What REALLY makes a good oncologist? in @JCO_ASCO
After 10 years and 203 JCO essays, one thing became clear: expertise alone isn’t enough.
Patient-centered care.
Clear, authentic communication.
Emotional intelligence.
And the harder work
Showing up again and again.
Openness to uncertainty.
Carrying the burden of cancer care.
Continuous growth.
Clinical competence is expected
Human connection makes the difference.
Science treats disease.
Presence treats fear.
https://t.co/g9hGjSLpGu @OncoAlert
Thrilled to share our new ASCO Global Guideline on Geriatric Assessment 🌍👵👴 — supporting cancer care for older adults in resource-constrained settings.
Published in @JCOGlobalOncol ➡️ https://t.co/bQpp9DleLO
#gerionc#globonc@ASCO
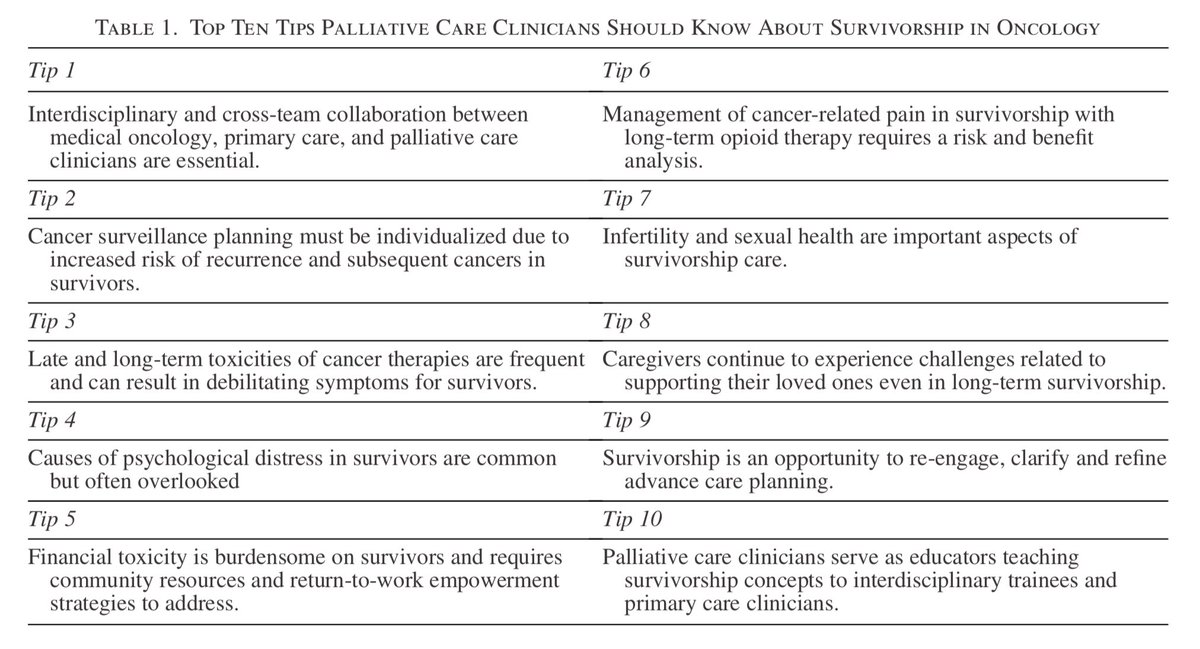
Top 10 Tips for Palliative Care Professionals to know about Cancer Survivorship Care - an excellent paper by @realbowtiedoc published in @PalliativeMed_J, with some key take home messages as summarised in this Table (see https://t.co/46QuS2yu6c for the full article).
Mirtazapine for breathlessness?
Evidence does not support its use.
In a similar fashion to using Clonazepam for pain it is probably helpful in a small number of people who have anxiety and poor sleep associated with their symptoms.
https://t.co/KrtP3C0VvH
Terminal agitation - A palliative care thread 🧵
This is not a thread on delirium near end of life.
Although severe delirium can lead to agitation, almost all delirium in the last days of life can be managed with non-pharmacological support or small doses of medicine
New therapeutic options don’t come along often in palliative care. When they do there is often understandable hesitancy to introduce these into practice. Clonidine is a good example of this so I wanted to explore more with this thread 🧵 👇