I’m pleased to share Mayo Clinic has announced a strategic collaboration with @Microsoft to develop and deploy a frontier AI model designed specifically for healthcare. Read more: https://t.co/I6RGCtR8MF
Extremely proud of friend, colleague, and boss, @TorBiering, for receiving the 2026 Danish Society of Cardiology & Danish Heart Foundation @cardio_dk Research Prize! This award is in recognition of his massively innovative, outstanding research efforts - Tor, you’re the man!
What do The Dave Brubeck Quartet and Advocate Health have in common?
At Advocate Health, it used to take pharmacy staff up to 25 minutes to fill out a set of prior auth questions.
Now, they only Take Five 🥁
Between rooms. On rounds. Walking the corridor outside an OR. Charting one-handed during a phone call. This is where clinical questions happen.
Today we're launching Voice Mode. OpenEvidence is the first multimodal medical AI: physicians can type, speak, or listen, on the same evidence base.
The clinician asks a clinical question out loud. Voice Mode waits when you pause, stops when you interrupt. The answer comes back concise, peer-reviewed, and verifiable against the source.
Conversation with a colleague. That was the bar.
For years we've focused on the intelligence: curation, retrieval, citations. Voice Mode is the interface catching up to where physicians practice.
The evidence quality doesn't change with the modality. Voice answers are shorter and shaped for listening; the references and the full written form stay in the conversation.
Voice Mode is now in OpenEvidence web and mobile.
Until now, physicians using AI in clinic had to assemble the patient’s context themselves. Allergies, comorbidities, medications, prior procedures, copy-pasted in from the chart.
Today we’re announcing a partnership with @CedarsSinai. OpenEvidence now works directly inside Epic, drawing on the patient’s full record and interpreting the medical literature through the lens of that specific patient.
Cedars-Sinai is the first academic health system to deploy patient-aware clinical intelligence at enterprise scale. The clinician asks a complex question in natural language. The answer reflects both the best available evidence and the patient in front of them.
Patient data is never stored after the clinical session or used for any other purpose.
We need awesome doctors who can help develop AI doctors to make AI scalable for all primary care, chronic disease care, and parts of specialty care we call "multi-specialty primary care"! AI allows for this oxymoron. Make a difference globally
It was a pleasure to welcome Dr. Robert W. Yeh as our 16th Peter M. Yurchak Visiting Lecturer this last week at MGH.
Thank you for your wisdom related to career building, future directions for device innovation, and much more!
It was a privilege to know Dr Braunwald for several decades . We collaborated on dozens of HF trials , from the planning and implementation of the NHLBI HF network, the STICH trial, and others. He was always generous with his time whether writing a letter of congratulations or offering thoughtful advice with a simple call. Despite his unmatched leadership and contributions to cardiovascular knowledge , research, and education, he often said his greatest joy was mentoring the hundreds of individuals he influenced directly and indirectly.
Truly the GOAT ( greatest of all time ) in our generation.
Later in life , he said Chris, you can call me Gene; I replied thank you Dr. Braunwald.
Rest in peace, Dr Braunwald. We will miss you .
Chris
The cardiology community has lost a giant. We honor the extraordinary legacy of Eugene Braunwald, MD, MACC, a visionary leader and pioneer whose outstanding contributions shaped the foundation of cardiovascular medicine as we know it today.
Read more: https://t.co/uaC2n4m5gD
The cardiology community mourns the loss of Dr. Eugene Braunwald, a towering figure whose work shaped modern cardiovascular medicine.
From foundational discoveries in heart failure to Braunwald’s Heart Disease, his legacy will guide generations to come.
A true giant in our field.
Heart of the matter new episode🎙️ Best Practices for Site-Based Research (Part 3)
Challenges, opportunities, and building successful research sites.
