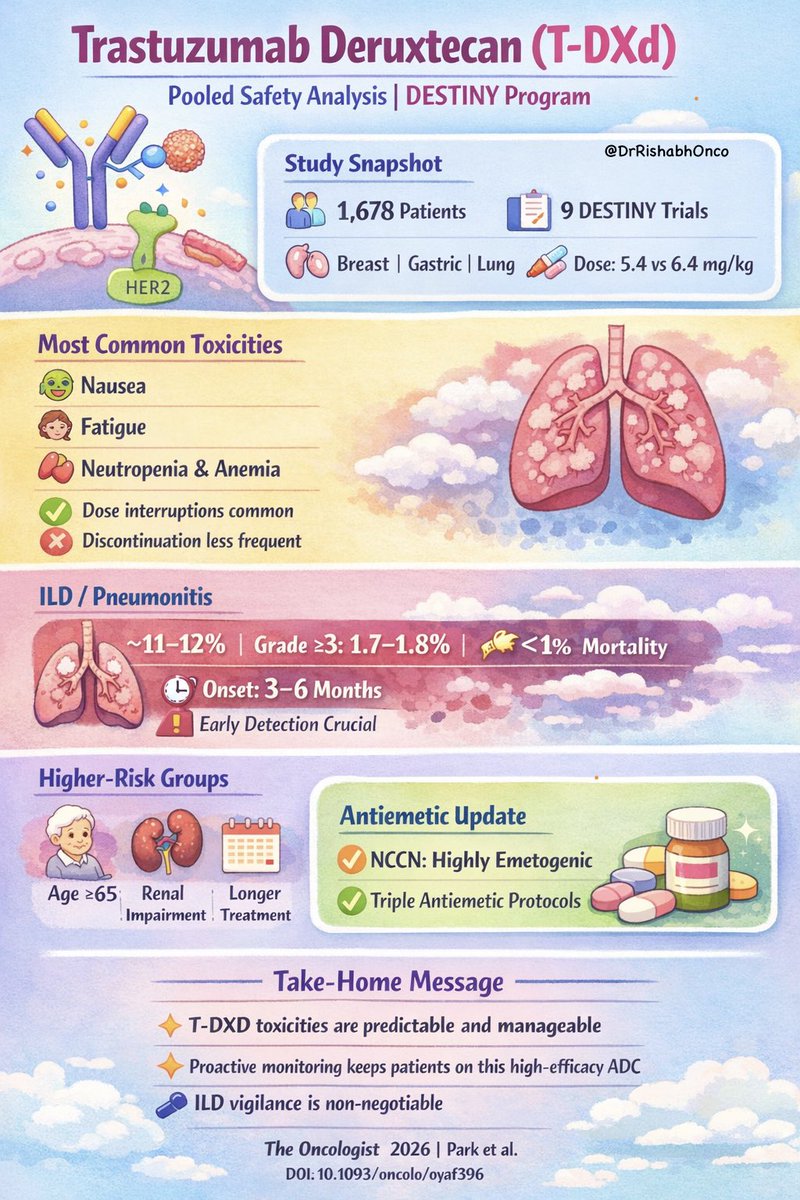
🚨 New pooled safety data for T-DXd across DESTINY trials
Largest safety analysis to date of trastuzumab deruxtecan (T-DXd) across doses and tumor types is out in The Oncologist 🧬
🔍 What was analyzed
9 phase I-III DESTINY trials
N = 1,678 patients
Breast, gastric, lung cancers
Doses: 5.4 mg/kg vs 6.4 mg/kg Q3W
📊 Key safety signals
•Most common TEAEs: nausea, fatigue, neutropenia
•GI + hematologic toxicities dominate, mostly grade 1–2
•Dose modifications common, discontinuation relatively infrequent
🫁 ILD remains the key concern
•Adjudicated ILD: ~11–12% overall
•Grade ≥3 ILD: ~1.7–1.8%
•ILD-related mortality: ~1%
•Median onset: ~3–6 months → vigilance over time matters
👵 Who needs closer monitoring
•Age ≥65 years
•Renal impairment
•Longer treatment duration
💊 Practice-changing nuance
•NCCN now classifies T-DXd as highly emetogenic
•Proactive triple antiemetic strategies likely needed upfront
🧠 Bottom line
T-DXd toxicities are largely manageable, but require anticipation, early intervention, and structured monitoring, especially for ILD and nausea, to keep patients on this highly effective drug.
#OncoTwitter #MedTwitter #BreastCancer #HER2 #ADC #Enhertu
@DFCI_BreastOnc@stolaney1@PTarantinoMD@OncoAlert@ASCO@myESMO@ESMO_Open