#HFC 💙 https://t.co/0btLfDOWuF
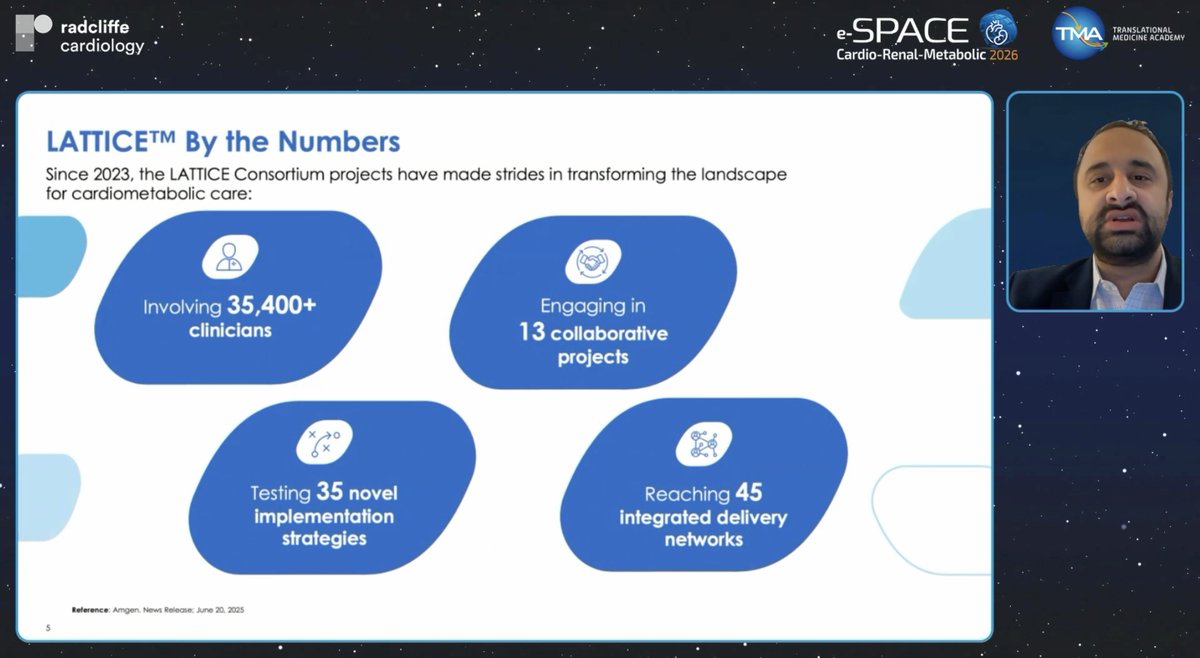
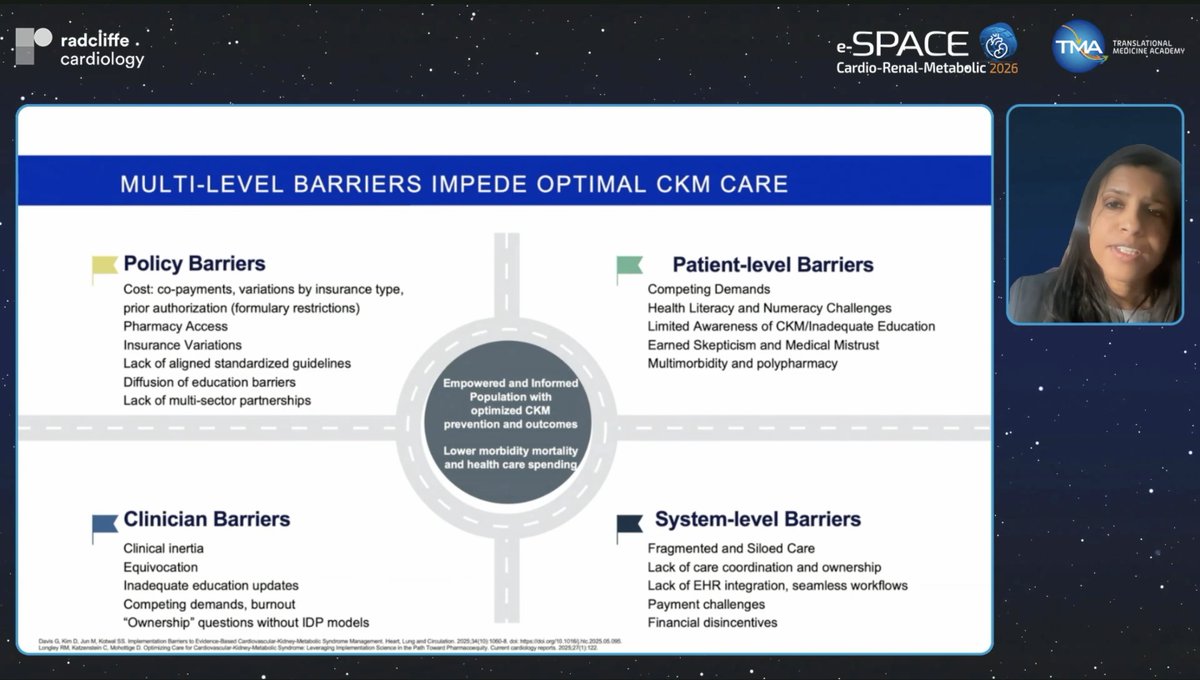
LIVE | e-SPACE CardioRenal Metabolic 2026
Plenary Session 10 Wrap-Up
We conclude From Prevention to Shared Decision-Making and bring e-SPACE Cardio-Renal-Metabolic 2026 to a close after two days of outstanding science, collaboration, and forward-thinking discussions across the cardio-renal-metabolic continuum.
Thank you for being part of the journey.
Missed a session or want to revisit the highlights?
e-SPACE CRM 2026 is now available on demand.
Watch anytime, anywhere: https://t.co/favdWnIEW5
#eSPACECRM2026 #CardioRenalMetabolic #CRMScience #IntegratedCare
An oncologist and a rural family doc can ask the same clinical question and need fundamentally different answers. Different structure, different depth, different follow-through. One-size-fits-all has never described how medicine works. It shouldn't describe how clinical AI works either. Today we're releasing Dotflows. Easiest way to explain is by example.
- Type ".discharge" and paste an exam note. Structured inpatient discharge summary, seconds. Type ".avs" and any query becomes a patient-facing after visit summary with instructions and return precautions.
- Type ".prior_auth" and get an insurance appeal letter grounded in medical necessity. (The fact that physicians built this one on day one tells you everything about the state of prior auth.)
- Type ".succinct" and every response gets compressed into the clinical shorthand you actually think in. It's been run over 3,000 times. The physicians have spoken, and what they said was "less."